Hello all. Would be so grateful for some pointers on what to do - I am at a loss.
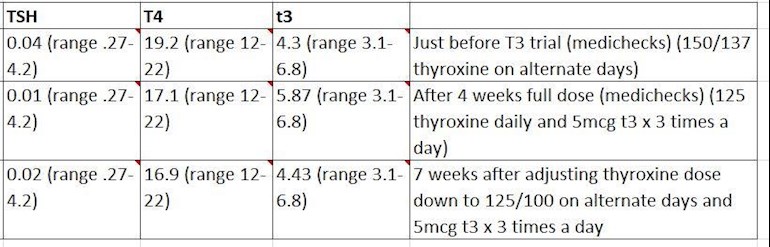
I have hashimotos hypothyroidism for 12 years. In a nutshell, I've paid to see a private endo recommended here as I was struggling with fatigue and he agreed to try me on a trial of T3 alongside (a reduced amount of) Thyroxine. Mid trial, my TSH was undetectable so my endo asked me to reduce my thyroxine further. A couple of weeks after I did this, I feel like I have crashed with all the signs that I associate with being undermedicated (as I have been in the past) - my resting heart rate has dropped, I am unable to exercise, my lower back is aching and despite sleeping well I wake up feeling exhausted and foggy. BUT my TSH is still too supressed. Looking at my numbers (pls see pic) the actual amount of thyroxine is lower than it was before the trial started and the T3 is pretty much unchanged. But the consultant said last time that TSH should not be undetectable as it can cause long term issues (what are these? Bone thinning?!).
I really don't know what to do next. I am fully expecting when I let the consultant know my most recent test results he will want to reduce medication further because of the very low TSH. But I already feel awful and dread to think how bad things could get if i take even less. Any advice so gratefully received! perhaps t3 just isn't the right fit for me?
I take iron spatone 2-3 times a week and high dose vitamin D daily as previous tests have shown me within normal range but the lower half for both. I have had coeliac tests which was negative.
I should also add that I started HRT (oestrogen patches and progesterone) about 2 months ago - which I'm know was probably not the most sensible move in the midst of a T3 trial but worsening migraines caused by perimenopause drove me to it!
Thanks in advance for any help!
R
Written by
Thyroidrunner
To view profiles and participate in discussions please or .
Was your TSH below range on T4 only? If you take T3, your TSH will be low or even suppressed, and lowering levo will not change that. Some people take T3 only (so no levo at all) and have a suppressed TSH. T3 tends to suppress the TSH more than levo.
If you feel bad, that could be because you are now taking too little T4 for your needs.
Everyone is different. After experimenting for +20 years (I also have Hashi´s), I realised that, even if I ended up needing T3, I also need T4 at a certain level. If my FT4 levels are below a certain level, adding T3 will not make me feel better. You may be one of those people who also need a certain amount of T4 to feel optimal. It can take a lot of tweaking to find YOUR sweet spot. Let your symptoms guide you, not your doctor!
Quite honestly, I wouldn´t trust a doctor who tells you to take less levo simply because your TSH is low, as long as your free Ts are in range.
Oral estrogen can be problematic as it raises thyroid binding globulin (TBG) levels which results in less thyroid hormone being available to the body. Transdermal estrogen (patches, gels, sprays) does not cause TBG levels to rise. So, the HRT should not be a problem in your case.
I couldn't agree with you more. Your saying exactly what I say and feel too. I need a certain amount of T4 to be able to sleep think and concentrate well with additional T3. I'm glad that I'm not alone that feels the same as yourself.
You most definitely are not alone! But T4 is sometimes forgotten because T3 gets so much attention…but I need both at a certain level, and if T4 levels drop too low, taking more T3 won’t make me feel better.
Yes!Yes!Yes! In fact adding more T3 to my low T4 for me personally makes me lethargic irritated and start having muscle/ joint pains. Makes it hard to climb stairs.
Thanks SlowDragon. I take thyroxine and T3 at 6am on empty stomach, then T3 mid morning and mid afternoon. I will get my levels checked. I am not on a gluten free diet - is there evidence to suggest this works for us? Thanks for your reply x
You don’t need any obvious gut issues to still find gluten free diet is beneficial
Hashimoto's frequently affects the gut and leads to low stomach acid and then low vitamin levels
Low vitamin levels affect Thyroid hormone working
Poor gut function with Hashimoto’s can lead leaky gut (literally holes in gut wall) this can cause food intolerances. Most common by far is gluten. Dairy is second most common.
According to Izabella Wentz the Thyroid Pharmacist approx 5% with Hashimoto's are coeliac, but a further 80% find gluten free diet helps, sometimes significantly. Either due to direct gluten intolerance (no test available) or due to leaky gut and gluten causing molecular mimicry (see Amy Myers link)
Changing to a strictly gluten free diet may help reduce symptoms, help gut heal
Before considering trial on gluten free diet get coeliac blood test done FIRST just to rule it out
If you test positive for coeliac, will need to remain on gluten rich diet until endoscopy (officially 6 weeks wait)
If result is negative can consider trialing strictly gluten free diet for 3-6 months. Likely to see benefits. Can take many months for brain fog to lift.
If no obvious improvement, reintroduce gluten see if symptoms get worse.
The predominance of Hashimoto thyroiditis represents an interesting finding, since it has been indirectly confirmed by an Italian study, showing that autoimmune thyroid disease is a risk factor for the evolution towards NCGS in a group of patients with minimal duodenal inflammation. On these bases, an autoimmune stigma in NCGS is strongly supported
In summary, whereas it is not yet clear whether a gluten free diet can prevent autoimmune diseases, it is worth mentioning that HT patients with or without CD benefit from a diet low in gluten as far as the progression and the potential disease complications are concerned
Despite the fact that 5-10% of patients have Celiac disease, in my experience and in the experience of many other physicians, at least 80% + of patients with Hashimoto's who go gluten-free notice a reduction in their symptoms almost immediately.
the times you take your T3 are exactly the same as the times I take mine. It seems to work for me. One addition. If you are taking T4 that is best taken right before you go to sleep for the night and and hour or two after you had dinner. I switched to that dosing time for T4 and found an improvement in my lived exerience.
Thanks again SlowDragon. I will try 112 daily that's a good idea. My brand of thyroxine is always changing unfortunately. Is their a brand I should be asking for? Thanks for your help x
Many people find Levothyroxine brands are not interchangeable.
Many patients do NOT get on well with Teva brand of Levothyroxine.
Teva contains mannitol as a filler, which seems to be possible cause of problems. Teva is the only brand that makes 75mcg tablet. So if avoiding Teva for 75mcg dose ask for 25mcg to add to 50mcg or just extra 50mcg tablets to cut in half
But for some people (usually if lactose intolerant, Teva is by far the best option)
Teva, or Aristo (100mcg only) are the only lactose free tablets
Most easily available (and often most easily tolerated) are Mercury Pharma or Accord
Mercury Pharma make 25mcg, 50mcg and 100mcg tablets
Accord only make 50mcg and 100mcg tablets
Accord is also boxed as Almus via Boots, and Northstar 50mcg and 100mcg via Lloyds ....but Accord doesn’t make 25mcg tablets
If a patient reports persistent symptoms when switching between different levothyroxine tablet formulations, consider consistently prescribing a specific product known to be well tolerated by the patient. If symptoms or poor control of thyroid function persist (despite adhering to a specific product), consider prescribing levothyroxine in an oral solution formulation.
Physicians should: 1) alert patients that preparations may be switched at the pharmacy; 2) encourage patients to ask to remain on the same preparation at every pharmacy refill; and 3) make sure patients understand the need to have their TSH retested and the potential for dosing readjusted every time their LT4 preparation is switched (18).
Levothyroxine is an extremely fussy hormone and should always be taken on an empty stomach and then nothing apart from water for at least an hour after
Many people take Levothyroxine soon after waking, but it may be more convenient and perhaps more effective taken at bedtime
No other medication or supplements at same as Levothyroxine, leave at least 2 hour gap.
Some like iron, calcium, magnesium, HRT, omeprazole or vitamin D should be four hours away
(Time gap doesn't apply to Vitamin D mouth spray)
If you normally take levothyroxine at bedtime/in night ...adjust timings as follows prior to blood test
If testing Monday morning, delay Saturday evening dose levothyroxine until Sunday morning. Delay Sunday evening dose levothyroxine until after blood test on Monday morning. Take Monday evening dose levothyroxine as per normal
REMEMBER.....very important....stop taking any supplements that contain biotin a week before ALL BLOOD TESTS as biotin can falsely affect test results - eg vitamin B complex
Could also be that your FT3 is too low for you. I see it's gone down since you reduced your levo, so that won't help, either.
An endo that prescribes T3 and doesn't know what the effects are going to be is an endo to avoid like the plague! He has no idea what he's doing, he doesn't understand how it all works.
There are no dangerous of suppressed TSH. That is a medicatl myth and is not born out by serious research. Once you're on thyroid hormone replacement, and the TSH is below 1, the TSH test is of little use. It cannot tell you if you're over-medicated, the FT3 does that. You are only over-medicated if your FT3 is over-range. There is no such thing as a 'too suppressed' TSH. And if your endo doesn't know that, he's never going to make you well.
TSH has two main roles, to stimulate the thyroid and stimulate deiodinase (T4 to T3 conversion). So, if TSH is too low your conversion is harmed, especially within tissues reliant on such conversion such as the brain and muscles. TSH has other lesser functions such as a role in bone formation. A suppressed TSH carries a risk of atrial fibrillation which can lead to stroke and possibly a smaller risk of osteoporosis. TSH usually reflects the combined effects of fT3 plus fT4 and so In healthy people is a good marker of thyroid status. It’s not sufficient that fT3 and fT4 are both within their reference intervals, what matters is where each is, the combined effect. If both are towards the lower end there will be hypothyroidism, if both are towards the upper end there will be thyrotoxicity.
Both T3 and T4 suppress TSH, liothyronine is about three times as potent as levothyroxine and so 10 mcg liothyronine will have the same effect on TSH as 30 mcg levothyroxine.
Looking at your history on the forum your TSH used to be OK but now seems to be very low on similar hormone levels. This suggests that your pituitary is now underperforming. This could be caused by a concurrent illness, depression or strict dieting amongst other things, or possibly a pituitary damaged by illness or an accident.
If you can’t find the reason for the low TSH I would be inclined to reduce your levothyroxine dose and possibly increase your liothyronine if you need to. This is because the low TSH will lead to low intracellular T3 even if serum T3 looks OK. Ideally you would get your TSH back up and be well on a moderate hormone dose like I believe you were a few years ago.
Try to avoid having a low TSH if you can as it leads to knock on consequences. You may not be able to do this.
Two comments. You state that a suppressed TSH carries a risk of atrial fibrillation. Please provide the evidence for that because, whilst my GP says the same thing, it is contrary to opinions expressed on the forum which refer to the work of Toft and researchers. Secondly you don't mention the genetic mutation in the DIO2 gene with its effect on the conversion of T4 to T3. I would be grateful for your response to these.
I usually refer to a 'low TSH' or 'very low TSH' because it is a factual description. I'm careful to only use the term 'suppressed TSH' when I believe TSH is driven low by high thyroid hormones. Sometimes TSH is low because the pituitary is under-performing, probably not damaged but not working as it should. I often use the term 'subnormal TSH' to describe this because the medical profession haven't come up with a term (I think they don't want to, they want to bury their heads in the sand). I think Thyroidrunner now falls into this category, their TSH is low because their pituitary is not producing as much TSH as we would expect.
There are lots of studies showing that a truely suppressed TSH leads to atrial fibrillation. This is my favourite one because it is well conducted and gives a balance view academic.oup.com/jcem/artic... . If you look at Table 2 you will see that the 'Adjusted HR' for 'Dysrhythmia admission/death' is 1.60. i.e. levothyroxine treated patients with a suppressed TSH are 60% more likely to be admitted to hospital or die from dysrhythmia. (You may need to scroll to the right of the table to see the adjusted column).
This study had an arbitary cut-off of 0.04 mU/L for defining a suppressed TSH. They would have got similar results if they used a higher or lower cut-off point. So, we mustn't take 0.04 as an exact figure, rather it gives an idea of where the risk lies. It's also worth noting that a mildly elevated TSH, so called 'subclinical hypothyrodism' carries higher risks than a suppressed TSH. I look forward to all our doctors warning us of the serious risk of suffering from subclinical hypothyroidism. Lastly, this study looks at cardiac events that lead to hospitalisation and death, other studies I have seen have shown higher AF risks for a suppressed TSH. My guess is this is because they include less serious events which are corrected by reducing the hormone dose or prescirbing beta blockers.
Fig. 1B shows how the risks of an abnormal TSH (high or low) builds up over time. Fig. 2
A is an excellent summary of the relation between log TSH and cardiac risk. Note there is quite a difference between a TSH of 0.04 and 0.01 - every little helps!
My point about AF is that a truely suppressed TSH does increase AF risk. A concern is that many patients are left hypothyroid for years and suffer cardiovascular damage as a consequence. My worry is that if these patients suffer AF they will be more likely to suffer a stroke because they will have weaker blood vessels due to prior long standing hypothyroidism. I feel it is wrong to give the impression that a suppressed TSH is safe and wrong to over-estimate the risk, especially in view of the greater risk from a mildly elevated TSH.
As for Toft, he was President of the British Thyroid Association (BTA) when they carried out a brutal witch hunt against doctors who diagnosed patients on the basis of clinical assessment or if they prescribed liothyronine. In his recent 'counterblast to guidelines' letter he states "We can prescribe doses of LT4 which do result in TSH suppression, but are associated with unequivocally normal serum T3 concentrations as I am unaware that
this combination of results has ever been proved a risk factor for atrial fibrillation or reduced bone mineral density". This smacks of pseudo-science as he offers no evidence for this hypothesis. The paper I cited shows that a suppressed TSH is associated with AF and fractures. I know of no study that looks at levothyroxine TSH suppressive therapy whilst separating out those with an fT3 above its upper limit. I feel that the majority of patients in these studies will have had an fT3 within its reference interval - few doctors will prescribe levothyroxine doses that elevated fT3 (and fT4 of course). Toft tends to lay down the law, regardless of evidence.
People with the rs225014 (Thr92Ala) DIO2 polymorphism have reduced type-2 diodinase activity. Studies have found this reduces their fT3 by about 0.4 and if they inherit the polymorphism from both parents they do not perform quite so well on cognitive studies if they are on levothyroxine monotherapy. They respond better to a little liothyronine. My view is that this polymorphism isn't very important, it explains minor symptoms which resolve with just a little T3. Many patients have severe symptoms and need lots of T3 - so their underlying problem is not the polymorphism. The DIO2 polymorphism is useful because it allows some doctors to rationlise prescribing liothyronine, often at doses greater than needed to overcome the effects of the polymorphism. It helps some patients get T3 and keeps it on the agenda. From a science point of view I don't think it is important.
Hi jimh111, so if a subnormal TSH is different from a low or very low one, I have a question, myTSH which is atm 0,0.31, would it be considered as subnormal or very low? I ask because as I have osteoporosis, but not because of TSH, as in my case it has always been over 0.5 and at periods of time over 2, I am interested in knowing if my risk of worsening my bones is increasing or not.
We are in danger of drifting too far off the original post. I wouldn't make much distinction between a low, very low or subnormal TSH. I just use the term subnormal to refer to a TSH that is low when it should be high because fT3 and fT4 (both) are below average.
It seems that osteoporosis is related to high thyroid hormones causing bone loss. TSH is easy to use as a indicator of overall thyroid hormone level (fT3 & fT4), that's why it is used in studies. So, if your TSH is low but fT3 and fT4 are around average I suspect it won't affect your bones. (I'm a patient not a doctor).
TSH does have a direct effect on bones but it seems to be minor. I draw this conclusion because bone loss seems to correlate more with fT3 or fT4 than TSH.
Some patients have to have a low TSH to recover. My guess is that if this enables them to lead a normal life and do exercise it will be better than having excellent blood tests and virtually disabled. I think it's more important to exercise within your limits than worry about the effect of TSH on bones.
yes now I¨m starting to recover from my hip problem as well and being able to walk some more distances so very soon I´ll be exercising my back much more. thank you very much, I was just reading your posts on the better conversion and activity of deiodinases if TSH wasnt abnormal thats why I wanted to know if I was included in the group hehe.
Hi, do you think HRT could be a contributing factor to a lower TSH? This might possibly be the reason why mine has always needed to be low for me to function. (Even when on T4 only my TSH was about 0.4 and my levels weren’t great). I don’t think there have been enough studies on this but I’m obviously very interested in any.Thank you for raising this point.
My numbers were all pretty similar to yours in all ways - I didn’t get my T3 up higher in range til I’d added in at least 20 mcg T3. But to get my T3 to move from 5.12 on Levo only to 6.3 on Levo plus lio, I had to take 30mcg a day. Getting my T3 that high has helped body temp, energy levels and hip pains.
I’d suggest you should never have lowered your Levo.
I was asked to reduce (from 100 to 50) and I felt awful as the T3 I’d added in didn’t compensate for that. So I unilaterally increased back to 100 along with the 20 lio. I’ve since added another 10 lio.
I don't think T3 is your problem, that lies with the prescriber whose knowledge is questionable
Consider how you felt during the mid trial....better?
I'd be inclined to try 100mcg levo plus 15mcg T3 (split if that suits you best) daily.... or even 20mcg T3
T4 to T3 conversion is poor (highish FT4 with low FT3)
So you may eventually need 20mcg T3
Wait 6 to 8 weeks then retest
Depending on both these results, and how you feel, review your dose if necessary.
Don't worry about TSH!
I have a form of thyroid hormone resistance and need high dose T3 to function, my TSH is on the floor but a heart scan shows my heart is fine as are my bones. I'm not dying!!
Show your medics the papers linked above,after highlighting the relevant points.....educate him!!
Before appointments I used to make a list of what I wanted to say ( as a reminder) and, as I've repeatedly said, it stopped me quacking like a demented duck with anxiety!!
Just a few thoughts... I'm not a medic just another patient who has had to learn how to improve my own health
I would focus on you FT3 levels my TSH is usually around 0 and I'm a poor converter from T4 to T3. I too have hashimotos since 1979 I stay mostly gluten & dairy free. I couldn't tolerated the meds and felt really bad last year when the endo changed my meds to levo and the T3 5 mcgs x 2 daily. I am back on NDT and feeling like myself again.
I think you’re feeling awful as you are over medicated. Your TSH being suppressed is letting you know you have too much thyroxine in your system. I would forget your third dose of T3 and keep with the same dose of Levothyroxine. If I’m over medicated my heart rate drops into the 40’s even 30’s and I feel as you are describing. This has happened a couple of times. Each time I reduced my medication I felt better. It may take 2/3 days on the lowered amount to feel start to feel the benefits.
I have taken T3 3 times a day when I was exercising at a gym 4 times a week. I had to reduce to 2 doses when I stopped. It’s an energy drug and you need to use it up or drop your dose. I presume you are on ThyBon Henning? Which is pretty powerful. Over medication symptoms can be very similar to under medication feelings for sure.
Your blood results don’t look alarming at all for T4 or T3 but I guess this test was before you took your daily medications? If so, once you take it you’ll go over the levels if your your TSH is suppressed like yours is.
I’d reduce your T3 by one dose. Make it the evening dose.
TSH is an indicator as to how much thyroxine is in your system. If suppressed you are carrying too much thyroxine is really simple as that. My TSH is not suppressed. Out of 18 blood tests while on T3 medication, only twice has it gone slightly suppressed. Both times it went suppressed I feel awful. A healthy persons TSH is about 1.00. This is what we should all be aiming for. To feel healthy. Calm but energetic. My latest TSH was 0.64(0.35-5.50) this is where I feel my best. I have regular 3 monthly tests. I’m going this morning for a regular blood draw. TSH, T4 and T3. Cortisol. B12. VitD. Folate. Ferritin. Lipids. Weight check. I get it done every 3 months as they are doing my regular B12 injection at same time. I keep a close eye on my bloods and want to keep my TSH low normal as this is a healthy persons thyroid level about around 1.00. Not everyone has to be suppressed TSH whilst on T3. It’s about managing your intake versus your energy output.
Your TSH being suppressed is letting you know you have too much thyroxine in your system. I would forget your third dose of T3 and keep with the same dose of Levothyroxine.
First of all, how can she have too much thyroxine in her body if her FT4 levels are in range? Are you saying that you should not look at the free Ts, only the TSH, to decide if someone is on the right dose of thyroid hormone?
Secondly, if she really does have too much thyroxine in her system, why not lower her dose of levothyroxine? Some experience a drop in FT4 levels when T3 is added. But if her levels of thyroxine are too high, that would be a good thing, wouldn´t it, so why lower T3 then?!
So, I find it really difficult to make sense of what you are saying.
What I am saying to be clear as said in my reply is, if she had her blood test prior to taking the medication it would be much lower than if she had the blood test after taking the medications. That is the big difference. Once you take your medications both T4 and T3 will increase significantly and in her case must be as her TSH is suppressed. So either T4 or T3 is too high. Her symptoms sound like she’s over medicated also. She needs a blood test after taking medications to check which of the two T4 or T3 is too high really. Maybe both are or maybe just one is. If your TSH is suppressed you are on too much thyroxine. A healthy persons TSH won’t be suppressed around 1.00 and that is what we are all striving to be ‘healthy’. Best thing is to manage your doses in order to keep all ranges good. Not over medicated.
I fear it would be no use arguing with you. All I can say is that you are wrong, on several accounts, and I hope that the OP won’t follow your advice. And, that others with more patience than me will chime in.
Well I have never felt so well with keeping my TSH just within range along with my T4 and T3 levels. I wonder how many people on here can say that. Being TSH suppressed due to over medication can cause people negative symptoms. I am not wrong.
I think it's important to consider your own past history of TSH levels on various levels of thyroid hormone when looking at other TSH levels . in your case McPammy, you often had TSH fairly high on 75mcg Levo with T4 top of range. ( TSH about 3/4 ish) , then when 10mcg T3 was added and you felt better , your TSH lowered , but was still just within range. (TSH 0.4 /0.6 ish )
So IN YOUR CASE it does make sense that TSH much lower than range may indicate too much thyroid hormone replacement FOR YOU.
However, lets take an example of someone else who for example has TSH 0.5 / 1 ish on 75mcg levo with T4 top of range . Then add in 10 mcg T3 , and like you ,they feel much better.... But now THEIR TSH will almost certainly go much further below range than your does .
I think that your particular relationship of TSH relative T4 /3 levels is individual to you ,, and also that you may in fact be in a minority.
It seem to me from my own results, and from the majority of results that i see here , it is somewhat unusual to be able have TSH at 'in range' levels while taking T3 in any form .
I think this may explain why you have formed the opinion that TSH 1 ish is desirable for all, even those on replacement thyroid hormone, because it just happens to be that your own personal setpoint for TSH relative to T4/3 levels that make you feel well is 'TSH just within range '
But i also see that it doesn't work that way for a lot of people ...lots of people do find that the right T4/3 levels for them to feel well cause their TSH to go under range.
Basically i'm trying to say in the kindest way possible ... i think you just happen to be lucky that your personal setpoint for 'TSH where you feel well' happens to be largely in line with the lab range.
But for somebody else, who produces less TSH than you at the level of T4/3 they feel best on .... their 'below range TSH' would not be an indication that they were on too much thyroid hormone. and "TSH 1" for them might mean 'way undermedicated '... especially if they were taking T3
" A healthy persons TSH won’t be suppressed ..... around 1.00 and that is what we are all striving to be ‘healthy’. Best thing is to manage your doses in order to keep all ranges good. "
The key word there is a "healthy" person. We know that once we take levo , this relationship between 'TSH around 1' and T4/3 levels usually changes .... you get relatively lower TSH for relatively higher T4 levels accompanied by lower T3 levels than in healthy/ unmedicated people .
If you then add taking T3 into the mix , you usually get TSH lower still. because taking T3 is usually observed to have a disproportionatly large effect on lowering TSH, compared to using Levo alone.
Yes I am going by my own personal experiences. My partner and my younger sister whom both have no thyroid issues both have a TSH around 1.00. They both check theirs through the NHS every year. It’s always around 1.00 and now mine is after getting to 36. And years of being undereducated with just T4 Levothyroxine at around 4. I’m 100% better than I was. I do know that when I went over medicated I had the same same symptoms as the lady posing the question. That’s why I replied in the way I have down to my own experience and symptoms.
yes i see that's how it is for you. and of course that it useful for you to know your set point's where you feel well.But for many others they might well have eg . a TSH of 0.4 even when just as undermedicated on Levo as you were ... we see it all the time on here. , and we see people all the time who only add a very small amount of T3 and no amount of loweering T4 will bring their TSH back into range ..... and those people will inevitably have to deal with their TSH being lower than range in order to try adding any T3 like you did.
My point is that experience shows us your TSH is actually unusually high for someone taking T3 , but that is not surprising, because it was unusually high on Levo before you did take T3.
This means you conveniently fit the into status quo view of many endocrinologists , but doesn't prove the staus qou view is correct for others who don't fit .
I do agree that we should always be open to the idea to try lower doses, with higher TSH, and give them a proper try for several months . I agree, some people might be surprised that they actually feel better that way.
I agree that overmedication symptoms can easily be mistaken for undermedication, and vice versa.
But for a lot of people ,their TSH just refuses to fit in that convenient box without them feel worse.
Taking exogenous thyroid hormones causes an observable disjoint between TSH levels and T4/3 levels. (this has been proved by several papers ~see Diogenes research)
So the fact that healthy people (who don't take T4 or T3) commonly have TSH around 1 becomes sort of irrelevant once they are on T4 or T3.
Is your TSH 1 now ?
If not , would you still feel well if your dose was adjusted to get it to be 1 ?
My TSH on my last blood test was 0.64(0.35-5.50) in Nov last year. Just within range. My T4 and T3 was mid way through ranges. I did the test leaving my medications for several hours as suggested on here. I’ve had 18 blood tests since I started T3. All bar 2 have been in range. 2 where over range which was T3. This is when I was taking T3 3 times a day when I was well enough to go the gym. I had to reduce to twice a day. Then I felt much better.
So well said, Tattyboogle!👏👏 I could not agree with you more...it´s been said here a thousand times, but it´s worth repeating: we can only offer advice and tell others what worked for us, but we cannot tell them that just because something helped us they will never get better unless they do the same thing. It simply does not work that way with thyroid hormone replacement. And I don´t think that we should try to replicate what happens in healthy people. They don´t get all their thyroid hormone from a pill, but slowly secreted from their thyroid gland day and night. There is simply no way we can mimic that once on thyroid hormone repacement.
Your TSH being suppressed is letting you know you have too much thyroxine in your system.
No, that's not what the TSH is letting you know. It's letting you know that the pituitary is satisfied with the amount of thyroxine - and T3, it doesn't distinguish between the two - in the system. But, that is because the pituitary is served first when it comes to dishing out thyroid hormones. And, it's quite common for the pituitary to be satisfied, but other tissues to still be hypo. There's no way we can tell how much thyroid hormone is getting into the cells, but if we look at how much there is in the blood - hence the FreeT4/3 tests - we can tell how much it possible to get into the cells. And, in this case, it's not a lot. The FT4 isn't even top of the range.
TSH should not be used for dosing. That is the best way to keep the patient sick, as evidenced by the number of sick people we have on here whose doctors only test TSH. The important number is the FT3, and that is well within range.
I’m not saying the TSH is best way to dose. I am saying T4 and T3 levels shouldn’t be over medicated. TSH only goes suppressed when you have too much medication. ‘Pituitary being satisfied’ would mean TSH is in range along with T4 and T3 being in range. It’s satisfied.. suppressed means not satisfied if you want to word it like that. But it ends up being the same thing. Suppressed means over medicated. I do know the differences and feel the difference between suppressed and not. I have experience both. The lady who posted her question is not feeling well on her suppressed TSH. I suggested she is over medicated as her TSH indicates that.
TSH only goes suppressed when you have too much medication.
No, not so. When you have too much 'medication', it shows in your FT4/3 readings, not the TSH. That is totally wrong.
I do know the differences and feel the difference between suppressed and not.
But, the TSH itself doesn't make you feel anything. It does not cause symptoms.
The lady who posted her question is not feeling well on her suppressed TSH.
The OP is not feeling well because her FT3 has dropped and is now too low for her - she's back to where she was before starting T3, when she also felt unwell. Nothing to do with the TSH itself.
I completely disagree with you I’m sorry to say.I think you are misunderstanding what I’m saying here. If her T4 or T3 is too high from ingesting too much thyroxine in turn her TSH will go suppressed. A healthy persons TSH will be around 1.00. This is what we aim for… to be healthy.
I think you are saying it doesn’t matter about a suppressed TSH? Of course it does as it’s reflecting that your T3 or T4 levels are too high, one or both.
If you do not take your medication prior to a blood test your T4 and/or T3 will be much lower than if you had. We all know that.
A healthy persons TSH will be around 1.00. This is what we aim for… to be healthy.
We aim to be healthy, yes, of course we do. But, there is no guarantee that keeping the TSH the same as that of a 'healthy' (euthyroid) person, will make a hypo healthy. Our bodies no-longer work the same. The HPT axis has been broken and is no-longer reliable. What we have to do is find what makes us healthy as individuals, not as a standard euthyroid model. If you are fit and healthy with a TSH of one, and the Frees in the right place for you, then you are very lucky. That is not the case for everybody. You should not try and force everybody into the same mould - that is the mistake the majority of doctors make, and why so many hypos are still ill depsite euthyroid levels. I think you should read some of diogenes ' posts, because they explain it all very well.
I think you are saying it doesn’t matter about a suppressed TSH? Of course it does as it’s reflecting that your T3 or T4 levels are too high, one or both.
Yes I am. And no it doesn't. A suppressed TSH does matter in as far as conversion is concerned, but it is not a realiable guide to dosing. Far too many variables for that.
If you do not take your medication prior to a blood test your T4 and/or T3 will be much lower than if you had. We all know that.
Of course it will! That's exactly why we leave a 24 hour gap for levo and 8 to 12 hours for T3. It is a very short-lived peak in levels, and gives no guide to our normal circulating levels of thyroid hormone in the blood. And that's what we want to know in testing: how much we have for the majority of the day, not what we have during the brief peak two hours after dosing. But that has nothing to do with the TSH. I think you're getting a bit muddled here.
I’m not muddled, my mind has not been so clear in years. All I know is that I’ve never been so energetic and healthy in years after years of under medication. I can only go on my own experiences and blood results. I’m much better within range on all 3 counts. I’m just passing on my experiences and definitely not forcing everyone into a mould. It’s where I have got my life back and like I’ve said never felt so good. I feel like I’m in my 30’s not 60’s. And my friends and family are truly amazed at my turnaround. I just wanted to help this lady if I could. I’m very upset at what I now feel ganged up on by members on here today.
Ive done nothing but try to help people on here to get well as I managed to.
I’ve lost over 4st. My thyroid levels are all in range. My B12, vitD, folate, ferritin, cortisol and lipids are all optimal now my thyroid is working as it should along with B12 and ferritin supplements. And I have loads of energy that I lacked for years. So I guess I am extremely lucky from being unable to walk and losing my job at Rolls-Royce to now being well again and enjoying life once again.
You are making bald statements. That is not sharing experience. You never say 'perhaps' or 'maybe', or 'this worked for me, could work for you'. You are stating bluntly that a suppressed TSH is always a sign of over-medication when it is blatently not. And, if you cannot accept that that is what you are doing, nor that what works for you won't automatically work for someone else, then there's nothing else I can say to you. I'm just warning people not to take this as a given. We are all different and have to find what works for as individuals.
Please don't take my /our points that way . We are just making the point that not everyone will have TSH at this level when they feel well, because that point is equally as true, and important to understand , as the fact that you DO feel really well with TSH in range .........no one is suggesting your dose of medication is wrong for you. or that you are wrong in you observations of yourself. and nobody thinks you are 'lucky' in that sense.. we all understand how devastating is to have lost things we value due to struggling to manage thyroid problems. Your observations and experience ARE very useful.
But in order to help people get well, we have to be prepared to see 'outside the box' of the rules of standard therapy.
if you had been only been advised to follow the 'rules' of standard thyroid therapy because they worked for most people ..... you wouldn't have been offered any T3, you'd probably still be on around 75mcg Levo with minor tweaks up ands down a bit here and there.
Your thyroid gland is not working as it should now...you have found the right dose of T3 and T4 for your needs, to replace the hormones you are no longer making on your own. There is a difference.
You are not being 'ganged up on' just because no-one agrees with you. We're just trying to help you see the other side of the question - tattybogle expresses this much better than I can. But, you're not seeing that there could be any other way of doing things other then the way you do them. It worked for you, and I'm very happy for you, glad you got your life back, and no-one is saying that that is not true. But, it wouldn't work for everyone, and that's what everyone is trying to explain to you, but I don't think you even read these explanations, you are so sure that you are right. I know you want to help people - we all do, that's why we're here - but I'm afraid you're not going the right way about it.
It’s an energy drug and you need to use it up or drop your dose.
It's statements like this that make me think you are muddled. For a start, T3 is NOT a drug, it is a hormone. Not the same thing. Yes, it does give you energy, but no, you don't need to 'use it up'. It only gets used when it gets into the cells, and not everyone gets it into the cells very well. Once it's in the cells, it stays there for about three days, whether it's 'used up' or not. It will then be converted to T2 as part of the recycling process. Dropping your dose will reduce the amount in the blood, and some people need high levels in the blood to get any into the cells. What is in the blood will only have a half-life of about 24 hours, so no need - and no way of - 'using it up'. You are giving people a completely false idea of how all this works, mainly, I think, because you don't understand it very well yourself. It's complicated, I know - lord knows I don't understand the half of it! - but you're confusing people and putting them off experimenting for themselves - the way you did - to find the right dose and the right hormone for them.
Wery nicely summarised! You and tattybogle have done a great job explaining how the body works and how hormones work together, not in isolation. I also agree that telling someone she is wrong does not amount to "ganging up". I have always been impressed with how nice people here are to each other...not all forums are like that.
I have left this thread due to feeling upset by all 3 people putting my experiences down. It goes both ways. You are not always right nor am I. We are all different. You once told me in my early days on T3 to double my T3 dose as you said 5mcg was way too small a dose. After a few days of that increase I actually went way over medicated and ended up in A&E as I could barely walk. That’s why I trust in my own decisions now. I never told you this at the time. I just let it go. And put it down to experience. That A&E visit was one of the two occasions that I’ve been over medicated on T3. The 2nd time was when I stopped going the gym when covid arrived. I had to return to twice a day dosage as I wasn’t burning off my energy as much.
We are all different with different amounts required to get optimal. I’m now optimal and strive to remain so. I hope you are well and your levels are optimal for yourself also.
This string of responses has caused me to be quite upset. I only ever want to help people and offer my experiences to help them get optimal and well.
I feel I’ve been bombarded with many messages putting my thoughts and experiences down. Not everyone has a suppressed TSH on T3. I’m living proof of that. I won’t reply to any messages again in this thread I’m sorry to say.
What we are saying is that you are wrong to say that:
* suppressed TSH automaticalling means that you are over-medicated - it doesn't
* T3 is an 'energy drug' - it isn't
* you should take your thyroid hormone just before the blood draw - you shouldn't
Those three points go against the majority opinion on this forum, not just three people. It's just three people that have tried to explain to you why those three point are wrong. And none of us are saying that we're always right about everything but we are right about those three points we've picked up on.
I'm sorry if that upsets you - and I'm sorry if I gave you wrong advice in the past and 10 mcg T3 was too much for you - it wouldn't be for most people. But that's life. We live and we learn - or we should do.
And, if one goes through all your posts, as I did, right from the beginning, it would seem that there were quite a few occasions when you ended up in A&E, barely able to walk, that had nothing to do with high T3...
"I asked Prof W. He said increase T3 to third dose. And leave Levothyroxine as is at 75. But I went over medicated in 7 days. We reduced increase to 2.5 and I went over medicated in 14 days."
"I did increase my T3 with my Endos advise however I went over medicated after a week with 5mcg increase. So I reduced to 2.5mcg T3 increase but after 2 weeks I went over medicated again. So now I’m back to my normal dose of 5mcg twice daily. This gets me to the top of the blood level."
In this forum, we offer patient-to-patient advice, not medical advice. All we can do is tell others about our experiences and what worked and what didn´t work. If someone´s advice made you feel worse, you cannot blame the person who gave it to you with the best of intentions .To be honest, I am a bit disappointed that so few people have participated in this discussion, as I know many here take T3 with great success.
As tattybogle pointed out in one of her posts, you are fortunate to feel so good with both FTs in range and a normal TSH while taking T3. I guess I speak for everyone here when I say we would all like to be like that as that would mean we would not have to fight ignorant doctors. But, unfortunately, many of us have to "sacrifice" our TSH in order to get our free Ts, and especially our free T3, up where we need them. And, the fact that you were able to maintain a normal TSH while optimising your free Ts using T3 does not mean everyone would be able to do that. Judging from the thousands of posts here, you are the exception to the rule, and a very fortunate exception at that. And nobody is saying your opinion or experience are less valid than anyone else´s. However, disagreeing with someone does not equal ganging up on them - even if several members disagree with you.
I’d be interested to know exactly what your T3 t4 and tsh. It’s great you’re feeling well but this person isn’t with t4 and T3 not at all high in range.
I know you’ve had lots of replies, but hopefully to reassure you, I’ve been on a T4/T3 combination since 2010, and my TSH has been barely detectable. I am not aware of suffering any I’ll effects from that
Found this artcle on eostrogen and how it lowers thryoid medication efficacy. Useful for me too as I am in same position as this poster : webmd.com/women/news/200106...
I started HRT and my thyroid levels were affected but didn't click with GP it's to do with my HRT😑
It was someone on this forum who raised this with me and it got me to think. I am retesting thyroid function in Feb after increasing my Levo. Will see what bloods show.
Hi sorry about your condition. I experienced suppressed TSH when my go increased my levethyroxin without any blood test to 100. I had become over active by TSH 0.02 and T4 20. I went to private consultation in Alexander Hospital in Manchester. he increased the dose and my TSH came in normal range. However I fpund a polish clinic in Oldham that I found they are better. Yesterday for the second time i saw my polish consultant and when I asked for trial, he said my T3 in within normal range so no need to try other medicine , he saud it is goid for someone T3 is not manageable. I have pain in my knees which he said it us for levo.
Suggest you get full thyroid and vitamin testing done via Medichecks or Blue horizon
Come back with new post once you get results
Knee pain could be low vitamin D
Bloods should be retested 6-8 weeks after each dose change or brand change in levothyroxine
For full Thyroid evaluation you need TSH, FT4 and FT3 plus both TPO and TG thyroid antibodies tested.
Very important to test vitamin D, folate, ferritin and B12 at least once year minimum
Low vitamin levels are extremely common, especially with autoimmune thyroid disease (Hashimoto’s or Ord’s thyroiditis)
Autoimmune thyroid disease with goitre is Hashimoto’s
Autoimmune thyroid disease without goitre is Ord’s thyroiditis. Both are autoimmune and generally called Hashimoto’s.
In U.K. medics never call it Hashimoto’s, just autoimmune thyroid disease (and they usually ignore the autoimmune aspect)
About 90% of primary hypothyroidism is autoimmune thyroid disease
Recommended on here that all thyroid blood tests should ideally be done as early as possible in morning and before eating or drinking anything other than water and last dose levothyroxine 24 hours before test
This gives highest TSH, lowest FT4 and most consistent results. (Patient to patient tip)
Private tests are available as NHS currently rarely tests Ft3 or all relevant vitamins
From personal experience, changing Levo dose is a horrid thing whether up or down and dropping a dose by too much too soon (in total you've reduced Levo by 31mcg - from 143.5 to 112.5 ) when embarking on a T3 trial sets it up to fail. I'd suggest going back to 125mcg Levo with the 5mcg Lio 3x day and sticking on that for longer than 4 weeks and see how you feel. If good, you'll need to argue with the Endo what's really important - lab report or you?
I think your endo will not ask for you to reduce your meds further. He will undoubtedly be pleased the TSH has risen.My TSH has been 0.02 for a long time and there was no issue. It’s only since it’s dropped to 0.01 that my endo isn’t too happy. (Did a post on this last week and answers were very helpful). There seem to be too many “professionals” hung up on the low TSH. Once we are on T3, it seems some of us have really low TSH levels. Others not so.
I’ve said about getting a bone density test done. My endo requested it 4 years ago but my GP either missed it or ignored it.
I think I will be sticking to my guns. Because like you, I’d rather have a life now than be housebound and barely be able to do anything. Surely a sedentary life with depression would cause even more issues (plus my cholesterol would probably go up again)?
By the way, I’m on HRT patches too. But I did start mine well before my Hashimoto’s diagnosis.
Let’s hope we both get our levels sorted soon and our endos calm down about the low TSH. 🧁
Thank you to you all for taking the time to reply to me in such detail. I am reading through it all and taking notes! However I’m sorry for inadvertently creating a debate which has caused some upset x
That is not your fault! Sometimes, a certain issue is raised that causes debate and the original discussion gets sidetracked. But that has nothing to do with the original post(er)!
Content on HealthUnlocked does not replace the relationship between you and doctors or other healthcare professionals nor the advice you receive from them.
Never delay seeking advice or dialling emergency services because of something that you have read on HealthUnlocked.

")
