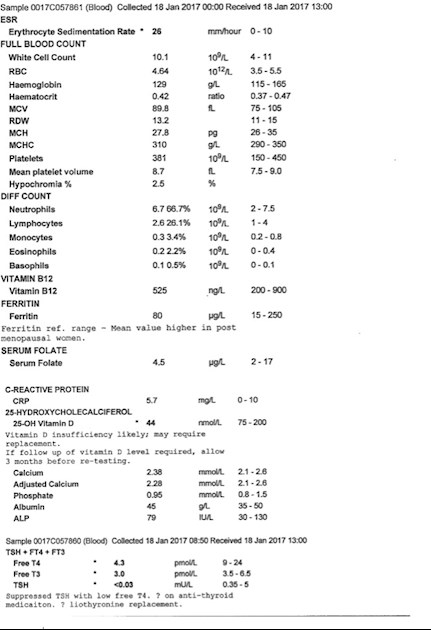
So I am stumped. I really don't know what to do. With my blood tests previous to this I was over the range for T3 but I was starting to feel better. I was told "You are over medicated whatever you feel. If you only feel well with high FT3 then you will have to decide whether the increased risks of developing osteoporosis and atrial fibrillation are acceptable in order to feel well today" so I, of course, decided to lower my T3. I have since had another flair up brought on by a long haul flight so I thought I would get a full blood panel to see what was going on. The results in the attached picture is on 3 grains ndt and 25mcg T3. Below are my past blood panels for comparison.
I can see I need to raise vit D, and B12 again. (Would this have anything to do with the rapid hair loss?) Any suggestions I am all ears. Feeling so frustrated, I just don't know what to do. Sorry for the negative tone! R xx
BLOOD PANEL FROM SEPTEMBER 2016
TSH0.3mIU/L0.35-5.00
Free T4 11 pmol/L0 - 24
Free T3 6.6 pmol/L3.5 - 6.5
Serum total 25-OH vit D 100nmol/L (75 - 200)
Vit B122000ng/L200- 900
Folate21.4pg/L2 to 17
Urea 4.2mmol/L2.5 - 7.8
Creatinine48 pmol/L49 - 90
eGFR result/1.73m2<60
Sodium139mmol/L133 - 146
Potassium4mmol/L3.5 5.3
Calcium 2.29mmol/L2.10 -2.60
Adjusted Calcium2.25mmol/L2.10 - 2.60
Albumin42g/lL35 - 50
Phosohate1.01mmol/L0.80 - 1.50
ALP59IU/L30 - 130
GENOVA BLOOD RESULTS NOV 2016 On 2 grains of NDT and 50mcg T3
TSH0mIU/L0.40-4.00 mIU/L
T4 Total 53nmol/L58-161 nmol/L
Free T4 8.5 pmol/L11.5-22.7 pmol/L
Free T3 8.9 pmol/L2.8-6.5 pmol/L
FT4 : FT3 Ratio 1Ratio 2.0-4.5 Ratio
RT30.14nmol/L0.14-0.54 nmol/L
Anti-Thyroidperoxidase abs <20 IU/mL <40
Anti-Thyroglobulin Abs <12IU/mL <35
Written by
Rhsana
To view profiles and participate in discussions please or .
The blood tests used is for the use of levothyroxiner alone so I don't think when on anything other than levothyroxine that our bloods can 'fit' into these ranges.If we take T3 only our T4 will be very low and T3 high as we are not taking T4 and our thyroid gland will be producing very little or none. I shall give you a link which may be helpful. This doctor (below) only prescribed NDT or T3 - never levothyroxine. (amended link below)
The potential harm from the use of thyroid hormone has been grossly exaggerated by the endocrinology specialty. Despite this, patients and their doctors should exercise caution to avoid thyroid hormone overstimulation. They can best do so by ignoring the endocrinology speciality’s exaggerations, and seeing the potential for harm with proper perspective.
Needless Worry Over Potential Harmful Effects of Thyroid Hormone
The three main potential harmful effects from the misuse of thyroid hormone are bone thinning, heart problems, and acute adrenal crises.
Osteoporosis. Through the 1980s and 1990s, doctors forced
millions of patients’ to keep their thyroid hormone doses too low
in order to avoid causing osteoporosis. In the early 1990s, studies
began appearing in journals showing that TSH-suppressive doses
of thyroid hormone don’t cause excessive bone thinning, and certainly
don’t cause osteoporosis or an increased rate of fractures.
For years, I’ve (JCL) talked with bone density radiologists
about the potential for bone thinning from the use of thyroid hormone.
Some have chuckled over the absurdity of the endocrinologists’
belief that TSH-suppressive doses of thyroid hormone cause
significant bone thinning, osteoporosis, or an increase in fractures.
Bone density tests of our own patients have shown that those
taking higher-end thyroid hormone doses usually have higher bone
density. The main cause of their higher bone density is that their
thyroid hormone doses are high enough to enable them to exercise
vigorously enough to thicken their bones. And, of course, their
wholesome diets and nutritional supplements also contribute.
It appears that the conventional endocrinologists’ scientifically
false belief that TSH-suppressive doses of thyroid hormone cause
osteoporosis has actually contributed to bone thinning among patients.
Those restricted to T4-replacement therapy usually are too
weak and fatigued to exercise vigorously. Their low physical activity
level has undoubtedly caused progressive thinning of their
bones, as well as deterioration of their health in general.
If a patient already has osteoporosis when she begins using thyroid
hormone, caution is prudent. If she hasn’t recentlly had a bone density
study, she should ask her doctor to order one. She should ask him to order
follow-up studies at intervals, perhaps every sixmonths. She may have
to teach the doctor that, despite the opinion of conventional endocrinologists, we absolutely cannot accurately infer from a TSH level the effect of a dose of
thyroid hormone on bone density. If the doctor wants to know the
effect, he should measure it directly by ordering a bone density
study.
When the patient’s dose of thyroid hormone is high enough to
enable her to exercise, she should do “bone-jerking” types of exercises
to tolerance each day. She should also make sure she gets
enough nutrient complex and protein each day to help thicken hbones. The complex we take includes the nutrients listed in Table
2.
Heart Problems. “You’re going to have a heart attack and
die!” is the warning many doctors give their patients when they ask
to be treated with desiccated thyroid—and especially if they ask for
T3. (If you haven’t read the Foreword to this book by Vicky
Massey, LMP, you may find interesting her experience with a doctor
who bellowed this warning at her.) Where these doctors get this
idea is a mystery, but they certainly don’t get it from the scientific
literature.
The belief of these doctors that patients using desiccated thyroid
or T3 run a high risk of heart attacks is clearly ignorance. Still,
though, it’s prudent for each patient to take reasonable precautions
when using thyroid hormone. We recommend that each patient at
least get a baseline EKG before starting to use thyroid hormone. If
the patient’s doctor has any doubts about the health of her heart, a
consultation with a cardiologist is wise. We’ve referred many patients
for cardiac consults before they began taking thyroid hormone.
Rarely, a cardiologist has recommended that the patient only
cautiously increase her thyroid hormone dose. Never has a cardiologist
reported to us that a patient should not use thyroid hormone.
Most patients with heart disease can safely use thyroid hormone.
In fact, using the hormone is likely to improve the patients’
heart disease. These patients, however, should use thyroid hormone
cautiously. And they—just like every other person who takes thyroid
hormone—should have a wholesome diet, take a full array of
nutritional supplements, and get regular aerobic exercise to tolerance.
If a patient has compromised heart function, her initial dosage should
be low enough to avoid aggravating the heart condition.If her doctor finds
that she tolerates the dose well, he should guide her through small dosage increases until she reaches her optimal dose. He must monitor her each step of
the way using all appropriate procedures to ensure her safety.
Recently, endocrinologists have warned that TSH-suppressive doses of thyroid hormone increase the risk of atrial fibrillation by 33%. A number of studies
showed that a certain set of people who had low TSH levels had a higher incidence of atrial fibrillation (see Figure 3).
But don’t conclude from this finding that if you take a dose of
thyroid hormone that suppresses your TSH level, you’ll have atrial
fibrillation. What endocrinologists—the main doctors who warn of
this risk—don’t bother to tell you is that these studies were done on
elderly, sedentary individuals. In fact, in some of the studies, the
patients were bedridden in nursing homes. In none of the studies
did the researchers control for a heart-protective diet, nutritional
supplements, or cardiovascular exercise to tolerance. The patients
appear to have been in such poor health that they may have
developed atrial fibrillation if they drank too much coffee each day.
It’s ludicrous and outrageously wrong to conclude that the results
of these studies apply to healthier people using TSH-suppressive
Hi shaws , thank you so much for your reply. I can't seem to get to a page on that link? I had my doubts about that statement (though I believe it was meant well) so I started to look for research that backed it up... whereI have found further statements to the same degree as that one, none of these can be backed up by any conclusive evidence. I would like to try a T3 only regime - this has come about because I misplaced my NDT and had to wait about 2 weeks to receive my next prescription, so I have been using T3 only now for about a week and I have to admit, I'm feeling a little better for it. Is it possible I just can't tolerate the T4 or possibly the fillers in NDT? or perhaps its just a placebo effect. either way I would like to give a T3 only regime a try to see how that goes, do you have any experience with that? Thank you again for your reply! It certainly help to ease the anxiety I have been feeling. R xx
shaws , Thank you so so much! That is brilliant excerpt! I am still not able to follow the links through when clicking on them. Is this the full article? nebula.wsimg.com/e0c9c9ed95...
Sorry the link didn't work. Sometimes there's a problem because all of Dr Lowe's work has been archived and can be awkward sometimes but I was able to access it to copy/paste but it doesn't work at present on the one above. The part statement above was by a Scientist/Researcher/doctor.
Content on HealthUnlocked does not replace the relationship between you and doctors or other healthcare professionals nor the advice you receive from them.
Never delay seeking advice or dialling emergency services because of something that you have read on HealthUnlocked.