JULY 2012
PRESS RELEASE
Int J Clin Exp Med 2012;5(3):208-220
Original Article Mitochondrial dysfunction and the pathophysiology of Myalgic Encephalomyelitis/Chronic Fatigue Syndrome (ME/CFS) Norman E Booth, Sarah Myhill, John McLaren-Howard
Department of Physics and Mansfield College, University of Oxford, Oxford UK; Sarah Myhill Ltd, Llangunllo, Powys UK; Acumen, Tiverton, Devon UK Received April 26, 2012; accepted May 21, 2012; Epub June 15, 2012; Published June 30, 2012
Abstract: The objectives of this study are to test the hypothesis that the fatigue and accompanying symptoms of Chronic Fatigue Syndrome/Myalgic Encephalomyelitis are in part due to defects in energy provision at the cellular level, and to understand the pathophysiology of the defects so that effective medical intervention can be implemented. We performed an audit of 139 patients (ages 18-65) diagnosed with CFS/ME and attending a private practice. The patients and 53 normal, healthy controls had the ATP Profile test carried out on neutrophils from a 3-ml venous blood sample. This test yields 6 numerical factors that describe the availability of ATP and the efficiency of oxidative phosphorylation in mitochondria. Other biomedical measurements, including the concentration of cell-free DNA in plasma, were made. The results of the audit are compared with the controls and a previous cohort of 61 patients. We find that all patients tested have measureable mitochondrial dysfunction which correlates with the severity of the illness. The patients divide into two main groups differentiated by how cellular metabolism attempts to compensate for the dysfunction. Comparisons with exercise studies suggest that the dysfunction in neutrophils also occurs in other cells. This is confirmed by the cell-free DNA measurements which indicate levels of tissue damage up to 3.5 times the normal reference range. The major immediate causes of the dysfunction are lack of essential substrates and partial blocking of the translocator protein sites in mitochondria. The ATP Profile is a valuable diagnostic tool for the clinical management of CFS/ME. (IJCEM1204005)
Keywords: Chronic fatigue syndrome, myalgic encephalomyelitis, mitochondria, adenosine triphosphate (ATP), oxidative phosphorylation, cellular energetic, glycolysis, cell-free DNA, exercise
Address all correspondence to: Dr. Norman E Booth, PhD FInstP, Emeritus Professorial Fellow in Physics, Mansfield College, University of Oxford, UK. E-mail: n.booth1@physics.ox.ac.uk
Full text available at ijcem.com/files/IJCEM120400...
Dr Norman Booth, Dr Sarah Myhill and Dr John McLaren Howard are pleased to announce the publication of a second paper concerning the link between mitochondrial dysfunction and ME/CFS.
Comment
In 2009 we published our first paper looking at mitochondrial function in ME/CFS patients. What we found is that those patients with the worst mitochondrial function had the worst levels of fatigue and vice versa. There was a very clear relationship between the two. The importance of this paper was that it gave backing to certain treatment interventions and also that it clearly established ME/CFS as a physical condition with physical causes. The mitochondrial function can be used as an objective assessment of fatigue and of course this has obvious practical implications. Hitherto any assessment of the level of disability had to be subjective and this created great difficulties for patients in cases where their physicians disbelieved the serious nature of their symptoms. For a detailed explanation of the clinical issues please see
drmyhill.co.uk/wiki/CFS_-_T...
This second paper further explores the above ideas. In this second paper the size of the patient group is much larger with 138 ME/CFS patients involved. Their mitochondrial function tests were compared with 53 normal healthy controls. The findings of the first paper were repeated and confirmed, but the analysis of this second paper was carried out slightly differently. It was found on careful inspection of the biochemistry that there were various sub-groups of ME/CFS patients with their own characteristic biochemical pattern. In particular, one of the five parameters measured, namely translocator protein function IN, can be higher as well as lower for patients as compared with controls. This second paper also attempts to explain what is happening at the biochemical level to result in such an abnormality. To this end, Dr. Booth provides an alternative method of assessing mitochondrial function. He noticed that the percentage inhibition of ATP closely correlates with TL-in factor – this is probably because the biochemistry of these two measured quantities is so closely associated. So instead of using TL-in to calculate the mitochondrial energy score, he used percentage ATP inhibited – this provided a solution to the problem of translocator protein IN being higher in some patients than in controls, a factor which in itself is abnormal.
Dr. Booth then went on to plot the relationship between mitochondrial energy score and the number of factors within the normal region to achieve an extremely close correlation. Importantly this test identifies a clean separation between the ME/CFS cases and the healthy controls.
So this first part of the paper very much confirms the work of the first paper published in 2009 which is that those patients with the worst ME/CFS had the worst mitochondrial function and vice versa.
It must be remembered that patients attending a clinic for ME/CFS are usually the most severely fatigued – no mildly ill patients were tested. Within these limitations the ATP profile is an exclusive and sensitive test for ME/CFS. However, we cannot claim that it is specific to ME/CFS because there are many other neurological illnesses and metabolic syndrome also associated with mitochondrial dysfunction.
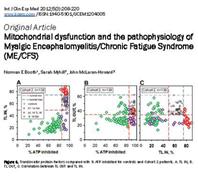
Dr Booth went on to analyse sub-groups within the main group. When mitochondria are stressed, i.e. energy demand exceeds energy delivery, in the short term they can switch into an alternative means of making ATP, of which there are 2 possibilities identified. Dr. Booth called these patients cohort 1 and cohort 2. In cohort 1, the mitochondria switch into anaerobic metabolism with increased glycolosis in order to produce ATP.
In cohort 2 there was an alternative process to supply additional ATP. This alternative process involves the adenylate kinase reaction in which two molecules of ADP combine to make one of ATP and one of AMP. The problem with this reaction is that for every molecule of ATP generated, so is one of AMP. This is not recycled, but mainly lost in the urine. So there may be short term metabolic benefits here, but in the longer term metabolic disaster ensues as the energy molecules literally leak away. It takes time to replace these leaked molecules of ADP (leaked in the form of a ‘lost’ AMP molecule) and so this may explain one of the clinical features of ME/CFS, namely delayed fatigue.
A vital feature of ATP studies is that they identify the mechanisms by which mitochondria ‘go slow’. Essentially they can ‘go slow’ for one of three common reasons, either there is substrate deficiency, i.e. lack of essential co-factors for mitochondria to work such as Co-enzyme Q10, magnesium, vitamin B3, or acetyl-L-carnitine, or secondly, because mitochondria are blocked by toxins. Typically the blockage can be of oxidative phosphorylation and/or translocator protein function. Dr John McLaren Howard has developed several further tests to look at the nature of these blockages. These tests include microrespirometry studies, translocator protein function studies, intracellular calcium studies and so on. The third possible mechanism for mitochondria malfunctioning has to do with membrane function. The membranes of mitochondria need to be of just the right consistency in order to hold the bundle of enzymes in the correct 3D configuration to allow efficient movement of substrate from one enzyme complex to another. To this end, again Dr John McLaren Howard has developed cardiolipin studies which look in more detail at mitochondrial membrane structure and function.
Many of the above tests have been available in research laboratories, some John has developed through his own brilliance and initiative. What is so wonderful is how he has given these cutting edge research tests a clinical application. This is extremely helpful for patients and clinicians because we can see exactly why mitochondria are ‘going slow’ and thereby correct deficiencies using both nutritional supplements, correct gut function, as well as being able to tailor detoxification regimes to individual patients.
This second paper also goes on to look at cell free DNA in ME/CFS patients. Cell free DNA is a measure of DNA in the bloodstream that is not bound up within cell membranes. It can only, therefore, come from damaged cells and therefore is a measure of cell damage within the body. What we found is a strong negative correlation with mitochondrial energy scores, ATP levels and the rate of oxidative phosphorylation. What this means is that those patients with mitochondria that perform extremely poorly have the highest level of cell damage and vice versa. This makes perfect biochemical sense – if mitochondria ‘go slow’ one can expect there to be the production of free radicals which have the potential to damage tissues. Therefore addressing these issues of poor antioxidant status is an essential part of the package of treatment for ME/CFS patients. These abnormal results clearly show that the effect on mitochondria is a systemic effect, not just confined to the neutrophils that are being tested. Very often we see levels of cell free DNA of a similar magnitude to those in patients who are experiencing a serious illness such as cancer, stroke, autoimmunity, or severe viral infection. Again this underpins the fact that ME/CFS is a physical condition with clear indications of marked cell damage. This puts ME/CFS firmly in the realm of major organic pathology.
Implications for the treatment of ME/CFS
These bio-medical tests have been extremely helpful in the diagnosis and management of ME/CFS patients. This is because they clearly identify the biochemical lesions that underpin the cause of this illness. Furthermore, identification of these lesions has clear implications for management using the standard methods of nutritional and environmental medicine. We are currently preparing a third paper which looks at the efficacy of these interventions in patients by measuring mitochondrial function tests before and after such interventions and correlating these with the clinical picture. For further information as to what these interventions are please see drmyhill.co.uk/wiki/CFS_-_C... which is available on line without charge.
")