Hello 😊 Please could I have some help with interpreting my 2nd lot of thyroid results? They are 8 weeks after the first as kindly advised on here. Please can I also get some advice on possible next steps?
Apologies this is so long but wanted to share as much detail as possible to save anyone having to ask a lot more questions.
I’m trying to unpick what symptoms are caused by chronic iron deficiency and what may or may not be a thyroid issue.
greygoose – hello there, you were very kind to comment on my first post, would love to have your input again please? Of course, anyone else’s advice is most welcome too!
Test at 9.40am, fasted (water only) no biotin as I don’t take it, and no other supplements for 36 hours before. Previous test also 9.40am.
Background
I’m undiagnosed and not on thyroid replacement. 45 year old female. Vegan - wholefoods and take a number of supplements.
I have many hypothyroid symptoms some of which overlap with iron deficiency and B12 deficiency.
I am taking iron supplements as I was severely iron deficient (ferritin 8ug/L ref range 30-250) and also anaemic in September 2023. I have a long history of mis-diagnosed iron deficiency dating back to age 2 – only just discovered recently.
I have longstanding PCOS but experienced few of the obvious traditional symptoms.
I started taking HRT in April 2023 as on top of everything else I was getting some perimenopausal symptoms and also because osteopenia was diagnosed – am still trying to get the dose right.
Long standing use of antidepressants and poor mental health episodes.
Fibromyalgia diagnosis 2016. GP now thinks FND too.
After getting ‘that virus’ 18 months ago, things have got worse. Before, I used to get random weeks where I would feel remarkably better (90%) for no apparent reason, then I’d go downhill again. The last 18 months I have no longer being experiencing any good days or weeks.
First ever TSH done in 2004 age 25 when I started to complain more about symptoms to my GP – TSH 3.4 (0.5-4.2). But, looking back I can see a few problems started in childhood.
Currently awaiting referral to Neurology and ENT. Also awaiting more tests for my low blood pressure.
Symptoms - I posted this list in the PA forum as it seemed pertinent to B12 deficiency. I haven’t listed all my symptoms as I’d already spoken to the GP about some others at a previous appointment - I probably have another 15 to add! healthunlocked.com/pasoc/po...
My own observations on these results
Thyroid – I interpret this as the pituitary is calling for more thyroid hormone to be produced hence TSH has risen a little since last time, and in turn fT4 and fT3 have responded by also rising a little. This would make sense. No antibodies again (nor goitre) so not showing signs of traditional Hashi’s/Ord’s.
What I’m not sure is if this is an appropriate (and good) response and indicates no problem in either pituitary/hypothalamus or the thyroid itself? I think fT4 and fT3 are still lower in the range than ideal (for euthyroid) but maybe this is ‘my normal’ and not a cause of symptoms – hard to know as I’ve had some symptoms for 20 years or more and no thyroid tests before the 2004 one (TSH 3.4) for comparison.
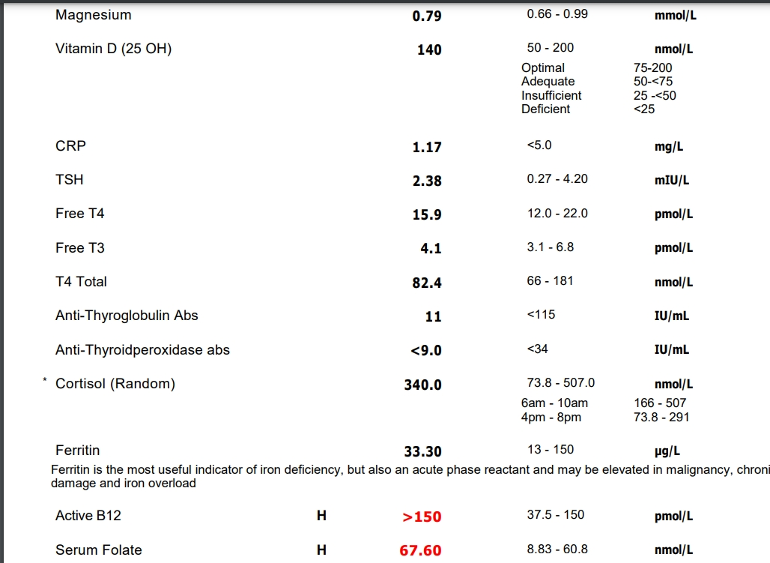
TSH 2.38 (0.27-4.2) - 53.7% though range - previous 1.75 (37.7%)
fT4 15.9 (12-22) - 39% - previous 15 (30%)
fT3 4.1 (3.1-6.8) 27% - previous 3.7 (16.2%)
Ferritin - number looks as though it’s not improved however (annoyingly) the range is different. Going on percentages through the range there does look to be an improvement but not sure this is an accurate comparison. I believe it’s still far from optimal so I will continue to supplement.
Nov – 31 (30-150) = 0.8%
Jan – 33 (13-150) = 14.6%
B12 and Folate – Active B12 in the November test didn’t appear deficient (Active B12 was 95 (37-188) but after consultation with the PA group and much research I decided to try self-injecting B12 for a while in the hope for improvement in neuro symptoms. Active B12 has obviously risen over range due to this, not worried, will continue on this path. I have been supplementing folinic acid and am now over range so will drop back a bit before re-testing.
Vit D – Looks good at 140nmol/L (50-250), I supplement through the winter and sunbathe in the summer, plus measure twice per year to keep within 125-175.
Cortisol – Mid range, I think ok but a multi-point saliva test I believe is more accurate plus measuring DHEA at the same time may be useful..
Possible next steps?
1. Wait 6-8 weeks and test again with a Thyroid Advanced panel? Hopefully ferritin continues to rise towards optimal levels.
2. Get a thyroid scan to check for anything amiss? Would prefer not to spend the money if not warranted but as I’ll be in London soon it would be easier to get it done at that point than make a special trip another time.
3. Get a genetic test from Regenerus Labs for possible conversion issues – not sure if this is useful in my case as not on thyroid replacement hormones?
4. Get a multi-point saliva test to assess if adrenal issues could be playing a part?
Thank you for managing to get this far! All advice most welcome please and anything else anyone can see that I’ve missed.
Written by
Bertiepuss
To view profiles and participate in discussions please or .
Hello! I've had a couple of full iron panels, November and December, but after starting the iron supplements. As I've been supplementing quite heavily I wanted to check I was not overdoing it with the iron and making serum levels and saturation levels too high. All good, still within range.
Well, although range switch is annoying, the improvement is ferritin in the time you took, is enviable.
Even in original range, that 30 level is a threshold and I would guess - if isolated - this would show symptom improvement.
Personally I’m curiously jealous how you are taking supplements and keeping your iron in range. How much are you supplementing, and do you know how much you’re eating? Also, don’t underestimate the symptom benefit of having sufficient iron. I’ve flip flopped on that and low iron vs in range iron was night and day for me.
I’m looking forward to hearing the refined view of your Ts. As my entire frame of reference is for hashi/hypo. For example, Vit D to me looks too high for a euthyroid person. I guess you’re trying to figure out if you are euthyroid or hypo? Or are your other conditions calling for higher D?
Sadly my improving ferritin has not improved symptoms very much, yet, but having learnt recently that I've been iron deficient probably my whole life, I appreciate it will take time for my body to start using it for all the necessary processes it's involved with. I am following a protocol on a FBook group which advises (based on American haematology research) how much iron you need to take on your body weight, plus regular testing to ensure you are not overloading. It's very comprehensive and has a set of excellent guides to follow on how to deal with iron deficiency. However, it's been a bumpy road with having to try different forms of iron due to stomach problems it has caused.
I have also been taking tranexamic acid to reduce the blood flow from the horrendous periods I was having and the HRT seems to have stopped the double, back to back periods. I get a reasonable amount of iron from my diet (not from meat) measured using the Chronometer app. So, a combination of things is leading to numbers improvement, but not yet meaningful symptoms improvement.
My Vit D is at that level because I supplement 3-4k iu's per day and get sun in the summer, no other reason, When I drop to 2k iu's my number go just below 100. I used to be deficient before I started supplementing 15 years ago. Bear in mind, these are UK measurements and I see you are in the USA, maybe you are reading the results in ng/mL (UK is nmol/L) which of course 140 would be high?
Yes, trying to work out if one particular deficiency (obviously iron, maybe B12, and I'm addressing both) is the whole problem or if there is any chance hypothyroidism is playing a part. Maybe adrenals too - of course it's all interlinked. According to some thyroid websites websites I read, my numbers are not optimal. Clearly I'm not overtly hypo but maybe there is something or other going on hence asking those with more experience here!
I’ve been blindly just aiming for 1-3x the daily value but would love a more scientific approach. I use MyFitnessPal and will check out Chronometer.
Yes, that’s probably it on the D3 units… and since you’re already calculating, here’s a link that might help validate/ confirm your dosing that I was grateful when Eeyore100 shared it grassrootshealth.net/projec...
I’m working on my iron/ferritin with purpose right now, and adrenals are in my “next” list after I do.
greygoose I know Bertiepuss tagged you for thyroid insights! I think it was you or SD who gave advice to me for my own presumably euthyroid daughter with ambiguous thyroid #s and diagnosed iron anemia… which was - fix the iron first, then deal with thyroid. Although my daughter was more 60% through ranges and Bertie is lower.
Thank you. I skimmed through past posts but couldn't find any replies from me. But I remember now.
Bertiepuss , hi. So...
FT4: 15.9 mU/l (Range 12 - 22) 39.00%
FT3: 4.1 pmol/l (Range 3.1 - 6.8) 27.03%
Well, at 2.38 your TSH is still low in-range compared to your low Frees. One would expect it to be much higher. So, it does still look like your pituitary is mal-functioning. Trouble is, doctors are just going to look at these results and say 'everything in-range, case dismissed - next!'
Here's something I wrote on the subject earlier today:
Thing is, you see, if you don't see something regularly, you tend to miss it when you do. He says your thyroid is 'normal' because both TSH and FT4 are within the stupid range. And doctors rely too heavily on ranges, without considering what the level within the range and the correlation between the different test results, and all that implies. They just give it a quick glance, all in-range so must be ok. It's not even thinking outside the box they need to do, it's all in the box. They just need to think about it more deeply. And, sometimes if we point these things out to them, you get the 'oh, yes...' reaction.
Hi greygoose , thank you so much for coming back to me on this😊 and thank you for the link to the post of the other member you replied to.
Have I understood this correctly? The level of TSH production should be eliciting a greater response from the thyroid gland than it is currently. So, one would expect with that level of TSH (2.38) that fT3 and fT4 would be higher in range?
I'm trying to understand this central hypo thing - my ft4 is not super low, but I get that it's possibly not optimal either. From what I've read, to have central hypo investigated, fT4 would need to be very low in range or below range with a normal TSH - fT3 will be ignored.
So, as you say, my doctor will never take these results as anything other than normal. No point even talking to them about it. Clearly I won't get anywhere on the NHS but I somehow think even paying for a private Endo appointment will result in me being laughed at having read the poor experiences with Endo's of others on here.
So what do I do next? What would give the most useful information and then what can I do with that information?
1. Wait 8 weeks and test again with a Thyroid Advanced panel? Hopefully by continuing with iron supplements my ferritin will rise towards optimal levels and maybe the thyroid function will also improve as a result?
2. Get a thyroid scan to check for anything amiss with the thyroid itself? Obviously if there is a central problem only, then one would expect to see a normal looking thyroid and that would rule out the thyroid itself causing problems. Unless both thyroid and pituitary are affected...
3. Get a genetic test from Regenerus Labs for possible conversion issues – not sure if this is relevant to me? I guess as fT3 is tracking a little behind fT4 that show normal conversion and it's just that both are not optimal.
4. Get a multi-point saliva test to assess if adrenal issues could be playing a part? Might help to build a picture of lower pituitary function?
Have I understood this correctly? The level of TSH production should be eliciting a greater response from the thyroid gland than it is currently. So, one would expect with that level of TSH (2.38) that fT3 and fT4 would be higher in range?
Not exactly, no. The thyroid is making what it can according to the level of stimulation it's getting. But, it's not getting enough stimulation to make decent levels of thyroid hormone. It's not the thyroid that is at fault, it's the pituitary because the pituitary is not responding to the low levels of thyroid hormone and making more TSH.
From what I've read, to have central hypo investigated, fT4 would need to be very low in range or below range with a normal TSH - fT3 will be ignored.
In this crazy, mixed-up thyroid world, that's probably true. Because they don't understand that those levels are low enough to cause symptoms, and all the other implications of low level stimulus. They're wrong, but...
Clearly I won't get anywhere on the NHS but I somehow think even paying for a private Endo appointment will result in me being laughed at having read the poor experiences with Endo's of others on here.
Endso are rarely the best people to see about a thyroid problem. They are 99.9% diabetes specialists. BUT, there are some out there who do understand, as I probably said, because we do have people on this forum that have managed to get diagnosed with Central Hypo. So, what you want is recommendations from those people. The trick is attracting their attention to reply to your post. And that best way to do that is to word your title carefully. Something like: Recommendations for private endos that understand Central Hypo, please. Or something like that.
1. Wait 8 weeks and test again with a Thyroid Advanced panel?
Well, you will need to test again eventually. Because eventually the thyroid hormone levels will drop even further. Impossible to say exactly how long that will take but say something like three months?
Hopefully by continuing with iron supplements my ferritin will rise towards optimal levels and maybe the thyroid function will also improve as a result?
I really don't think that raising ferritin will improve your thyroid function because there's nothing wrong with your thyroid. It would function better if it got more stimulation. And, whilst having optimal ferritin is essential for all sorts of reasons, I don't think it's going to have any effect on your pituitary/TSH.
2. Get a thyroid scan to check for anything amiss with the thyroid itself? Obviously if there is a central problem only, then one would expect to see a normal looking thyroid and that would rule out the thyroid itself causing problems. Unless both thyroid and pituitary are affected...
A good idea just to be sure. But I don't think that's going to cut any ice with your bog-standard GP! S/he would just take that as evidence that you don't have any sort of thyroid problem, end of. They just don't have the knowledge to draw any sorts of conclusions.
3. Get a genetic test from Regenerus Labs for possible conversion issues – not sure if this is relevant to me? I guess as fT3 is tracking a little behind fT4 that show normal conversion and it's just that both are not optimal.
Waste of money at this point, because conversion is not your problem. Your problem is lack of TSH. And I don't think that has anything to do with genetics.
4. Get a multi-point saliva test to assess if adrenal issues could be playing a part? Might help to build a picture of lower pituitary function?
That's a much better idea than the others. But, given that the average doctor knows nothing about adrenals or cortisol, any more than s/he knows about pituitaries, I'm not sure they'll take any notice of that. However, you will know. And knowledge is power. So, yes, I'd personally go with that as the next step.
Thank you greygoose, that's really helpful advice 👍 😊 A few more questions if you please?
"1. Wait 8 weeks and test again with a Thyroid Advanced panel?
Well, you will need to test again eventually. Because eventually the thyroid hormone levels will drop even further. Impossible to say exactly how long that will take but say something like three months?"
In response to your above answer, wondering what do you make of this please? 3.5 years ago I had a comprehensive thyroid panel done by a nutritionist to try to help with unpicking my problems. Unfortunately she retired soon after and never gave her opinion on my results. The analysis notes given from the testing company advised on the thyroid results "dysfunction highly likely, much improvement needed" 🤔
So here I am, 3.5 years later, and my results remain fairly much the same, possibly better? Nothing is getting worse in terms of numbers from what I can see. Do you think this still points to pituitary despite there not being an obvious decline over a long period of time?
Are there any other tests you know of to determine pituitary issues that I could order myself at a reasonable cost (other than saliva test mentioned), before trying to see a specialist? Wondering what will accurately show there is a pituitary issue, I guess maybe an MRI?
I know central hypo is not what you have yourself and I appreciate you are not medically trained, but with your wealth of knowledge and research, I highly respect your opinion. Do you have any particularly useful resources you can share about central hypo please, so I can can further read about it myself?
Do you think this still points to pituitary despite there not being an obvious decline over a long period of time?
Well, yes. Because although your thyroid hormone numbers have slightly improved - which isn't that surprising because there's bound to be some variation caused by external factors - your TSH remains too low and is not responding to your low thyroid hormone levels.
Are there any other tests you know of to determine pituitary issues that I could order myself at a reasonable cost (other than saliva test mentioned), before trying to see a specialist?
I don't think there are, no. The pituitary makes a lot of hormones, but the tests - apart from TSH - seem to be reserved for specialists to order. Even a GP can't order them.
And even if you do the saliva test, that won't test your pituitary hormones, it will test the adrenal hormone, cortisol - oh, and get one that also includes DHEA. But, the thing is, if your cortisol is low for 24 hours, then you might get an endo to order a Short Synatchen Test which - hopefully (but not always) - will include testing for ATCH, which is a pituitary hormone.
Wondering what will accurately show there is a pituitary issue, I guess maybe an MRI?
An MRI might. But, then again, it might not. Depends what is wrong with your pituitary.
Two well-known causes of Central Hypo are a bad bang to the head, and excessive bleeding during child birth. Neither of those would show up on an MRI, but might make an endo take the problem more seriously. What would show up would be an adenoma (benign tumour) on the pituitary, or a shrunken/mishaped pituitary (that's called Empty Sella, or something like that, I'm a bit vague about those things).
I do have some links I can share with you, but not sure how helpful they will be:
Well, I just plugged my numbers into the SPINA Thyroid app and something was flagged as a little high out of range. I'm am still trying to learn how the app works so all a bit confusing, but the interpretation by Thyroid Patients Canada says there is a (possible and very mild) Resistance To Thyroid Hormone (RTH). The explanations on how to read the app and interpret results is somewhat breaking my brain 😁 I see RTH mentioned as a possible cause of CH and this is mentioned in the link you sent to the Endocrinology advisor website. I shall put on my detective hat again a little later.
I haven't had a bad bang on the head but I did fall down the stairs a few years ago, just the last couple of steps but landed very heavily on my bottom and I certainly saw stars in my eyes as the force ricocheted upwards. That's when my more mild symptoms got worse and the drunk feeling started 4 days after the fall. No idea if related or not, probably will never know.
I will follow your suggestions and see from there. Hopefully I can get a recommendation for a thyroid specialist with central hypo knowledge. I am loathe to be forced into spending yet more money (like so many others) to try to find help but looks like that's what it will take. Many thanks again for your support, it is truly appreciated 🙏😊
the interpretation by Thyroid Patients Canada says there is a (possible and very mild) Resistance To Thyroid Hormone (RTH).
Are you sure about that? RTH and not TRH? Complicated, I know, but they are two entirely different things.
Resistance to Thyroid Hormone (RTH) is when you have good levesl of thyroid hormone in your blood but still feel hypo because it can't get into the cells. That would not appear to be your case because your levels of thyroid hormone are not good!
I see RTH mentioned as a possible cause of CH and this is mentioned in the link you sent to the Endocrinology advisor website.
No, it doesn't mention RTH. It's talking about resistance to thyroid-releasing hormone - TRH.
TRH is a hypothalamus hormone which somehow tells the pituitary when to make TSH. Quite how that works isn't very clear, and nobody really seems to know, but the pituitary can become resistant to TRH. If that is the case, then TSH will be low, but other pituitary hormones will be good. So, resistance to TRH can be one cause of abnormally low TSH.
Told you my brain was breaking 😁 I'm muddling my T,R,and H's. Now I may break your brain with the info below, sorry!
You are right, the article is indeed talking about Thyroid-Releasing Hormone Resistance or Deficiency. I mistakenly thought this was the same thing as RTH. Thanks for pointing out it is not! So, TRH does not seem to apply in my case as TSH is not abnormally low or are you saying mine is abnormally low as it's inappropriately low compared with the levels of fT4/3?
Yes, the SPINA Thyroid result is definitely talking about RTH but they describe it in a different manner to you - that the receptors in the pituitary are resistant and not the cells specifically. Maybe this is a different form of RTH, or it's the same and so you get the resistance in the pituitary receptor cells and the cells elsewhere in the body at the same time?
See below in italics, taken from The Thyroid Patients Canada website . My TTSI value (Thyrotroph thyroid hormone resistance index) is only just outside the reference range at 175 (100-150). And, my results from 8 weeks ago were within the reference range so this all may well be irrelevant...but, maybe there is something here (very mild RTH) playing a minor part, who knows as it's not hugely obvious?
5. TTSI: Thyrotroph thyroid hormone resistance index
TTSI data can help diagnose Resistance to Thyroid Hormone (RTH) and other disorders that mimic it.
RTH means the thyroid hormone receptors in the pituitary gland require more T4/T3 than normal to stimulate them in order to bring down the TSH.
To the degree TTSI is significantly elevated (reference 100-150), a patient may have RTH. According to a clinical study by Pohlenz et al, 1999, cited in the SPINA-Thyr manual:
Normal TTSI is 136 (reference 100-150) Mine is 175
Mild pituitary-selective RTH = 308 Mine is not anywhere near this level
Severe pituitary-selective RTH = average 747
Generalized RTH (even beyond the pituitary) = average 1559.
In RTH syndromes, the person has a biological requirement for higher Free T3 and possibly higher Free T4 levels than the normal levels found in healthy controls, at the upper limit of reference or slightly higher.
A high TTSI may also reveal other disorders. (I did not include points 1 and 2 as they didn't seem relevant at all. Point 1 was about non-thyroidal illness and point 2 was about TSH-receptor blocking antibodies in thyroid-disabled patients on therapy (not me). Points 3 and 4 are probably not relevant either but I've included them in case you spot something.
3.Pituitary TSH hypersecretion may be caused by a pituitary adenoma (TSH-oma). This is very rare. If it occurs during thyroid therapy, a high TTSI would result. A healthy thyroid gland is required for an abnormally high level of TSH stimulation to cause hyperthyroidism (high FT4 and FT3) (ref 12. Beck-Peccoz et al, 2000/2019). However, if the patient does not have enough thyroid tissue for TSH to stimulate, the FT4 cannot rise along with the TSH stimulation, and the TTSI will rise significantly.
4.A rare genetic condition called a “partial SBP2 deficiency” can also cause TSH to be abnormally high per unit of T4. In this case the reason is that T4-T3 conversion via D2 is significantly impaired within the hypothalamus and pituitary gland. This condition handicaps the SECISBP2 gene, which is responsible for forming the three deiodinase enzymes (D1, D2, D3) as well as glutathione peroxidase, from selenium. Such cases can be distinguished from “resistance to thyroid hormone” because the FT3:FT4 ratio may be abnormally low prior to therapy, and the TSH suppresses normally in response to T3 dosing. (See ref 11, Dumitrescu et al, 2008)
So, if the SPINA results can be relied on, this is me having an uneducated guess - Maybe I biologically require higher levels of fT3 and possibly fT4 (compared to healthy controls) as stated above due to a very mild form of RTH. So the pituitary is a little unhappy, but not unhappy enough to raise TSH really high hence why my thyroid hormone levels remain lowish normal. A bit of a catch-22. Quite possibly they are quite a bit lower than I need them to be to feel well and bring the TSH down to around 1. And/Or there is not enough healthy thyroid tissue (mild atrophy but without antibodies) to produce enough hormones in response to the TSH. And/Or there is something else affecting the pituitary (TRH resistance/deficiency?) causing what looks a little like CH but not full blown with obvious low ft4 that's below range. 😵
But, the SPINA app's results didn't point to CH on another value it reports...I guess it could be wrong. I don't think it is supposed to be used as a diagnostic tool, more to point to a direction for further investigation.
If you can bear to look at this any further I would very much appreciate your thoughts. I somehow doubt this type of conversation will be well received by an Endo, can you imagine!
OK, so you got me in the second paragraph! My brain is not officially broken.
So, TRH does not seem to apply in my case as TSH is not abnormally low or are you saying mine is abnormally low as it's inappropriately low compared with the levels of fT4/3?
No, it's RTH that doesn't apply to you because you don't have high levels of thyroid hormones. I wrote: Resistance to Thyroid Hormone (RTH) is when you have good levesl of thyroid hormone in your blood but still feel hypo because it can't get into the cells. That would not appear to be your case because your levels of thyroid hormone are not good!
TRH does possibly apply to you because your TSH is too low compared to the levels of your thyroid hormones.
they describe it in a different manner to you - that the receptors in the pituitary are resistant and not the cells specifically. Maybe this is a different form of RTH, or it's the same and so you get the resistance in the pituitary receptor cells and the cells elsewhere in the body at the same time?
As I understand it, cells in the pituitary react differently to other cells. With RTH you have good levels of thyroid hormones and low/euthyroid TSH because the pituitary is getting enough thyroid hormone and therefore reduces production of TSH. For that reason, you cannot tell RTH from a blood test, only from symptoms.
RTH means the thyroid hormone receptors in the pituitary gland require more T4/T3 than normal to stimulate them in order to bring down the TSH.
But this is the opposite of your problem. Your TSH is not high enough, so the pituitary is not having problems bringing down, but problems raising it.
In RTH syndromes, the person has a biological requirement for higher Free T3 and possibly higher Free T4 levels than the normal levels found in healthy controls, at the upper limit of reference or slightly higher.
But we don't know how much FT3 you need because it has never got that high. No, this is entirely barking up the wrong tree. You do not have RTH - or if you do, we cannot possibly know because you are clinically hypo.
3.Pituitary TSH hypersecretion may be caused by a pituitary adenoma
You do not have TSH hypersecretion! Quite the opposite. Look, not being funny or anything, but I really don't think you're ready for The Thyroid Patients Canada website. I'm not ready for The Thyroid Patients Canada website! It's hyper complicated and written in a way that is not user-friendly. You have to have a scientific background to understand it all. My advice is: leave it alone. Stick to something with simpler language. It is not for people of our level of understanding, you will only confuse yourself.
Maybe I biologically require higher levels of fT3 and possibly fT4 (compared to healthy controls) as stated above due to a very mild form of RTH. So the pituitary is a little unhappy, but not unhappy enough to raise TSH really high hence why my thyroid hormone levels remain lowish normal.
Sorry, but that is gibberish. That's not how it works. The pituitary has no idea if you have RTH, the pituitary only goes by what's in the blood, not what gets into the cells. Please, take my word for it, your problem is not RTH because you don't have enough thyroid hormone to get into the cells anyway.
And/Or there is not enough healthy thyroid tissue (mild atrophy but without antibodies) to produce enough hormones in response to the TSH.
Not your problem either. If that were the case, and the pituitary was functioning normally, your TSH would be sky high. Your problem is you don't have enough TSH. Sorry, but this is so obvious and you are making it all more complicated than it already is. Why?
And/Or there is something else affecting the pituitary (TRH resistance/deficiency?) causing what looks a little like CH but not full blown with obvious low ft4 that's below range.
But it is full-blown CH. Central Hypo just means that the pituitary is not producing enough TSH for some reason. If the problem lies with the pituitary itself it is called Secondary Hypo. If the problem is the hypthalamus, it's called Tertiary Hypo. When we don't know which one it is we call it Central Hypo. And the fact the the FT4 isn't below range yet is neither here nor there. There is not enough TSH therefore you have Central Hypo.
I somehow doubt this type of conversation will be well received by an Endo, can you imagine!
You couldn't have this conversation with an endo, they don't know enough about it. Believe me, I've tried talking to them about adrenals and they're way out of their depth with just that! They change the subject, that's all.
Got it, I think, and thank you for the thorough explanation, I will review again in the morning to make sure I understand! I'm sorry I'm making it more complicated than it needs to be. I like to understand everything in depth, so trying to pick things apart is what I tend do, and I do enjoy the learning. Drives my husband to distraction! I shall resist trying to fathom the information on Thyroid Patients Canada!
So we can't have conversations with an endo, our GP's will only look at TSH...basically you have no chance of getting proper help until your dead, ok, almost dead!
Many thanks again for your time and patience with me, it's greatly appreciated 🙏
The problem is, doctors are not educated in thyroid - or much else to do with the endocrine system - and they are terrified of hormones because they know nothing about them. Especially T3. So, no, you cannot have a conversation about anything endocrinological with an endo! Weird as that may seem. 99.9% of them are diabetes specialists so only know about insulin - and according to many diabetics I've talked to, they don't know much about that, either!
GPs sometimes know more than endos, but it's been dinned into them that they are not the specialists, endos are, so they should always defer to the endo - even if they know more than the endo. Which doesn't happen very often, but it does happen. But they still don't know very much. I remember one time I tried to have an intelligent conversation with a GP about adrenals. He frowned and gazed into the middle distance, repeating 'adrenals, adrenals, adrenals', as if he was trying to remember where he'd left them. Then I mentioned DHEA and I swear he nearly crossed himself. Another GP made the bald statement that 'adrenals are nothing to do with thyroid', end of conversation. It's hopeless, really. They have blinkered vision and a one-track mind, and if you don't fit into the typical, stereo-typed hypo box, they just don't know what to do with you, so usually 'diagnose' fibro or CFS. They're only 'happy' when your TSH is over 10.
I could go on, but I won't. I self-treat because I have a certain degree of resistance to thyroid hormone, and need a high dose of T3 only. The struggle to get enough T3 prescribed is over-whelming - FT3 needs to be high and TSH is obviously suppressed - so I gave up and self-treat. So, at least I'm alive, which I probably wouldn't be if I'd just done as I was told by doctors. I'd either be dead or a dribbling vegetable in the corner.
He frowned and gazed into the middle distance, repeating 'adrenals, adrenals, adrenals', as if he was trying to remember where he'd left them. Then I mentioned DHEA and I swear he nearly crossed himself. I nearly choked on my tea this morning reading this 🤣🤣🤣 It's not funny really, not funny at all 😬
It shouldn't be this way but if self-treatment is the only way to feel well (or at least a little better) then that's what one must do.
It totally takes the guesswork out of how much iron to supplement - the 'why' and the 'how' and also how to test properly to stay within safe limits as iron can be toxic. It will take you several hours to read all the guides but it's helped me immensely on figuring out how to deal with one piece of the puzzle. As you say, it's a case of working through all the wonky bits one thing at a time, and it takes a while! I do hope you will find the FB group really helpful.
Thank goodness we have people on the forums here to support us! I will have a look at the replies about your daughters results, thank you for pointing this out to me 👍 Sharing experiences really helps as the replies to someone else's post can shed light on ones own situation. Thanks also for the vitamin D calculator link - it turns out I am supplementing the the right amount to achieve and maintain the level I'm currently at. Seems at least I'm absorbing one nutrient efficiently 😊
Ah, right, thank you for picking this up! 👍😊 The link you have put is for the associated website but I don't think it has anywhere near as much information as the guides have in the Facebook group.
To view the guides you have to have a FB account and then you need to join the group. Once approved you can then access the files in that group. For those with iron deficiency with and without anaemia it's really worth joining just to read all the information provided.
Click on "Read the list of available tests" and on page 3 of the pdf you'll see
Urine Iodine Test:
Specimen requirements: Urine
Cost: £76
Order Code: END25
Turnaround time: 5 - 10 days
Iodine is an essential trace element, vital for healthy thyroid function. Adequate levels are required to enable the production of T3 and T4 thyroid hormones, whilst also being required in other areas of health.
Deficiencies can lead to impaired heat and energy production, mental function and slow metabolism. Urine iodine is one of the best measures of iodine status. This test is not performed as a loading test, but can be used to establish existing levels or to monitor iodine supplementation.
Thank you for the link to the iodine test. I have been vegan for 6 years and was veggie before that from about the age of 8. I supplement iodine as aware of the potential deficiency risks in a vegan diet - 150-200mcg daily, dose decided on after much research. Would you still advise it's worth doing the iodine test considering I supplement?
I take a lot of other supplements, here's the list, hefty I know but have been trying to cover all bases! Some I've taken for a long time, some for a few months and some I started more recently (in italics).
Iodine – 150-200mcg as potassium iodide
Selenium - 200mcg as selenomethionine
Iron – 110mg (elemental) as bisglycinate
Vit C – 1000mg to help absorb iron
Folinic acid 400mcg – just cut down from 800mcg
B12 – injections I self-administer since December was supplementing 1000mcg before that
Eye Complex – with Lutein, Meso-zeaxanthin and Zeaxanthin
Vitamin A – 700mcg as retinyl palmitate
Vitamin K2-mk7 – 200mcg
B6 as P5P – 100mg
Vitamin D3 – 3000-4000iu
Omega 3 – as algae oil total 1650mg EPA/DHA
Magnesium – 400mg as combination of Malate, L-Threonate and Chloride
Zinc – 30mg as bisglysinate chelate
Vitamin E and GG – 250mg Tocotrienols plus 150mg Geranylgeraniol
LDN – 4.5mg
Still waiting to start a B-complex but have held off due to not wanting the biotin content to affect blood tests. Also plan to start Boron and Creatine - have to add everything one at a time, low dose and slowly to prevent reactions.
Any further advice would be very much appreciated please 🙏
No, still on the list. However, I tried to research more about this particular test and came up with a lot of negative views on the accuracy of it. It sort of put me off to some degree so it moved down lower on my list of tests to spend on.
Content on HealthUnlocked does not replace the relationship between you and doctors or other healthcare professionals nor the advice you receive from them.
Never delay seeking advice or dialling emergency services because of something that you have read on HealthUnlocked.

")
")