From reading other postings and advice from all you lovely people on here, I did Blue Horizon’s Thyroid+11 panel. I have hashi’s (diagnosed 2010), currently on 100mg Levo, 48 y.o female. I am feeling indescribably exhausted, achy, breathless and mild nausea on and off and have been for around 3-months. Thought it was stress of work, but this is getting unbearable now.
I would really appreciate your thoughts so that I can take these results to my GP (not that I have ever had the same one twice at my surgery!) and try and be assertive with him or her about what I think I need …
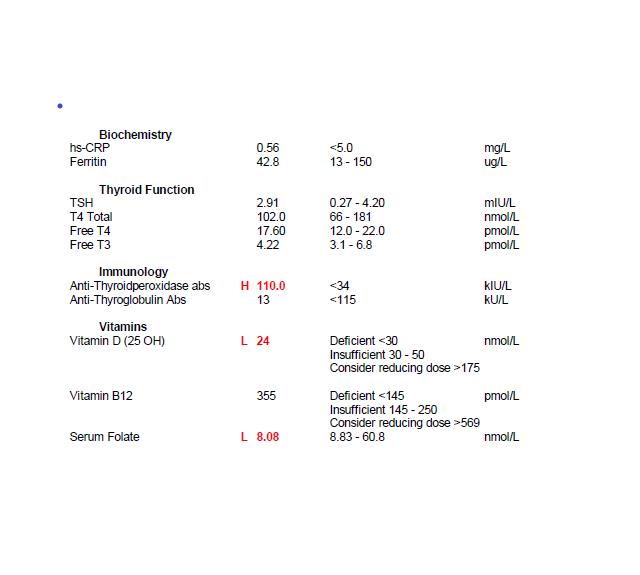
I can see that Vit D needs urgent attention and TSH not great at the moment, but T4 and T3 levels are ok, I think? TSH is up from from 1.1 in June (same range and same fasting morning bloodtest before taking levo).
But it is the folate that is confusing me – it is low, but ferritin only low-ish and B12 is ok. I can honestly say my diet is good. Of course it could be better, but I am almost a green vegetable and banana freak! And I have been following a GF diet since April 2017 – but have lapsed over past 2 months (but I am going back to it strictly from now on as it definitely made a difference ..)
Also, I don’t understand whether this result is showing active b12 or not and if anyone could explain the difference to me, I would appreciate it.
Any thoughts appreciated. Thanks so much.
Written by
jlanable
To view profiles and participate in discussions please or .
This B12 test is Serum B12, not Active B12. Serum B12 tests both active and inactive forms. I'm not an expert on B12 but from what I've read, Active B12 is about 10-30% of the total of all B12 and it's Active B12 that goes from the blood into the cells. Serum test may show "normal" but you could still actually be deficient.
Your result of 355pmol is the same as 481pg/ml. According to an extract from the book, "Could it be B12?" by Sally M. Pacholok:
"We believe that the 'normal' serum B12 threshold needs to be raised from 200 pg/ml to at least 450 pg/ml because deficiencies begin to appear in the cerebrospinal fluid below 550".
"For brain and nervous system health and prevention of disease in older adults, serum B12 levels should be maintained near or above 1000 pg/ml."
As your folate level is below range, you should discuss this with your GP and he should really prescribe folic acid. Recommended level for folate is at least half way through it's range (but yor doctor wont know this, they aren't taught nutrition).
Also point out to your GP that at a level of 24nmol/L you have Vit D Deficiency and according to NICE treatment summary for Vit D deficiency:
"Treat for Vitamin D deficiency if serum 25-hydroxyvitamin D (25[OH]D) levels are less than 30 nmol/L.
For the treatment of vitamin D deficiency, the recommended treatment is based on fixed loading doses of vitamin D (up to a total of about 300,000 international units [IU] given either as weekly or daily split doses, followed by lifelong maintenace treatment of about 800 IU a day. Higher doses of up to 2000IU a day, occasionally up to 4000 IU a day, may be used for certain groups of people, for example those with malabsorption disorders. Several treatment regims are available, including 50,000 IU once a week for 6 weeks (300,000 IU in total), 20,000 IU twice a week for 7 weeks (280,000 IU in total), or 4000 IU daily for 10 weeks (280,000 IU in total)."
Each Health Authority has their own guidelines but they will be very similar. Go and see your GP and ask that he treats you according to the local guidelines or this summary and prescribes the loading doses. Once these have been completed you will need a reduced amount (more than 800iu so post your new result at the time for members to suggest a dose) to bring your level up to what's recommended by the Vit D Council - which is 125nmol/L and the Vit D Society recommends 100-150nmol/L - and then you'll need a maintenance dose which may be 2000iu daily, maybe more or less, maybe less in summer than winter, it's trial and error so it's recommended to retest once or twice a year to keep within the recommended range. You can do this with a private fingerprick blood spot test with City Assays vitamindtest.org.uk/
There are important cofactors needed when taking D3 as recommended by the Vit D Council -
D3 aids absorption of calcium from food and K2-MK7 directs the calcium to bones and teeth where it is needed and away from arteries and soft tissues where it can be deposited and cause problems such as hardening of the arteries, kidney stones, etc.
D3 and K2 are fat soluble so should be taken with the fattiest meal of the day, D3 four hours away from thyroid meds.
Magnesium helps D3 to work. We need Magnesium so that the body utilises D3, it's required to convert Vit D into it's active form. So it's important we ensure we take magnesium when supplementing with D3.
Magnesium comes in different forms, check to see which would suit you best and as it's calming it's best taken in the evening, four hours away from thyroid meds
Check out the other cofactors too (some of which can be obtained from food).
Your ferritin also needs improving. For thyroid hormone to work (that's our own as well as replacement hormone) it's said that ferritin needs to be at least 70, preferably half way through range. You can help raise your level by eating liver regularly, maximum 200g per week due to it's high Vit A content, also liver pate, black pudding, and including lots of iron rich foods in your diet apjcn.nhri.org.tw/server/in...
It's very likely that your nutrient levels are this bad because your Hashis, confirmed by your raised TPO antibodies. Hashi's and gut/absorption problems tend to go hand in hand.
You will probably benefit from going back on your gluten free diet and supplementing with selenium l-selenomethionine 200mcg daily can also help reduce the antibodies, as can keeping TSH suppressed.
Some Hashi's information:
Gluten contains gliadin (a protein) which is thought to trigger autoimmune attacks so eliminating gluten can help reduce these attacks. You don't need to be gluten sensitive or have Coeliac disease for a gluten free diet to help.
SlowDragon is our Hashi's expert, have a look at one of her posts which gives information and links about gut problems here near the bottom of the thread
The aim of a treated hypo patient generally is for TSH to be 1 or below or wherever it needs to be for FT4 and FT3 to be in the upper part of their respective reference ranges when on Levo if that is where you feel well.
Your TSH is too high at 2.91, your FT4 is 56% through it's range and your FT3 is only 30% through it's range. You are undermedicated and need an immediate dose increase of 25mcg Levo, retest in 6 weeks, repeat increasing/retesting every 6 weeks until your levels are where they need to be for you to feel well.
You may find that as your nutient levels optimise then your thyroid hormone may work better.
Content on HealthUnlocked does not replace the relationship between you and doctors or other healthcare professionals nor the advice you receive from them.
Never delay seeking advice or dialling emergency services because of something that you have read on HealthUnlocked.