Hello all, my favorite wise forum friends! Long post, but here it goes. Nothing like a slightly desperate mom to just lay it all out there!
Can you believe I have been patient for a whole year! Optimizing vitamins! Which has been tough watching my girl be tired all the time, and dipping in and out of limiting fatigue and regular headaches, all while in her first year at university. Periods irregular. Recently have identified random very high/jumpy heartrate... POTS-like when she gets up sometimes (like from 80 to 150 in a minute upon standing). Sometimes she's doing "better" (I know she's working hard, and seeing her friends) but she's never "good" and is truly tired all the time. She describes that familiar body-shutting-down fatigue feeling that we all know so well.
1 year ago I wrote this: healthunlocked.com/thyroidu...
All gave advice that I took, and would love your and EVERYONE'S input.
Please help!!!!
QUESTIONS:
* What would you do?
* Buddy195 had suggested a 3 month trial of levo a year ago... I'm about ready to try it at this point... I know it's important to find out WHY her numbers are the way they are.... but in any case, they are LOW and I'd sure love to replace her thyroid hormone to help her. LynLyn Your comments stuck with me... any life experience to share now?
* Fluctuations over time... early signs of a failing thyroid? Or could it just be ferritin? Or something else entirely?
* Conversion has taken a hit... will prob add selenium now but can't imagine it would actually fix the intensity of her symptoms (???)
* I'm pursuing an iron infusion to bring her ferritin up... it's hard (even in the US!) to find a knowledgeable dr. but still trying. I want to address this in ANY case, as it needs to come up. But not convinced it's the CAUSE... possibly an effect of low thyroid impacting absorption.
* Her low TSH of 1 is throwing me off.... pituitary?? temporary?? Or actually NORMAL???? I may look to get a pituitary scan, but can't imagine it's that. Despite... her Free Ts are still on the low side. Is it SlowDragon or greygoose who has had advice on secondary hypo?
* IS THERE ANYTHING I HAVEN'T TRIED???? It's hard to wait. It's hard to watch her be so down.
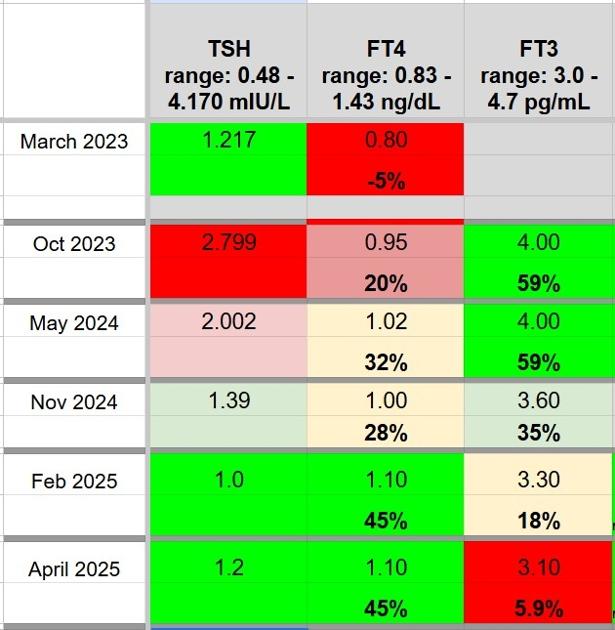
BLOOD TEST RESULTS HISTORY - see picture.
HEALTH HISTORY:
* No diagnosis, No antibodies
* Thyroid scan last summer all normal
* No celiacs
* Did 6 point saliva cortisol a year ago and nothing stood out to me; Have done sex hormone panel and nothing stood out. Both of these I've concluded are not the CAUSE but could be impacted by low thyroid... or low ferritin.
* Supplementing 2x Thorne b complex a week, 5000 D+K daily, and we've moved key vitamins to near/optimal; results since May 2024 have been between:
B12 - 550-730
Folate - 10-20
D - 40-55 ( ng/mL so this is optimal)
Also takes magnesium daily
* Supplementing 2x Three Arrows weekly... Circulating iron and FBC is absolutely Goldilocks perfect; remaining problem... ferritin, although improving from 5 to 35, is still too low.
Thanks to everyone as always.
")