I am 39 years old and was diagnosed with hypothyroidism just over 2 years ago after going for a blood test for fatigue. No other symptoms than that at the time.
Last July I went to the GP as felt ill- tingling in the arms, weakness, headaches- my TSH was 12.6 so the original prescription was increased from 25mg to 50mg of levothyroxine.
I went back in November for a blood test with a TSH of 5.25- despite feeling fine I was increased to 75mg. Within around 2 weeks of the dose increase I experienced lower back pain which and sore wrists which at the time I didn’t connect to this possibly being related to the dose increase. Back pain hasn’t been an issue before.
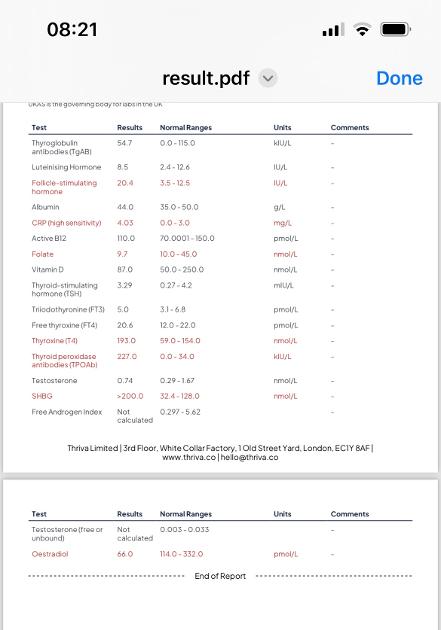
In January this year I had a Thriva blood test as just didn’t feel right with fatigue, continuing back pain, ringing ears and tingling hands and forearms. The results are attached.
In light of struggling to get an appointment with my GP to discuss the results I arranged an appointment with a private thyroid clinic who based on how I was feeling and the Thriva results increased my dose to 100mg (I take the 75mg from GP and 25mg of a different brand to make up the 100mg). They want to review my bloods in 3 months. They also suggested taking vitamin D, selenium and zinc and folate which I am implementing. I have been on the 100mg for just 2 weeks and still don’t feel great (patience is not my thing).
I have also finally managed to get a telephone appointment with my GP but really at a loss as to what I should be asking for and if my dose is too high or whether I just need to give a few months for the 100mg to kick in.
I have no other “known” medical conditions other than vitiligo which I have had since the age of 11. I am at a loss as to what I should be suggesting to the GP- is the increase in dose causing side effects/ making me feel worse? Looking for some direction.
Written by
Zanne60
To view profiles and participate in discussions please or .
High TPO antibodies confirms autoimmune thyroid disease also called Hashimoto’s
About 90% of primary hypothyroidism is autoimmune thyroid disease, usually diagnosed by high TPO and/or high TG thyroid antibodies
Autoimmune thyroid disease with goitre is Hashimoto’s
Autoimmune thyroid disease without goitre is Ord’s thyroiditis.
Both are autoimmune and generally called Hashimoto’s.
Are you in U.K.
In U.K. medics hardly ever refer to autoimmune thyroid disease as Hashimoto’s (or Ord’s thyroiditis)
Essential to test and maintain GOOD vitamin D, folate, ferritin and B12
For good conversion of Ft4 (levothyroxine) to Ft3 (active hormone) we must maintain GOOD vitamin levels
Exactly What vitamin supplements are you taking
They also suggested taking vitamin D, selenium and zinc and folate which I am implementing
No other medication or supplements at same as Levothyroxine, leave at least 2 hour gap.
Some like iron, calcium, magnesium, HRT, omeprazole or vitamin D should be four hours away
(Time gap doesn't apply to Vitamin D mouth spray)
So January test results above were when on 75mcg daily
Recommended that all thyroid blood tests early morning, ideally just before 9am, only drink water between waking and test and last dose levothyroxine 24 hours before test
This gives highest TSH, lowest FT4 and most consistent results. (Patient to patient tip)
Is this how you did this test ?
I have been on the 100mg for just 2 weeks and still don’t feel great (patience is not my thing).
No point seeing a consultant until you have new test results after 8-10 weeks on 100mcg
Which brand of levothyroxine is your 75mcg and which brand is 25mcg
Many people find different brands are not interchangeable
Poor gut function with Hashimoto’s can lead leaky gut (literally holes in gut wall) this can cause food intolerances.
Most common by far is gluten.
Dairy is second most common.
A trial of strictly gluten free diet is always worth doing
Only 5% of Hashimoto’s patients test positive for coeliac but a further 81% of Hashimoto’s patients who try gluten free diet find noticeable or significant improvement or find it’s essential
A strictly gluten free diet helps or is essential due to gluten intolerance (no test available) or due to leaky gut and gluten causing molecular mimicry (see Amy Myers link)
Changing to a strictly gluten free diet may help reduce symptoms, help gut heal and may slowly lower TPO antibodies
While still eating high gluten diet ask GP for coeliac blood test first as per NICE Guidelines
The predominance of Hashimoto thyroiditis represents an interesting finding, since it has been indirectly confirmed by an Italian study, showing that autoimmune thyroid disease is a risk factor for the evolution towards NCGS in a group of patients with minimal duodenal inflammation. On these bases, an autoimmune stigma in NCGS is strongly supported
In summary, whereas it is not yet clear whether a gluten free diet can prevent autoimmune diseases, it is worth mentioning that HT patients with or without CD benefit from a diet low in gluten as far as the progression and the potential disease complications are concerned
Despite the fact that 5-10% of patients have Celiac disease, in my experience and in the experience of many other physicians, at least 80% + of patients with Hashimoto's who go gluten-free notice a reduction in their symptoms almost immediately.
Similarly few months later consider trying dairy free too. Approx 50-60% find dairy free beneficial
With loads of vegan dairy alternatives these days it’s not as difficult as in the past
Igennus B complex popular option. Nice small tablets. Most people only find they need one per day. But a few people find it’s not high enough dose and may need 2 per day and/or may need separate methyl folate couple times a week
IMPORTANT......If you are taking vitamin B complex, or any supplements containing biotin, remember to stop these 5-6 days before ALL BLOOD TESTS , as biotin can falsely affect test results
In week before blood test, when you stop vitamin B complex, you might want to consider taking a separate folate supplement (eg Jarrow methyl folate 400mcg)
Thankyou so much for your time and informative reply; as to your questions-
1-UK based- yes although I have never discussed the condition with my GP, even when diagnosed. I was told it was as simple as take the prescribed Levo and you will be fine. This is why in Jan I got my own Thriva test and then spoke to a thyroid clinic. I wanted to be better informed.
2) Supplements- started taking Pharma Nord combined zinc and selenium about a fortnight ago , vitamin D (2000 IU) and folic acid (note you say the latter shouldn’t be needed- should I stop taking this? ).
I also periodically take magnesium and omega 3 as per Thriva’s advice and MSM. I don’t take anything within 4 hours of the levo other than lemon water and after an hour a couple of boiled eggs for breakfast. I do take the contraceptive pill about half a hour after the levo- is that a problem? Take the supplements at night after dinner. I think it is sensible what you say re B vitamins and will order some. It is strange getting used to the volume of supplements but if it helps me….
3) Timing of blood test- the last one was about 6.30am (Thriva where I screen shotted the results) and hadn’t taken that days Levo. Wouldn’t have been on any supplements other than MSM. When the GP take bloods it’s whenever they can fit me in and offer no advice re timing.
4) Brand- the 75mg are Teva and 25mg Wockhardt. I always used to request Wockhardt when I was on 25mg as I thought I got on better with that. With the 75mg it differs as to what brand I pick up from the pharmacy each month. Would I be better asking for 4x 25mg of Wockhardt?
5) Diet- my husband eats a dairy and gluten free diet and I eat what he eats save for the odd slice of cheese. I would say I have a healthy diet.
6) Ferritin- I didn’t get that tested with Thriva (I was trying to best work out what I needed to test for) but my July 2024 GP result said this was low and to eat more red meat etc. The NHS app doesn’t give a figure.
Again Thankyou so much for your time and help- if there is anything you can add to the above please do.
Many patients do NOT get on well with Teva brand of Levothyroxine.
Teva is lactose free, but contains mannitol as a filler instead of lactose, which seems to be possible cause of problems. Mannitol seems to upset many people, it changes gut biome
If a patient reports persistent symptoms when switching between different levothyroxine tablet formulations, consider consistently prescribing a specific product known to be well tolerated by the patient.
Physicians should: 1) alert patients that preparations may be switched at the pharmacy; 2) encourage patients to ask to remain on the same preparation at every pharmacy refill; and 3) make sure patients understand the need to have their TSH retested and the potential for dosing readjusted every time their LT4 preparation is switched (18).
1-UK based- yes although I have never discussed the condition with my GP, even when diagnosed. I was told it was as simple as take the prescribed Levo and you will be fine.
Well that’s what many of us were told
You were started on too low a dose and left far too long on only 25mcg Levo
Standard starter dose is 50mcg and bloods retested every 2-3 months and dose should be increased as fast as tolerated to bring TSH below 2
Most patients on levothyroxine find their symptoms improve when TSH around 1
Thankyou, I really do hate having to medicate, it takes me all my time to take a painkiller for a headache but I understand I will need the Levo to function. I did like the Wockhardt so may try and battle to have that.
I do wonder if there is a conversion issue from T4 to T3 as Northen Light’s says as I literally feel like I am being mildly poisoned following the dose increase but I know messing around with it without supervision or making drastic changes can cause more issues.
Thankyou, I did wonder this. I am going to try and discuss with my GP- I am not sure whether this ties in with the thyroid issues or is entirely separate.
When my estrogen is too low the first symptoms I get are achy stiff joints and sore weak muscles, especially first thing in the morning or after sitting awhile.
Edited to add: early on I used to get headaches that lasted all day or a few days that coincided with hormone changes around ovulation. My body didn't handle well the more dramatic changes of early perimenopause.
Sorry to hear that- this isn’t fun is it! If it’s a sign of peri menopause I can process that but part of me wonders if the higher dose in levo has caused more of the problems due to the timing of the increase and worsening symptoms over a period of around 3 months.
That really makes sense; Thankyou - I feel like since the Levo went above 50mg in November 2024( firstly to 75mg and then 100mg towards the end of Jan 2025) I have had new symptoms and worsening fatigue. I gave the benefit of the doubt when they said they levo had to go up again; I listened to the “experts” but my gut tells me the increase in dose has created the odd sensations/ feeling rough.
Newness wise my fingers are swelling at night hence feel stiff and occasionally wrists and forearms and now the same with my toes and feel flushed/ itchy which is really strange almost like an allergy, ringing ears too. My lower back pain seems to have come about two weeks or so after the levothyroxine increase to 75mg and it’s on both sides, normally it’s just my right side occasionally when I sit dodgily on my office chair.
I felt I didn’t have enough knowledge to argue with the suggested increase in dose but other people’s experiences on here are really helping and I think the levo being too high resonates - as you say the differential between the T3 and T4 is big. I literally feel like it’s an allergy/ my body isn’t happy with the amount of Levo. I don’t normally have any health issues beyond the fatigue and a bit of a dodgy knee from years of running.
I have a Gp telephone appointment on 4th and I am going to ask for a referral to an endocrinologist and I think I will ask if I can be reduced down and supplement T3 which I didnt even know they could do. I am just hoping the side effects disappear when the Levo dose drops!
I went to the pharmacy this morning to collect the next set of tablets pending my appointment on 4th March- guess what …. Teva, rejected them and asked for something else.
Thankyou, it really is much appreciated and glad you got sorted in the end- I thought it seemed more than a coincidence.
It sounds like being pro active is the way forward- the first step will be getting the GP to refer me to an endocrinologist ( I will go private if needs be) as I’m guessing the GP wont want to comment - roll on 4th March!
low vitamin d can cause aches all over and fatigue and it also lowers your immune system but you can only go by blood test w thyroid to actual see if the meds are pushing your higher or not and to test your antibodies . I must say the ringing in the ears is something i have struggled w for years since taking thyroid meds and it is very annoying.
It seems to be the dose increased and ringing started. It seems like a process of trial and error to get what works for you. Hopefully the vitamin d will help with the fatigue and aching.
When in your cycle was your test taken as your FSH is high. Also what kind of contraception are you taking as sex hormone imbalances also affect thyroid and can cause a lot of symptoms similar to hypothyroidism. It would be also really useful to check your progesterone level though might be difficult on NHS.
Hi it was taken on the morning of day 2 of my period. I take the combined pill Gedarel 20/150. The timing was as per Thriva’s recommendation. It really isn’t straightforward trying to unravel the whole balance thing with hormones. I am not sure what I would do with the pill/ balancing of sex hormones.
Content on HealthUnlocked does not replace the relationship between you and doctors or other healthcare professionals nor the advice you receive from them.
Never delay seeking advice or dialling emergency services because of something that you have read on HealthUnlocked.