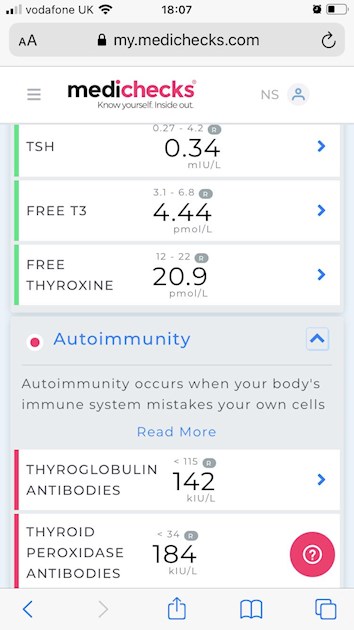
*new updated full thyroid tests including antibodies* . please review and advice. New pic of results posted. So I now have full thyroid and vitamin results below .Thanks
I posted on here a few weeks ago regarding my thyroid level whilst ttc (IVF). My latest IVF failed around two weeks ago. Before treatment my TSH level was 1.9 and after embryo transfer my TSh level went to 8.3. I had a previous failed embryo transfer in July and my TSh level was fine before treatment but was 9 after the failed transfer. I understand this may not be the reason that the embryo failed to implant but I would like to rule anything out before I start my next IVF. I had my follow up yesterday with the fertility consultant and he said the hormones I was taking have caused my TSh levels to be unstable? During treatment I upped my dose of Levo from 75 to 100 (when it was 8.3). I had my bloods done recently and my TSh is now 0.176 and free thyroxine is 24.4 (I am no longer on fertility drugs). I have now been advised to reduce my dose to 75mcg. I have also been referred to an Endocrinologist by my GP- the appointment is not till the new year. Would anyone recommend a private Endo? I have only been diagnosed with thyroid problems since last January before I started IVF. The only symptoms I’ve had is back in July when my TSh was 9..I was low in mood, brain fog and couldn’t concentrate. I feel fine now with no symptoms.
SlowDragon kindly gave me good advice a couple of weeks ago and told me to have my vitamin levels checked. I would also welcome any other advice. Below are the latest blood results.
*Can you please review my GFR and Creatine Levels. The GP said the levels are ok but the numbers are not in range*
Sorry for the long post. I will be grateful for any advice
TSh 0.176 mu/L 0.2 -5.0
Free Thyroxine 24.4 Pmol/L 10-24
GP rang yesterday to discuss the result and to reduce dose to 75mcg
Vitamin Levels
Vitamin B12 489 ng/L 170-730
Ferritin Serum 106 ug/L 13-150
Folate Serum <20.0 ug/L 3.9-26.8
Vitamin D 46 nmol 50-250
GP also discussed Vit D levels and prescribed an Osteocap 20,000 to take weekly for six weeks, bloods will then be repeated.
I’m an ICU consultant, not an endocrinologist or GP.
But I think it’s wise to wait until January to see an Endocrinologist as it takes around 6 weeks for thyroid function tests to settle after a dose change. You’re only very slightly over treated and I doubt it had much impact on your cycle.
Your Vitamins D levels are a bit low so you should think about taking a Vit D supplement. Oral sprays are easy. I agree with your GP.
Your renal function is slightly raised. I would ensure you stay well hydrated and get them retested. They won’t impact fertility but you need investigation if they remain raised. But it’s nothing to worry about. Your GP just needs to repeat in 6-8 weeks.
Thanks for your reply! I will take your advise on board. I have just started a Vit D supplement weekly for six weeks. I will have all bloods repeated in 6-8 weeks. I hoping to start IVF feb/March time so I’m hoping my bloods are in range by then.
Bloods should be retested 6-8 weeks after any dose change.....or brand change in levothyroxine
For FULL thyroid testing you need
BOTH TPO and TG thyroid antibodies tested
TSH, Ft4 and Ft3
Recommended on here that all thyroid blood tests should ideally be done as early as possible in morning and before eating or drinking anything other than water .
Last dose of Levothyroxine 24 hours prior to blood test. (taking delayed dose immediately after blood draw).
This gives highest TSH, lowest FT4 and most consistent results. (Patient to patient tip)
Is this how you do your tests?
Private tests are available as NHS currently rarely tests Ft3 or thyroid antibodies or all relevant vitamins
If TPO or TG thyroid antibodies are high this is usually due to Hashimoto’s (commonly known in UK as autoimmune thyroid disease).
About 90% of all primary hypothyroidism in Uk is due to Hashimoto’s. Low vitamin levels are particularly common with Hashimoto’s. Gluten intolerance is often a hidden issue to.
Hi SlowDragon..I was hoping you’d pop up on here. My GP said he was going to do full thyroid testing including Ft4, Ft3 and antibodies so I’m not sure why it’s not been tested. I will request the bloods online instead..
I took your advice from last time and didn’t take the tablet until after the bloods were taken and didn’t eat anything (8am) and the previous tablet was taken 24hrs before, therefore, the latest results will be a true reading.
So, do you think I may have Hasimoto? Or are you unable to tell without the full thyroid bloods? No, I haven’t had an ultrasound of my thyroid yet. I’ve got an appointment with an Endo before Christmas (referred by my GP) so I’m assuming I’ll have more tests done then? I’ve read up that thyroid is linked to kidney problems, so yes, I will be having regular bloods to monitor it.
My GP said he was going to do full thyroid testing including Ft4, Ft3 and antibodies so I’m not sure why it’s not been tested.
We see this all the time. Whatever the GP requests (could be "Thyroid Function Test" or every test you mention individually), the lab takes the view they know best. If TSH isn't significantly out of range, that might be all they do. If TSH is high, they might do Free T4. If TSH is low or very low, they might really push the boat out and do Free T3.
The claim is that they are not needed. I disagree. And suggest that the only reason they are refused is cost.
The labs have set up in their computerised testing systems things like:
"If TSH is in range, don't do any more testing." So the GP might have asked for everything.
I see it as gross malpractice. The staff in the labs have no direct professional relationship with you. Yet their decisions directly affect your treatment.
When I had my last bloods, the hospital lab didn't do one of the tests (vit D) requested by the CONSULTANT - so it's not just GPs they ignore! At the subsequent phone consultation, I suggested that the consultant out-ranked the lab assistant somewhat and therefore shouldn't be over-ruled on a whim. He laughed a bit at that ... but the inference was that it happens to him all the time.Guess nothing will change until the consultants, GPs etc all complain ...
Even if we don’t start on full replacement dose, most people need to increase levothyroxine dose slowly upwards in 25mcg steps (retesting 6-8 weeks after each increase) until on full replacement dose
Consider starting levothyroxine at a dosage of 1.6 micrograms per kilogram of body weight per day (rounded to the nearest 25 micrograms) for adults under 65 with primary hypothyroidism and no history of cardiovascular disease.
Traditionally we have tended to start patients on a low dose of levothyroxine and titrate it up over a period of months.
RCT evidence suggests that for the majority of patients this is not necessary and may waste resources.
For patients aged >60y or with ischaemic heart disease, start levothyroxine at 25–50μg daily and titrate up every 3 to 6 weeks as tolerated.
For ALL other patients start at full replacement dose. For most this will equate to 1.6 μg/kg/day (approximately 100μg for a 60kg woman and 125μg for a 75kg man).
If you are starting treatment for subclinical hypothyroidism, this article advises starting at a dose close to the full treatment dose on the basis that it is difficult to assess symptom response unless a therapeutic dose has been trialled.
A small Dutch double-blind cross-over study (ArchIntMed 2010;170:1996) demonstrated that night time rather than morning dosing improved TSH suppression and free T4 measurements, but made no difference to subjective wellbeing. It is reasonable to take levothyroxine at night rather than in the morning, especially for individuals who do not eat late at night.
Thanks for this advice. I’ve had my fertility consultant write to my GP to clearly state that my TSH level needs to be under 2.5 ttc..GPs don’t seem to understand this..
Replacement therapy with levothyroxine should be initiated in all patients to achieve a TSH level of 0.5-2.0pmol/L.
Dr Toft, past president of the British Thyroid Association and leading endocrinologist, states in Pulse Magazine,
"The appropriate dose of levothyroxine is that which restores euthyroidism and serum TSH to the lower part of the reference range - 0.2-0.5mU/l.
In this case, free thyroxine is likely to be in the upper part of its reference range or even slightly elevated – 18-22pmol/l.
Most patients will feel well in that circumstance.
But some need a higher dose of levothyroxine to suppress serum TSH and then the serum-free T4 concentration will be elevated at around 24-28pmol/l. This 'exogenous subclinical hyperthyroidism' is not dangerous as long as serum T3 is unequivocally normal – that is, serum total around T3 1.7nmol/l (reference range 1.0-2.2nmol/l)."
(That’s Ft3 at 58% minimum through range)
You can obtain a copy of the articles from Thyroid UK email print it and highlight question 6 to show your doctor please emai
I'm sure I've read that Levothyroxin can have a negative effect on Oestrogen/ Progynova. What dose of Progynova are you on pre ET and what thickness is your lining at the scan pre ET?
I read something similar about Progynova upsetting the uptake of Levothyroxine...so best to ensure you take them at least a couple hours apart.
Going into FET each time has destabilised my thyroid bloods. My clinic pushed for my TSH to be under 1 going into a FET cycle rather than 2.5 for that reason. My cycle back in Feb resulted in my TSH spiking to 2.9 when I retested after the FET failed. If I’d have been at 2.5 starting, it would have been way over 5.
I have always struggled with lining thickness issues. Interesting what you’re saying Pcck about the link to Levo impact on lining.
My TSH was 1.9 before treatment so the clinic so my consultant said I was ok to start treatment. My TSH had then spiked to 8.3 after embryo transfer..it was too late to do anything then. I agree, my consultant is writing to my GP to state that my TSH needs to be under 2.5.
Yikes! That’s a colossal spike! My TSH is running a little below range at the moment at 0.04. Long-term that’s not ideal as it can cause issues with bone density, but for now I’d rather it was there.
It kind of sounds like your reproductive hormones are sensitive and when they increase they really do increase, be that in a natural or medicated cycle.
I only took Prognova for my frozen embryo transfer in July that failed. I was taking 2mg 3 x daily. For my recent fresh IVF cycle it was a different protocol. I took Meriofert 150, three vials at night. My womb lining was good at 10.6.
I had my follow up yesterday with the fertility consultant and he said the hormones I was taking have caused my TSh levels to be unstable?
I don't understand the comments from your fertility consultant. Is he trying to imply that you don't need thyroid hormones and that your TSH levels would be more stable without them? Because if so he's a danger to your health, in my opinion.
I think you need to know more about your thyroid before attempting another round of IVF. What are your levels of TSH, Free T4, Free T3, and thyroid antibodies?
If you have high levels of thyroid antibodies I would suggest that you need to go on a ruthlessly gluten-free diet. It might help and it won't harm.
...
Your cholesterol is astonishing, and in my opinion not in a good way. I've never seen anyone report a total cholesterol as low as yours before. Cholesterol isn't an optional extra in the body it is essential for life. Are you on statins or any other treatment to reduce cholesterol? I hope not, because statins are known to lead to birth defects.
What kind of diet do you eat? Cholesterol is an essential part of the human body, and it will be needed by a foetus/embryo to grow and survive. Do a search for information on hypocholesterolemia.
I found this linkwhich might be of interest, although I would suggest looking for confirmatory references elsewhere e.g. Pubmed or Google Scholar because I think the link is a commercial one. It mentions infertility and hypocholesterolemia in quite a few sections.
In your shoes I would want B12 to be top of range or even up to 1000 ng/L. B12 is not poisonous, and European reference ranges are absurdly low. Allegedly, in Japan the top of the range is about 1300 ng/L. You might find this link of interest - I think it is written by a Dutch Pernicious Anaemia/B12 Deficiency group :
Your folate result is weird and unhelpful. The fact that your result is < 20 ug/L suggests that the lab doing the testing can't measure anything less than that with any precision. So how did they come up with their reference range? In your shoes, with the test above, I would want a result somewhere between 20 and 27. See this link for more info :
If I assume you weigh 140 lbs (10 stone) then the calculator suggests the following :
----------------------------------
All suggested intake amounts are based on a weight of 110 lbs
Maintenance Dose
To achieve the desired serum level within approximately 3 months, a supplementation amount of
3,000 IU* (75 mcg) per day (this includes your current intake amount)
will be sufficient for 50% of people to achieve the desired serum level of 100 nmol/L
or
4,000 IU* (100 mcg) per day (this includes your current intake amount)
will be sufficient for 90% of people to achieve the desired serum level of 100 nmol/L.
Loading Dose
To quickly achieve the desired serum level within days†, a dose of
25,000 IU (625 mcg) per day can be taken for 4 days, followed by the above maintenance dose.
*Values rounded to the nearest 1,000 IU and are capped at a maximum of 10,000 IU/day.
†This calculation is based on published data by van Groningen et al., Eur J Endocrinol., 2010
Hundreds of peer-reviewed scientific studies have documented the well-established safety of single 'loading' doses of vitamin D to get levels up quickly (1-26). Loading doses ranging from 100,000 IU to 600,000 IU have been shown to rapidly increase vitamin D levels, but fail to sustain levels longer than 2-3 months. Larger doses induce more rapid breakdown of vitamin D (1-2). Therefore, the customized loading dose has been divided into doses of 25,000 IU over a number of days to achieve the initial increase in vitamin D levels. The maintenance dose is your custom daily dose recommended to achieve and sustain the desired levels of vitamin D.
---------------------------
Please note all references to vitamin D supplementation are specifically to vitamin D3, never vitamin D2. You need to take co-factors along with vitamin D - magnesium and vitamin K2. They get mentioned on the forum a lot, so do a search for more information on them. SeasideSusie's posts on them are particularly helpful.
Vitamin D3 supplements are available in many different doses on sites that sell supplements.
...
Good luck.
I know what it is like going through IVF. I did it five times in the 1990s, got pregnant three times, and lost them all in the first trimester. I had no access to the internet (which barely existed at the time anyway), and I suspect my thyroid (which the IVF clinic told me was "borderline underactive" but nobody wanted to treat me) was one reason for things not working. I also strongly suspect that low nutrients were another reason for the outcomes I got. Going gluten-free might have helped me too.
I had my TSH level checked on the 30th September before commencing IVF and it was 1.9 and the clinic was happy to go ahead with treatment. I didn’t have my embryo transfer till the 28th October (due to injections and egg collection). I did request to have my TSH level checked before the transfer due to my TSH not being stable but the clinic said it wasn’t necessary. I then requested to have my bloods checked at my GP after the transfer and my TSH level was 8.3 and my Levo was increased from 75 to 100 by my GP. My consultant said the hormones would have affected my thyroid level and that I need to speak to an Endocrinologist before the next IVF. I’m more annoyed that my clinic don’t bother checking bloods before transfer.
I will have full thyroid levels checked and post back on here. I’m not on any statins or any other medication for cholesterol..it’s the first time from yourself that I’ve heard it’s low? I have always ate a balanced diet with the odd treat. I’m a good weight and my BMI is 23. I have been following the Mediterranean diet for the past two weeks which is fresh wholesome food including eating fish three times a week, and strictly no processed food. I am also looking to cut out gluten (This diet is recommended for women ttc).
Sorry to hear that you’ve had a difficult time with ttc. It’s a long tough journey
I have started taking a prenatal that contains all vitamins including B12 (20ug 800) I have not yet had a read of the link you posted, but I will do thanks. I have just started taking Osteocaps 20,000 a weekly tablet for six weeks for my low vitamin D level. I will look into the other vitamins that you have recommended. Thanks for the advice.
Thanks SD. I didn’t no I had Hashimoto’s. What is the treatment for this? I need my antibody levels to come down for ttc. I now know vitamin levels play a part, my vitamin D level is 46 and I am currently taking a weekly Osteocap 20,000 units. I have already started to cut out gluten from my diet..would it be better to eat gluten then do the blood test to check for celiac disease first? I will resend the post.
Hashimoto's affects the gut and leads to low stomach acid and then low vitamin levels
Low vitamin levels affect Thyroid hormone working
Poor gut function with Hashimoto’s can lead leaky gut (literally holes in gut wall) this can cause food intolerances. Most common by far is gluten. Dairy is second most common.
According to Izabella Wentz the Thyroid Pharmacist approx 5% with Hashimoto's are coeliac, but over 80% find gluten free diet helps, sometimes significantly. Either due to direct gluten intolerance (no test available) or due to leaky gut and gluten causing molecular mimicry (see Amy Myers link)
Changing to a strictly gluten free diet may help reduce symptoms, help gut heal and slowly lower TPO antibodies
While still eating high gluten diet ask GP for coeliac blood test first or buy test online for under £20, just to rule it out first
The predominance of Hashimoto thyroiditis represents an interesting finding, since it has been indirectly confirmed by an Italian study, showing that autoimmune thyroid disease is a risk factor for the evolution towards NCGS in a group of patients with minimal duodenal inflammation. On these bases, an autoimmune stigma in NCGS is strongly supported
In summary, whereas it is not yet clear whether a gluten free diet can prevent autoimmune diseases, it is worth mentioning that HT patients with or without CD benefit from a diet low in gluten as far as the progression and the potential disease complications are concerned
Despite the fact that 5-10% of patients have Celiac disease, in my experience and in the experience of many other physicians, at least 80% + of patients with Hashimoto's who go gluten-free notice a reduction in their symptoms almost immediately.
Was this test done as early as possible in morning before eating or drinking anything other than water and last dose levothyroxine 24 hours before test?
Suggest you might consider refusing to reduce levothyroxine dose
Currently your Ft4 is 89% through range
But Ft3 is only 35% through range
Helpful calculator for working out percentage through range
Like thousands of Hashimoto’s patients you have poor conversion of levothyroxine (Ft4) to active hormone (ft3)
If you reduce levothyroxine, Ft3 will drop further
Getting vitamin D levels optimal and strictly gluten free diet may help
But likely to need addition of small doses of T3 prescribed alongside levothyroxine
Email Dionne at Thyroid UK for list of recommend thyroid specialist endocrinologists who will prescribe T3.....
...NHS and Private
tukadmin@thyroiduk.org
The aim of levothyroxine is to increase dose upwards until Ft4 is in top third of range and Ft3 at least half way through range (regardless of how low TSH is) ...important to have optimal vitamin levels too as this helps reduce symptoms and improve how levothyroxine works
Dr Toft, past president of the British Thyroid Association and leading endocrinologist, states in Pulse Magazine,
"The appropriate dose of levothyroxine is that which restores euthyroidism and serum TSH to the lower part of the reference range - 0.2-0.5mU/l.
In this case, free thyroxine is likely to be in the upper part of its reference range or even slightly elevated – 18-22pmol/l.
Most patients will feel well in that circumstance.
But some need a higher dose of levothyroxine to suppress serum TSH and then the serum-free T4 concentration will be elevated at around 24-28pmol/l.
This 'exogenous subclinical hyperthyroidism' is not dangerous as long as serum T3 is unequivocally normal – that is, serum total around T3 1.7nmol/l (reference range 1.0-2.2nmol/l)."
(That’s Ft3 at 58% minimum through range)
You can obtain a copy of the articles from Thyroid UK email print it and highlight question 6 to show your doctor please email Dionne at
The test was done first thing in the morning without taking my tablet or eating or drinking. I have been referred by my GP to see an NHS Endocrinologist.. the appointment is New Year’s Eve..would it be better to go private?
Well I found out the appointment date one month ago so still quite a long wait..I’m not sure what the Endocrinologist specialises in but I will look at going private just in case.
Content on HealthUnlocked does not replace the relationship between you and doctors or other healthcare professionals nor the advice you receive from them.
Never delay seeking advice or dialling emergency services because of something that you have read on HealthUnlocked.