(I have also posted this on the thyroid UK forum.)
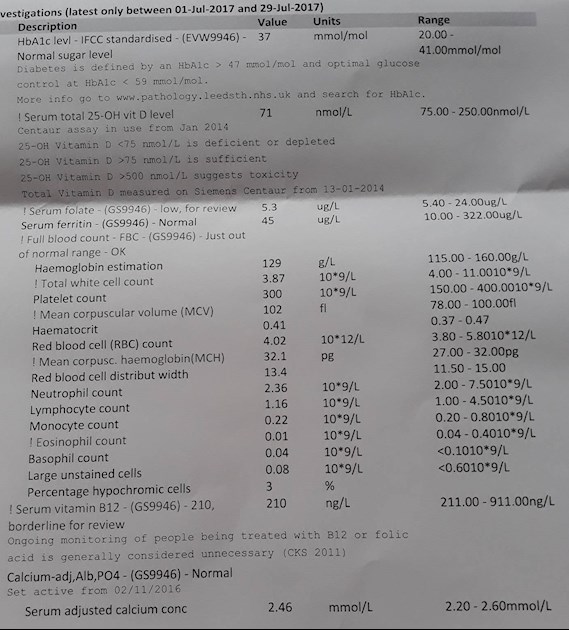
I am writing on behalf of my sister for some advice. She was diagnosed with autoimmune hypothyroidism a couple of years ago and has mostly been feeling well. However, in the last few months she has been feeling very tired, her hair has been falling out, she can't lose weight, etc. She had some bloods done and what I think are the most significant results are below. She also had a thyroid function test, but it was only TSH (result was 0.08, range 0.2-2.0); no fT4).
What leaps out at me is that she is actually deficient in Vitamin D, folate and B12 (as evidenced by a just-below range reading and over range MCV).
Her GP proposes to treat the folate deficiency alone and observe the B12 levels; they propose to do nothing about the vitamin D deficiency, although this is something my sister has suffered from on a regular basis.
We are going on holiday together to France shortly and I have said that I am happy to pay for her to have some private bloods done while we're there as it's very easy and pretty cheap. What should I consider asking for? I thought fT4, gastric parietal cell antibodies, intrinsic factor antibodies.
I note also that her ferritin could be better, although depressingly classed as normal. I will be recommending to her that she self-supplements; what is a good choice for not much money?
I seem to recall reading that treatment of a folate deficiency shouldn't begin if there's a B12 deficiency in the offing as well. Is that right?
As an aside, I carry the MTHFR mutation (compound heterozygous) but it doesn't seem to affect my ability to recycle B12 for some reason; my levels are relatively okay (mostly hovering around 500-600 or so). Might this also be a factor in my sister's problems?
Any advice very gratefully received; she's really not well at the moment.
Written by
hose1975
To view profiles and participate in discussions please or .
If you are going to france you can actually get B12 injections over the counter at the pharmacy though that doesn't get over the fact that your GP is not treating your sister correctly.
Macrocytic anaemia - larger rounder red blood cells - is caused by both B12 and folate deficiencies.
Please refer him to the BCSH guidelines on diagnosis and treatment of cobalamin (B12) and folate deficiencies. They can access them through the BNF but you can also see them here
if your sister has neurological symptoms then B12 deficiency needs to be addressed now.
folate deficiency should not be treated in preference to a B12 deficiency - ideally B12 should be addressed by starting B12 loading shots 24-48 hours before starting treating folate deficiency.
Serum B12 used as a single marker will miss 25% of people who are B12 deficient (and also pick up 5% who aren't). If your sister is symptomatic - which she is - then that should be taken as showing that she is deficient. Just going by range with serum B12 is dangerous and even where results are in normal range the BNF recommends treatment on the basis of symptoms.
If her GP really wants to clarify if B12 deficiency is present rather than acting on the markers that have already been presented - then they could test for MMA which will be raised if cells don't have enough B12 - it can be raised by other things (kidney function mainly) but isn't raised by folate deficiency (unlike homocysteine)
on MTHFR - depend on exactly which variant you have and whether it is hetero or homozygous - affects processing of folate much more than B12 - even if homoxygous (2 copies), so not really surprising that it isn't really affecting B12 for you
Content on HealthUnlocked does not replace the relationship between you and doctors or other healthcare professionals nor the advice you receive from them.
Never delay seeking advice or dialling emergency services because of something that you have read on HealthUnlocked.