Drug action information and diagnosis
In My post “Post 1 Part 3” I attempted to describe my thinking on the concept of Stress Breakdown Point. Graph 1 in the “Post 1 Part 3” post indicated that a small change in stress could make a lot of difference in quality of life for people with chronic health disability.
In the posts I have presented and hope to present I hope to be able to give people the means to present a case to their medical doctors or consultants as to why they need to do something differently. It has taken me quite a number of years to gather the information to develop arguments. They cannot be developed in the five or ten minutes of a medical consultation. So I am hoping that those who can will take my arguments look at them closely and improve upon their accuracy or change them to fit their particular circumstances.
On Healthunlocked there is much talk on diagnoses. What is a diagnosis? My take on what is a diagnosis is as follows. “A diagnosis is a summary for a compilation of a list of symptoms” Hopefully the diagnosis can result in a course of treatment which is beneficial to the health and well being of the patient. Looking at a diagnosis this way enables a better understanding of the issue that a diagnosis does not give a cause for the symptoms present. The cause has to be established by investigation. There is limited time and limited funds for investigations so all the facts needed for an accurate cause for a particular diagnosis are not always present. The patient needs to bear this mind in discussions with their medical consultant. Long term health disabilities can be very stressful and sometimes the stress is such that it becomes very difficult to disentangle stress of symptoms from a physical health disability causing mental overload from the symptoms of some mental health disorder. Many patients have been prescribed psychiatric medication or given a mental health diagnosis (as per DSM) because all the medical consultant can see is the psychiatric response to the stress of a health disability rather than the underlying physical health disability stress overload that needs better management strategies.
On page 1 in the book “Fascia What it is and why it matters” by David Leondak there is a quote by Gisela Draczynski. It says:
“Experience teaches that it takes years or decades for new fundamental insights in medicine to become common knowledge among doctors.
‘Additionally any body of knowledge that reveals linear (or) causal relationships is more easily understood and categorized than those that reveal relationships that are multidimensional’"
To use a bit of algebra, We can say for a linear (or) causal relationship y = f(x). For a multidimensional relationship we can say y = f (x1 + x2 + x3 +x4 + …. +xn). Where x1 x2 x3 x4 …. xn are different types of variable. Most issues with many long term health disabilities are multidimensional yet in the interaction with the patient the doctors tend to treat health disabilities as having a simple causal relationship.
For example: Back pain is a bit debilitating. It can make a person a bit non communicative and depressed. Long term back pain creates a sleep deficit. Sleep is needed to clear waste products from the brain because the brain cannot clear these waste products when it is awake. The patient who has had back pain for a few months starts to present a mental health disorder to their doctor because of the sleep deficit. It does not take much lack of insight by both patient and doctor for the doctor to start thinking that the problems are due to the patient’s mental health disorder. The doctor who wishes to avoid a scene will tell the patient one thing and put something else in the notes. Mental health disorder is taken by many people to imply that the patient is not able to understand their condition and themselves.
I am a victim of what happened in the UK before 1991. Patients were not allowed to see their medical records. This allowed unethical doctors to tell patients one thing and write something else in the medical notes. This is still going on.
I recently had a appointment with Dr Y at a local hospital. He told me that Diagnosis “X” matched the issues I had and suggested seeing another specialist and having more tests. I looked up Diagnosis “X” on the internet. It was something that needed further investigation. Dr Y sent a letter to my GP. The letter contained no mention of diagnosis “X” only that the results of the tests done were within normal parameters. I saw the recommended other specialist at the same hospital who agreed that my symptoms would match diagnosis “X” but could go no further on resolving the issue because the specialist needed additional test results. The NHS system did not allow this specialist to order the needed tests. The specialist had to write a letter to Dr Y for Dr Y to order the tests. I had to request that the specialist refer to Diagnosis “X” in the letter they wrote to me, my GP and Dr Y. The letter the specialist sent did suggest that I had Diagnosis “X”
I reported this issue to a friend who was trying to get treatment for their son. My friend told me of similar problems that they were experiencing. They also told me that they would have had to wait six months to see a specialist who could interpret some test results. My friend contacted people she knew in Europe and got back an interpretation of the test results within two days. They also told me of the experience where their son was referred to a specialist. They waited several months only to be told that the specialist did not see anyone under the age of 18. They had to start the request for an appropriate specialist all over again. i.e. at the bottom of the waiting list. By the time the person manages to see a specialist conditions for the son would have changed maybe significantly so the original test results would not be reliable for that point in time when the specialist was seen. However, the diagnosis would be made and stored in the medical records based on test results made at another point in time that is significantly different. The medical records would be unlikely to record this problem.
Graphs
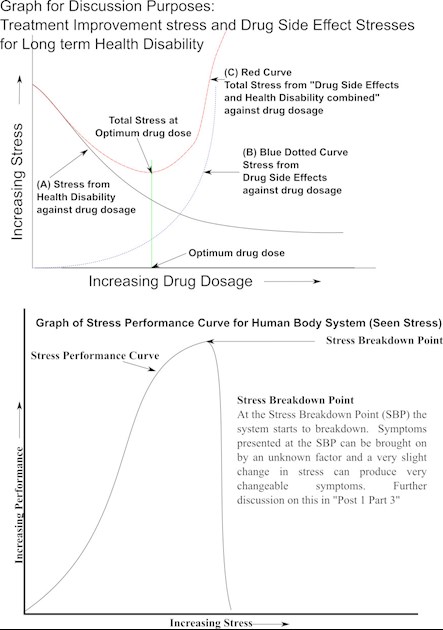
There is a lot of talk about trials and accuracy of treatment. The image shows two graphs: a Graph for Discussion Purposes Treatment Improvement Stress and Drug Side Effect Stresses for Health Disability and a graph of performance versus stress which shows Stress breakdown Point. In the top graph there are three curves, A, B and C. The three curves demonstrate what happens when medication is taken for a health disability. How the curves are in reality will vary from drug to drug, health disability to health disability and person to person. The curves are presented to highlight my thinking and form a working model for a person with a long term health disability to investigate their condition, and discuss with their doctor. A working model does not need to be scientifically accurate. It provides a means to think and present a case for further investigation.
Curve B shows the stress from drug side effects against drug dosage. At low dosage no side effects are present. At low dosage the body breaks down all of the drug into harmless chemicals for excretion. As the drug dosage increases the body is not able to breakdown all of the drug into harmless chemicals and the drug breakdown products begin to build up in the body causing side effects. The stress caused by drug side effects increases exponentially because the drug is building up in the body and potentially harmful breakdown products are building up faster than they can be removed.
Curve A shows the decreasing stress from health disability against drug dosage because the drug has a beneficial effect on the health disability. The red curve ‘C’ takes the stress of the health disability and the stress of drug side effects added together. It can be seen that there is a decreasing stress and then the stress begins to rise. This point where the curve just begins to rise is the “Optimum Drug Dosage”.
The point of optimum drug dosage is a variable quantity. It will vary from patient to patient and be affected by external events that the patient is subjected to. For example: I have a chronic pain condition. When the weather changes to a certain type of dampness my pain condition changes significantly. I don’t take pain killers, but if certain types of weather affect me badly I can reasonably deduce that if I was on medication that the optimum dose for my condition would change according to the weather.
How is the optimum dosage determined? I do not know the answer to this. It is something that is difficult to determine from what is written on drugs. Some drugs have their dosage determined by blood testing. This only tells how much of a particular chemical is in the blood. It says nothing about the stress from side effects or the stress of the health disability nor does it say anything about how fast the drug is absorbed. The absorption rate of the drug is related to how it is administered, injection, pessary, tablet or liquid.
Even then it may have complications. Drugs are made in batches. There is a variability between one batch and another. A drug manufacturer may decide to change how a drug is made. For example there is a drug known as digitalis which is used to treat a heart condition. There is a problem known as Digitalis Toxicity. This can suddenly appear because the person has developed low magnesium levels or has a kidney infection. There was a situation a number of years ago when the digitalis made by one manufacturer was subtly changed. The quantity of digitalis in the tablet and the purity of the tablet was the same. However the tablet was composed of finer digitalis particulate. This resulted in the tablet dissolving faster and the patient received a much higher dose after taking their tablets than what they had before. Many patients died as a result before the medical profession realised that there was a problem.
Another example I have come across relates to insulin injections. A person I know had adapted to taking insulin over a number of years and they could predict to a fair amount of certainty how much they needed and when they needed it. They were a car driver. The insulin formulation was changed. The person was not informed of the change in formulation and they took the new batch of insulin the same way they had taken the old batch. They got in their car and drove to some event. On the motorway the car had to be boxed in by three police cars to protect them and other members of the public from their highly dangerous driving. The insulin they took had affected their mental capacity quite badly and they was unaware of it. They were fined £150 in court for dangerous driving which was caused by the medical profession changing the insulin formulation without telling them.
There is a problem concerning the combination of pain killer and anxiety meditation. The doctors had prescribed pain medication at the recognised dose that caused no problems. The patients at a later date were prescribed medication for their anxiety condition. Again at the correctly recognised dosage. The patients died from suffocation. The anxiety medication increased the effectiveness of the pain medication in paralysing the breathing system. Each medication by itself had presented no problems. The meditations together killed people and the doctors were unaware of this effect until after the event.
fda.gov/downloads/Drugs/Dru...
medshadow.org/features/drug...
drugabuse.gov/drugs-abuse/o...
self.com/story/medications-...
lhsfna.org/index.cfm/lifeli...
Oxycodone is a pain killer. Using data at en.wikipedia.org/wiki/Oxyco....
Oxycodone is metabolized by the enzymes CYP3A4 and CYP2D6, and its clearance therefore can be altered by inhibitors and inducers of these enzymes. (For lists of CYP3A4 and CYP2D6 inhibitors and inducers, see
en.wikipedia.org/wiki/CYP3A...
and
en.wikipedia.org/wiki/CYP2D...
respectively.) Natural genetic variation in these enzymes can also influence the clearance of oxycodone, which may be related to the wide inter-individual variability in its half-life and potency.
Drugs have other complications. They can change in effectiveness. Over a period of time the dosage needed to have the same effect may need to be increased. If the drug needs to be changed and the person has been on the drug for a long time there is the problem of addiction. The body has been on the drug for a long time and has made adaptations to accommodate the drug. When the drug is withdrawn the body is still making adaptations for a drug it is expecting. This causes withdrawal symptoms. The nature of the withdrawal can vary from person to person and from drug to drug and the length of time a person has been on the drug.
There is also the human microbiome. The microbiome in the human digestive system could play a part in the processing of drugs. The microbiome varies from person to person. So the microbiome processing of drugs will vary from person to person. See ncbi.nlm.nih.gov/pmc/articl...
The lower graph is a graph of Stress Performance curve for Human Body System. This shows the Stress Breakdown Point where the performance drops considerably for a slight increase in stress. The Stress Breakdown Point can change the curves of the top graph if it is exceeded. A drug may cause the Stress Breakdown Point to decrease without the person with the long term health disability knowing.
I have written in approximations partly because different data sets give different results. Different people have different responses and it is impossible to know someone’s response to medication without some form of experimentation and investigation. There needs to be a way to enable people who have capacity to investigate their own condition to have the tools to do so. And be educated to do so.
I have been told on a number of occasions by professional people that because I do not take pain killers I do not suffer pain. I have extended discs in the neck. A very slight bit of discomfort in the neck causes massive pain in my arm. Varying pressure in my neck on nerve roots causes all sorts of differing effects in my arm. I have learnt that I need pain and discomfort to detect that I am applying unwholesome pressure to nerve roots. It is known that continual pressure on a nerve will damage the nerve. It is important to me to be able to continue doing things with both arms. So I need to avoid pain killers to keep both arms functioning. I have to explain this to medical doctors. This I find disconcerting for I expect them to know.
I hope I have given information for helping people to handle people’s present health disabilities in discussions with the medical profession. Critical comments will be gratefully received. There is always a possibility that what I have written may not have been understood the way I intended.
