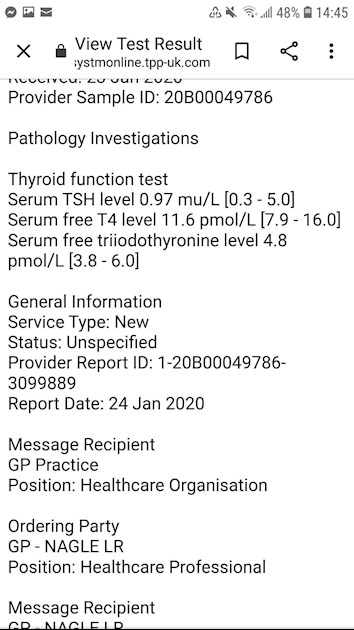
Hi all, I increased levo dose from 50 to 75mcg around 2 months ago. I am trying to get optimal as not ovulating regularly and trying for our second baby for over a year now :/ i have been prescribed Clomid but want to see if can sorting thyroid first. My tsh has gone from 2 to 0.9 which am pleased about but my t3 is 4.8 so not optimal and wonder if i need t3 to add to t4 but understand before adding t3 need to get vitamin levels optimal to see if that is hindering conversion process. Attached are thyroid results and below are some other blood test results, i would be grateful for some feedback thanks:
B12 337ng/L (120 - 900)
Ferritin 22ng/mL (15-300)
Folate >20ug/L (2.5 - 9999)
ALT 57uL (0.0 - 35.0)
Mean cell haemoglobin levels 32.1 (27 -32)
Serum calcium 2.16mmol/L (2.2-2.6)
Plasma fasting glucose 4.9mmol/L (3.5-6)
Written by
Ljdaly74
To view profiles and participate in discussions please or .
Good conversion takes place when the ratio is around 3:1, over 4:1 can suggest poor conversion. Your ratio of 2.42 : 1 shows good conversion.
It's not T3 that you need, it's an increase in Levo that is needed to raise your FT4 which, because of your good conversion, will also raise your FT3.
Your GP may be reluctant to increase your Levo. You can use this information to support an increase:
Dr Toft, past president of the British Thyroid Association and leading endocrinologist, states in Pulse Magazine (the magazine for doctors):
"The appropriate dose of levothyroxine is that which restores euthyroidism and serum TSH to the lower part of the reference range - 0.2-0.5mU/l. In this case, free thyroxine is likely to be in the upper part of its reference range or even slightly elevated – 18-22pmol/l. Most patients will feel well in that circumstance. But some need a higher dose of levothyroxine to suppress serum TSH and then the serum-free T4 concentration will be elevated at around 24-28pmol/l. This 'exogenous subclinical hyperthyroidism' is not dangerous as long as serum T3 is unequivocally normal – that is, serum total around T3 1.7nmol/l (reference range 1.0-2.2nmol/l).*"
*He recently confirmed, during a public meeting, that this applies to Free T3 as well as Total T3.
You can obtain a copy of the article by emailing Dionne at
tukadmin@thyroiduk.org
print it and highlight question 6 to show your doctor.
**
B12 337ng/L (120 - 900) - ng/L is the same as pg/ml
Too low, but your GP wont be bothered because it's within range.
According to an extract from the book, "Could it be B12?" by Sally M. Pacholok:
"We believe that the 'normal' serum B12 threshold needs to be raised from 200 pg/ml to at least 450 pg/ml because deficiencies begin to appear in the cerebrospinal fluid below 550".
"For brain and nervous system health and prevention of disease in older adults, serum B12 levels should be maintained near or above 1000 pg/ml."
Do you have any signs of B12 deficiency - some people with a level in the 300s have been found to need B12 injections. Check here:
If you do then list them to discuss with your GP and ask for testing for B12 deficiency and Pernicious Anaemia.
**
Folate >20ug/L (2.5 - 9999)
This is good, do you supplement?
**
Ferritin 22ng/mL (15-300)
This is very low at just 2.46% through range. I would point out the percentage through range to your GP because he will say there is no problem as you are within range at 22.
**
Mean cell haemoglobin levels 32.1 (27 -32)
This is part of a full blood count. Were MCV, haemoglobin, haematocrit measured? Did you have an iron panel to include serum iron, transferrin saturation %, TIBC? These would determine if you have iron deficiency or iron deficiency anaemia, which low ferritin can suggest.
**
It would also be a good idea to test Vit D.
**
ALT 57uL (0.0 - 35.0)
Serum calcium 2.16mmol/L (2.2-2.6)
These out of range results should be discussed with your GP.
Wow thank you for all this info. Re the ALT gp just said wouldn't worry probably caused by raised bmi! The calcium they rounded up so is just within range. But will check.
Will ask for Vit D.
What can they give for low ferritin? Iron supps?
Didnt have iron panel tested.
Haematocrit 0.4L (0.37 - 0.46)
Yes do supplement folate - 5mg folic acid.
B12, i do have a few of the symptoms namely infertility as not ovulating?! Will speak to GP. Since these tests i have been taking Vit B- Complex Howard & James supplements. Would these help?
Good to know re, T3. I can try and ask increase of levo from 75 to 100mcg but doubt will get far as had to beg to go from 50 to 75!
Do you think should still hold off Clomid until get more optimal?
No, it's not as simple as that. Iron is complicated which is why it's best to get an iron panel and full blood count done.
If your iron panel shows a good level of serum iron then taking iron tablets for low ferritin would possibly push your serum iron up too high, and high iron is as bad as low iron.
So the iron panel will show if there is iron deficiency.
A full blood count will show if there is anaemia.
If everything else is OK but you just have low ferritin - which is what I have (good iron panel, good full blood count, low ferritin) then what helps me to raise ferritin is eating liver (or liver pate, black pudding has the same effect). Limit for liver is 200g per week due to it's high Vit A content. This is how I have raised my ferritin in the past without my iron panel going haywire. This isn't to say it will be exactly the same for everyone. If I stop eating liver my ferritin lowers again.
Yes do supplement folate - 5mg folic acid.
Is your GP going to continue with the prescription now that you have a good folate level?
B12, i do have a few of the symptoms namely infertility as not ovulating?! Will speak to GP.
You can't test for B12 deficiency whilst taking folic acid/folate as these mask signs of B12 deficiency.
Since these tests i have been taking Vit B- Complex Howard & James supplements. Would these help?
I've not heard of this brand so have checked it out. Personally, I wouldn't recommend it. A good B Complex will say "bioavailable" or "bioactive" which means that it contains the bioavailable forms of active ingredients that don't need converting by the body, in particular it will contain methylfolate (not folic acid) and methylcobalamin (not cyanocobalamin). That brand has 2.5mcg cyanocobalamin B12 which wont do anything at all for a low level. You would need at least 400mcg, maybe more, depending on your current level. Good bioavailable brands recommended here are Thorne Basic B (I use this brand) and Igennus Super B.
Also, as far as B Complex is concerned, they all contain Biotin (B7) so need to be left off for 7 days before any blood test - including thyroid tests. This is because Biotin is used in most testing machines and if we also take Biotin (either as a stand alone supplement or in a B Complex) then this can give false test results.
Do you think should still hold off Clomid until get more optimal?
I'm sorry but this is something I can't comment on, I have no knowledge at all about this.
Re: You can't test for B12 deficiency whilst taking folic acid/folate as these mask signs of B12 deficiency.
The 5mg folic acid part of my trying to conceive treatment plan. I would have been taking these when had the b12 test. Does make result void and should the result have been better than it was if was being supplemented?!,
It masks the signs of B12 deficiency, I don't know if it affects results. Maybe you can check out signs-and-symptoms of B12 deficiency I linked to and see if you can remember anything from before you started the folic acid.
Ah ok thanks. Just another quick question, with an increase in levo do you see bulk of any difference/improvement in levels over the immediate follow on couple of months or will it continue improving after that?
Changes in dose of Levo can take up to 6 weeks to be fully effective and for us to feel the difference. This is why we suggest waiting 6-8 weeks for levels to stabilise before retesting. Some of us need even longer than that. As far as test results go don't forget that a blood test is a snapshot of what's happening at the exact time the blood is drawn. Levels change all the time based on time of day (there is a circadian rhythm with hormones) and, of course, the time of the last dose of Levo taken before the test.
* Book the first appointment of the morning, or with private tests at home no later than 9am. This is because TSH is highest early morning and lowers throughout the day. If we are looking for a diagnosis of hypothyroidism, or looking for an increase in dose or to avoid a reduction then we need TSH to be as high as possible.
* Fast overnight - have your evening meal/supper as normal the night before but delay breakfast on the day of the test and drink water only until after the blood draw. Eating may lower TSH, caffeine containing drinks affect TSH.
* If taking thyroid hormone replacement, last dose of Levo should be 24 hours before blood draw, if taking NDT or T3 then last dose should be 8-12 hours before blood draw. Adjust timing the day before if necessary. This avoids measuring hormone levels at their peak after ingestion of hormone replacement. Take your thyroid meds after the blood draw. Taking your dose too close to the blood draw will give false high results, leaving any longer gap will give false low results.
* If you take Biotin or a B Complex containing Biotin (B7), leave this off for 7 days before any blood test. This is because if Biotin is used in the testing procedure it can give false results (most labs use biotin).
These are patient to patient tips which we don't discuss with doctors or phlebotomists.
I have no idea why this is the case, but I have often noticed that when people report a single liver function test result as being out of range it always seems to be ALT that is high.
It's happened to me. My ALT was high a couple of years ago but then returned to completely normal (roughly mid-range) in the tests I have had since.
I imagine high ALT is warning people about something, but what it is I simply don't know.
Vitamin D deficiency is frequent in Hashimoto's thyroiditis and treatment of patients with this condition with Vitamin D may slow down the course of development of hypothyroidism and also decrease cardiovascular risks in these patients. Vitamin D measurement and replacement may be critical in these patients.
Evidence of a link between increased level of antithyroid antibodies in hypothyroid patients with HT and 25OHD3 deficiency may suggest that this group is particularly prone to the vitamin D deficiency and can benefit from its alignment.
Hashimoto's frequently affects the gut and leads to low stomach acid and then low vitamin levels
Low vitamin levels affect Thyroid hormone working
Poor gut function can lead leaky gut (literally holes in gut wall) this can cause food intolerances. Most common by far is gluten intolerance. Second most common is lactose intolerance
According to Izabella Wentz the Thyroid Pharmacist approx 5% with Hashimoto's are coeliac, but over 80% find strictly gluten free diet reduces symptoms, sometimes significantly. Either due to gluten intolerance (no test available) or due to leaky gut and gluten causing molecular mimicry (see Amy Myers link)
Changing to a strictly gluten free diet may help reduce symptoms, help gut heal and slowly lower TPO antibodies
While still eating high gluten diet ask GP for coeliac blood test first or buy test online for under £20, just to rule it out first
Assuming test is negative you can immediately go on strictly gluten free diet
(If test is positive you will need to remain on high gluten diet until endoscopy, maximum 6 weeks wait officially)
Trying strictly gluten free diet for 3-6 months
If no noticeable improvement, reintroduce gluten and see if symptoms get worse
Getting vit D tested when getting progesterone tested (day 21 of cycle so not long now, is difficult to find vein so like to group tests!) Have been supplementing vit D for over 4 years now so hoping is ok?!
Yes am hash/hypo tpo was 36 (0 - 5.6 kU/L) back in 2016 drs wont test again as say no point as already know am
hash/hypo?!
Prolactin back then was 315 (<800mIU/L) they didnt say anything about that result.
Interesting read re dose of levo. I am 45.5 and bmi 35 do these factors affect dose too? Increased from 50 to 75mcg few month back, havent noticed any improvement in fact now getting warm fingertips?!
Well according to my maths i should be on 172mcg levo almost 100 more than am on!
Take vit D3 2000iu ne a day tablets igennus pure and essential from Amazon, when is best to take?
At mo is Teva brand but not kept track what have had in past, maybe i should request not teva?
4 vits being vit d, b12, folate and ferritin? Is that right? Folate seems ok as am on 5mg folic acid, b12 and ferritin just in lower range yet to hear re vit d.
B12 likely too low. Obviously Folate looks good as on folic acid supplements
But it might be better to be Supplementing a good quality daily vitamin B complex, one with folate in not folic acid may be beneficial. Rather than just folic acid
B vitamins best taken in the morning after breakfast
Igennus Super B complex are nice small tablets. Often only need one tablet per day, not two. Certainly only start with one tablet per day after breakfast. Retesting levels in 6-8 weeks
Or Thorne Basic B or jarrow B-right are other options that contain folate, but both are large capsules
If you are taking vitamin B complex, or any supplements containing biotin, remember to stop these 7 days before any blood tests, as biotin can falsely affect test results
You can have low ferritin but high iron. Always need full iron panel test for anaemia
Eating iron rich foods like liver or liver pate once a week plus other red meat, pumpkin seeds and dark chocolate, plus daily orange juice or other vitamin C rich drink can help improve iron absorption
Many people find Levothyroxine brands are not interchangeable.
Once you find a brand that suits you, best to make sure to only get that one at each prescription. Watch out for brand change when dose is increased or at repeat prescription.
Many patients do NOT get on well with Teva brand of Levothyroxine. Though it is the only one for lactose intolerant patients. Teva is the only brand that makes 75mcg tablet. So if avoiding Teva for 75mcg dose ask for 25mcg to add to 50mcg or just extra 50mcg tablets to cut in half
Content on HealthUnlocked does not replace the relationship between you and doctors or other healthcare professionals nor the advice you receive from them.
Never delay seeking advice or dialling emergency services because of something that you have read on HealthUnlocked.

 will have to try harder.
will have to try harder.