Hi all
I have several previous posts about my thyroid- I feel I’ve had thyroid symptoms for years then had to have a hemi-thyroidectomy in Feb 20 due to multi-nodular goitre. I started Levo shortly afterwards when my symptoms started increasing and my TSH increased to over 6.
I saw an endo privately in Oct as I still wasn’t feeling great and I had tried to optimise all my Vits as much as I could. At that time I was on 75mcg Levo and my results were Oct 20: TSH 1.98 (0.27-4.2) Ft4: 16.6 (12-22). My Vit D was 70.
The endo increased Levo to 100mcg and asked me to retest end of Jan, he said the aim is to get your TSH under 1 which I thought was surprisingly sensible! He said if that doesn’t work we could try adding T3.
So, I’ve now been on 100mcg Mercury Pharma Levo for 10 weeks, I’ve been taking good quality B12, B complex and Vit D (I stopped the B well before testing). But I haven’t been feeling that great again. I’ve just got my latest results back, and my TSH hasn’t moved, and my FT3 and FT4 are both falling again! I’m really confused. When I first started Levo I seemed to respond really well.
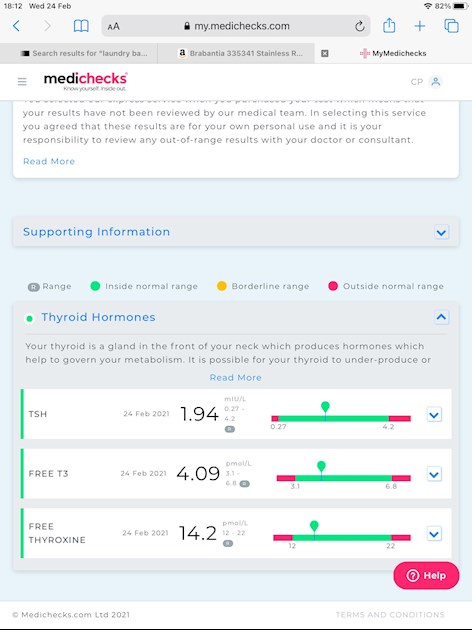
The latest result is in the photo. And below is the result from before I was on Levo at all, just for reference:
Jun 20: TSH 6.1 (0.27-4.2) FT3 4.5 (3.1-6.8) FT4: 13.2 (12-22)
Thyroglobulin abs 11.3 (<115) TPO abs <9 (<34)
Sorry it’s so long. Wonder if anyone can make sense of it. And before anyone asks, I’m not gluten free, no. 😢
