Sodium 139 mmol/ml (range 133-145 mmol/ml) Optimal 142 (a little low but Good)?
Potassium 4.1 mmol/ml (range 3.5-5.5) Optimal 4.2 or higher (a little low but Good)
Calcium 9.4 mg.DL (range 8.4-10.6) Good
Creatinine 0.6 (0.5 - 1.2) BUN 8 (6.22) ALT 26 (5-40) AST 24 (10-37) Kidneys and Liver Good
MORE IMPORTANT TESTS
These tests were done. Symptoms of high anxiety (we both have had/are having akathisia reaction which is anxiety on steroids), No menstrual cycle, Menorrhagia (heavy menstrual bleeding)
BLOOD
Cholesterol 171 (110-200 mg/dl) Good
HDL 43 (40-59 mg/dl) OK
LDL 82 (50-99 mg/dl) OK
VLDL 45 (8-30 mg/dl) HIGH
Triglyceride 227 (40-149 mg/dl) HIGH
Hemoglobin A1C 4.8% (4.8-5.7) Borderline Low - Not diabetic
Average Glucose 90 (91-123 mg/dl) LOW (suspicious!)
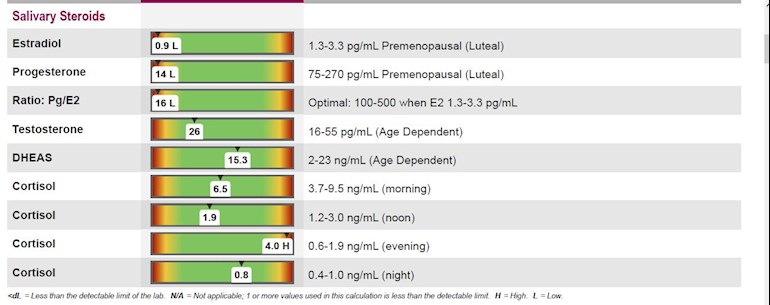
17 OH Progesterone 25 ng/dl (no range) OK But oddly Low reading
DHEA-S 652.6 mg/ml (84.8-378.0) VERY HIGH
Estradiol 29 ng/dl (no range) VERY LOW
Testosterone 62 ng/dll (3-41) HIGH
FSH mIU/ml 6.0
LH mIU/ml 6.9
Good but not ovalating properly and had an Overary Cyst 6 months ago.
Prolactin 18.1 (4.8-23.3 mg/ml) Good
TSH 0.58 (0.27-4.2)
Free T4 1.2ng/ml (0.9-1.8)
OK So I suspected Adrenal Fatigue, Hypothyroidism of so sort and we both suspected POCS.
So I ordered the saliva test, we have ordered a thorough thyroid test, and we ordered a glucose fastening test (and B12 as for some reason this was not on the thyroid test)
11.5 uIU/mL )fasting. Fasting: 2.0-19.6
154 uIU/mL after 30 minutes. 30 Minutes Post Glucose: 6.0-86.0
VITAMIN B12
466 (pg/mL) Range: 200-1100
Adrenal Fatigue (phase 6 now 3D) and a Thyroid issue, the new panel will tell us everything.
Any other suggestions would be most welcome here.
I did the adrenal fatigue Dr Peatfield protocol years ago, as I too had low cortisol with high testeterone and DHEA but being male (and maybe ignorant) didnt bother with the others.
Still I found 20mg a day with hydrocoritsol worked really well before starting on NDT thyroid (Take 2 grains in summer 3 grains in winter).
But we might as well start treatment now (as the thyroid results will take a couple of weeks at least anyway), but I was just wondering based on the results above what you would do?? Any suggestions??
If you think Cortef is a good idea here (can someone PM me where to get it in the States. I know where to get it here but oddly enough comes from the States and wont deliver domestically). Is the newer Ortho Molecular Products Adren-All Capsules any good? They contain a good mix of Bovine adrenal 220mg, as well as They both have Vitamin A, Vitamin C,Vitamin E,Niacin,Vitamin B6, Vitamin B12 and Pantothenic Acid. They both have Eleuthero root, Rhodiola Root, Schizandra Berry Extract and licorice Root Or Adrenavive iii, Or is this not strong enough and hydrocotrisol is needed (which would be my prefered option unless we cannot get it.
I am never sure about Progesterones and oestrogens as they can be addictive, which is why it can be very difficult for some women to stop their prescriptions, but I could be over reacting here, or is that needed here despite DHEA-s and testosterone being high
Any advice on this would be great.
Written by
Crunchieeagle
To view profiles and participate in discussions please or .
Insulin Resistance test fail. I am not keen on Metformin especially as the Vitamin B12 is lower and needs supplimenting maybe with methyl folate or 5-MTHF not Folic acid anyway.
However I have read and seen alot of good things for POCS with Myo-nositol and D-chiro-inositol. Again only i have heard and read but not experienced is 2000mg Myo-inositol with 50mg of D-chiro-inositol, or even just 500mg of D-chiro-inositol to begin with. I think adrenal support wiill help here too? Dont worry if no one had had experience here, but it is the adrenal issue I need advice on.
The typed out info is from the blood. I wanted to do a cortiol test but did the full saliva at the same time. So blood and saliva were done within two weeks of each other but she is not ovalating anyway. Is definitely stuck in the pre- LH phase. Docotr of course thinks there is nothing wrong hence the extra tests. The full thyroid panel will take another couple of weeks mate.
Thanks Helena. The bood panel was already done, and doctor siad there no problems. So I disagreed and thought of POCS andrenals and Thyroid will be out of sync. I do believe 100% cortisol needs to be done with saliva, but it was interesting to get a comparison.
PCOS no.1 symptom (but not always is insulin resistance). She failed that (positive).
It is interesting what you say about saliva v blood. Even STTM say blood is better for adrenals?? Estrogen was very low in blood too and progesterone was not tested.
Anyway maybe the problem being as progesterone is ss low and estrogen even lower but testosterone is midrange, and the DHEA is high in the range. There is something funny going on. I wonder if that is related to POCS as that would normlise anyway I feel. Then mabe her soritsol would improve anyway?
Like I said it was that reason, we could just go progesterone creams but I have heard that can be addictive so an adrenal cortex supplimentation instead?
But that is entertained here instaed of adrenal cortex.?
Hi, sorry you haven't had any replies going into your results. I did find these a bit confusing. It threw me off that in the post you say "I'm male", but I've only just seen from the comment these are someone else's results?
Cortisol is always difficult to get much discussion going about, as it's harder to figure out than thyroid things. This is definitely quite a bad result, and sounds like you know that. Although the chart you've got makes it look a lot worse than it is, because the 4 results are shown within their own ranges, not against the same axis as they would be in a graph. Your results are out of the standard shape, but not far far out as they look in the chart. Morning is still the highest result and nighttime is the lowest.
Looking more carefully, 3 of the results are pretty optimal, and only 1 is very wrong. This does make me concerned there has been an error. I had a result very similar to this earlier in the year. It turned out one result had been contaminated because I'd eaten half an hour before. I know it was an error because I complained and got a retest. Some places with great customer service will give you a retest for free if a result looks like a mistake. I would consider a retest if it's possible in the budget even if you aren't offered one.
With the DHEA if you believe the saliva are fine, but if you believe the blood there's an issue. I don't know which of these is the most trustworthy, but I'm inclined to trust the saliva as that test is recommended. My own blood and saliva have always matched. High DHEA is semi-good news in that it suggests an early stage adrenal fatigue, because later in the process the body isn't able to maintain it.
I have looked into my own adrenals off and on for the 6 years I've been ill. This year I found they had gone from looking horrible when I was very very ill, to looking very nice now that I'm closer to having my thyroid right. I concluded that the adrenal fatigue was really just a marker of other illness. I didn't take any adaptogens, gland extract, or DHEA prior to the improvement.
Although I do have pretty good lifestyle factors, meditate, rest a lot, am not stressed, and eat a good diet, worked on my insomnia and now sleep well, exercise gently, vitamin tests fiid. These things are all worth doing whatever you decide with more treatment-y treatments. They are more effective, really, than others.
Unfortunately I'm not able to comment on the sex hormones, but obviously they are very bad. It might be worth making a new post about them later, and making clear in the title it's about sex hormones, because passers-by might not be realising. Many people here can interpret thyroid and basic vitamin results, but it's harder to find good analysis of other results.
On the saliva test progesterone is well under range but the DHEA is borderline high. The blood tests (which you can argue both ways for saliva and blood IMO) but cortisol for saliva is the key, and it could be an error.
Let's assume it is not (as these tests are damn expensive), but we can repeat later after PCOS treatment starts with myo and d-chiro-inositol which with alot of people works better than metformin (and believe me her doctor said everything is normal despite ovary cysts), so is next to useless and unlikely to prescribe.
Do you know anyone has taken progesterone treatment as i hear it is addictive. Is it better than 250mg bovine adrenal cortex we have delivered tomorrow, can both be used?
Is it worth a two week trial of progesterone? She is not ovulating so it doesnt really matter when we start but FSH is in good shape
We have methyl type folic acid and Vit B12 too.
I am pretty sure when we have the PCOS better, and cant wait for the thyroid results, as this will tell us alot, but I suspect thyroid problems and PCOS are the route cuase hear but I want her cortisol (not in perfect shape) but in a good shape before thyroid is strated very slowly, if that does indeed come back. We have ordered a huge thyroid profile with exerything with cream on top. So we should get a good picture.
Whilst I agree cortisol is not horrendous I still think Morning Cortisol should be higher but has insomnia in any case because of PCOS and other issues, so I guess that doesn't help.
Thanks for your answer on your own experiences. Hopefully the progesterone levels will rese when insulin sentitivity is sorted, but to help that I was thinking ACE but now possibly progesterone such for a very short while as it does have its side effects.? What do you think (Don't worry I wont do what you say, but would appreciate your knowledgable input here).
Many Thanks for the reply.
Just wondering what you think to my questions?
(FWIW I had very high DHEA's and tesosterone too, and manage to get cortef (and my cortisol level we in check but always on the low side IN THE RANGE for the first 3 and after 3 months on 20mgs in total a day got everything back in check and myself am on 2 grains of Thyroid S in the summer and 3 in the winter).
Thanks to a lovely treble dose of radiotherapy by the nhs without my consent I’ve no estrogen and no progesterone.
I do use the progesterone cream with no side effects.( The sweats were a nightmare) Also the only natural thing I could think of to increase estrogen was organic soya milk( I try to get non gmo ) that definitely helps.
If she does not sleep well she could consider melatonin in small pieces say 1 mg to start with. It is used to lower dhea. So if the blood is right it need lowering. If the saliva is right it’s mid range so a small amount should be ok.
I have no dhea so take pregnenelone and I am hoping my testosterone will increase with that.
Sorry I can’t be more exact but I’ve never seen so different results before.( and I’ve seen hundreds of adrenal results).
Good luck and just message me if I can help further. My specialist is amazing and I will be speaking to her soon so I can add an odd question in.
This is the ‘classic PCOS’ patient, and also the most common. The culprit in the development of classic PCOS is insulin resistance – when the body becomes less responsive to insulin and blood sugars become imbalanced. High insulin and leptin impede ovulation and stimulate the ovaries to make testosterone.
What’s the cause? Insulin resistance is caused by obesity, sugar intake, smoking, trans fats, and environmental toxins.
Do you have it? Ask your doctor to check your fasting insulin and fasting glucose levels. You may also have elevated LH (luteinizing hormone) or cholesterol levels. You may be overweight, or normal weight with a history of extreme dieting or eating disorders.
So we are going to take myo-inositol and a little d-chrio inisitol for insilin insensitivity. smartfertilitychoices.com/i...
2. Immune Related PCOS
This second type of PCOS is due to chronic inflammation, which can be the result of many different causes. This inflammation impedes ovulation and disrupts hormone receptors, stimulating adrenal gland androgens like DHEA. Women with family or past medical history of other immune dysfunctions, like autoimmune conditions, may be more likely to develop this type of PCOS.
What’s the cause? Immune system dysfunction causes chronic inflammation that eventually leads to elevated androgens. Blood tests for inflammatory markers like CRP, ESR, vitamin D deficiency, thyroid antibodies and food sensitivities/allergies should be evaluated. You may also have elevated DHEA-S, an adrenal androgen.
Thyroid results to come, but we are chekcing Hashis with this too.
Thats why i though maybe adrenal cortex to bring it down?????? Her corisol balance may need improving (depending if the 3rd result was an error but for now i am assuming not and will rest in 3 monthsafter adrenal support.
3. Post-Pill PCOS
For most women, a slow-to-restart period after stopping the birth control Pill will normalize within the first six months, but for others the suppression can last years and require treatment.
What’s the cause? After years of the Pill hijacking your hormones, the body has a hard time producing its own Estrogen and Progesterone again, making ovulation natural or non-existent.
Do you have it? Though you may have had regular periods before taking the Pill, since coming off you’ve had an irregular cycle and perhaps have battled with acne. You likely have elevated LH (luteinizing hormone), and potentially also have elevated prolactin, though lab tests may be normal.}
Her Ovaries are in good shape after the cyst from ultrasound. However low FSH, LH Estrogen and Progesterone, after being on the pill for years. Thats why I thought Progesterone maybe a good idea (even very short term)??
4. Environmental PCOS
The final, and perhaps simplest, type of PCOS is one where there is a single environmental (or other hormonal) imbalance that is interfering with your body’s ability to ovulate on a regular schedule. It can take a bit of trial-and-error to determine the true cause of PCOS in these cases, but once found, patients respond very quickly to treatment.
What’s the cause? In patients who are sensitive, certain food choices can play around with the body’s ability to ovulate. For example, I have seen patients begin to ovulate regularly after taking soy out of their diets, by properly supplementing a strict vegetarian diet, or by removing artificial sweeteners. I also include thyroid disease in this category, because hypothyroidism can disrupt normal ovulation.
Do you have it? If you don’t fit into the category of the other types of PCOS, or don’t respond well to regular PCOS treatments, it may be time to have a look at environmental factors or the thyroid.
Of course, there can be overlap between these categories, and the diagnosis is not always black and white.
We are checking hash's, magnesium, full thyroid, Iron everything, so we will get the full picture here. It was a £300 test, but will be worth it, as once we know if where the problem is, we can act on that bit. For example if it is low thyroid and not hashi's or the other way around we know what to do.
I know doctors dont like talking about other patients (tried it many times myself), but it would be great if you did find any info out.
What i dont understand is if you have PCOS, why they dont test FOR everything first to find out which one it is?? Of couse money, but then they end up spending more omeney finding the route cause???
We have founf out a methylation problem too (MTRR) so we are adding in B12, and also Mitochondrial function, so CoQ10 and Vitamin B2 too (and some folate through a Vitamin B complex).
Then if the thyroid results i feel maybe more accurate so we can try that again. x
Content on HealthUnlocked does not replace the relationship between you and doctors or other healthcare professionals nor the advice you receive from them.
Never delay seeking advice or dialling emergency services because of something that you have read on HealthUnlocked.