Melatonin is the only naturally occurring substance in the body that I have found that can help return the body toward homeostasis through multiple pathways.
Definition of homeostasis:
the tendency toward a relatively stable equilibrium between interdependent elements, especially as maintained by physiological processes.
This includes returning elevated inflammatory levels and elevated oxidative stress levels back toward normal/healthy. I have not found any other single molecule produced in the body that can potentially do that and much much more in terms of protecting the body and its organs. Here is a link where they used 100 mg/night in resistance trained athletes for 4 weeks and were able to return them to " redox equilibrium" with that dose. Here is a link to that study which is behind a paywall.
>>>We conclude that melatonin supplementation at doses of 100 mg.day-1 during four weeks, 30-60 min before bedtime, enhances the efficiency of the endogenous antioxidant defence system leading to redox equilibrium, and yields skeletal muscle protection against exercise-induced oxidative damage, without adverse effects (Zhang and Zhang 2014).>>Our findings confirm the beneficial effects of melatonin treatment on athletes, without any undesirable side effect that could affect athlete's performance.<<<
The study above showed the health benefits and safety of 100 mg / night in athletes. The following study shows the value of just 10 mg / night of melatonin in PWP :
It makes you wonder what that same 100 mg study would have shown in PWP.
Melatonin promotes stabilization of Nrf2 as well as increased gene and protein expression of Nrf2 while suppressing KEAP1. This is highly desirable as more activated Nrf2 will increase the antioxidant status to levels capable of greatly reducing oxidative stress which does much of the damage in PWP. Melatonin via activation of Nrf2, HO-1 and Sirt 1 is able to also reduce neuroinflammation.
In PWP it is known that the total antioxidant capacity(TAC) is significantly reduced and significantly below healthy controls. The bodies response to this is to produce more melatonin, to increase TAC, but the body does not seem to be able to produce enough melatonin on its own to complete this task. This is why studies of PWP show elevated serum melatonin levels, but not nearly high enough to return to homeostasis as glutathione and TAC are at reduced levels even though melatonin serum level is above normal control levels. Of course this problem is exacerbated with age as native melatonin levels decline fairly quickly from puberty to the 50's at which point they continue to decline at a lesser pace. Even so, just 10 mg of melatonin per night starts to increase glutathione and TAC, but not enough to reach redox equilibrium as was seen in the 10 mg PWP study. Keep in mind that although the exact cause of PD is not known, it is established that excess oxidative stress and excess inflammation are what is doing most if not all of the damage in PWP, so you can see the value of returning the body to redox equilibrium to slow or stop this destructive process.
In the following study, children with Duchenne Muscular dystrophy were given melatonin at 70 mg/day for 9 months and the effects were remarkable! There was a follow up report on these children the following year which was also remarkable and is the second link below!
Melatonin is the most potent antioxidant in the body for multiple reasons. Melatonin upregulates gene expression of the following natural antioxidants in the body, superoxide dismutase(SOD), catalase(CAT) glutathione(GSH), glutathione peroxidase (GPx) and heme oxygenase 1(HO-1). Each of these antioxidants have potent properties of their own. Take HO-1 as an example. By itself, it has the following qualities of antioxidant, antiinflammatory, anti apoptotic, antiproliferative and immunomodulatory effects, but the positive effects of melatonin go much further!
Melatonin itself is a potent scavenger of the following : reactive oxygen species (ROS)/hydroxyl radicals, reactive nitrogen species (RNS), H2O2 and peroxynitrite (ONOO). All of these are at elevated levels in PWP. Further, melatonin can neutralize up to 10 oxygen radicals compared to the antioxidants vitamin C and vitamin E, which can only neutralize oxygen radicals on a one to one basis. Melatonin works through multiple pathways, one of which is the Nrf2 / KEAP1 pathway which Albert has gone in to detail about. The following study describes how elevated levels of peroxynitrite
(almost 50% elevation) lead to elevated UPDRS score while melatonin is an effective scavenger of peroxynitrite, ROS, RNS and H2O2, either directly or indirectly.
Melatonin is also a protector of the mitochondria and in fact is produced in the mitochondria and melatonin is also absorbed by the mitochondria. This is important because PD is a mitochondrial function disruptor and the malfunctioning mitochondria can lead to dopaminergic neuron death as outlined in the abstract below. Keep in mind that the body is not able to produce enough melatonin on its own to prevent all of the damage to the mitochondria.More melatonin is found in the mitochondria than in the blood by a very significant amount. Melatonin has already proven to restore mitochondria function in Alzheimer's mice.
The following full study highlights some of the abilities and usefulness of melatonin in PD including melatonin's ability to reduce alpha synuclein aggregation to protect dopaminergic neurons from death, protect mitochondria also to protect dopaminergic neurons from death, antiinflammatory properties to control inflammatory damage in the brain, scavenge multiple radical types to protect the brain as a whole and protect dopaminergic neurons specifically, points out that PD impairs brain melatonin production as well as decreases melatonin receptors in the substantia nigra.
You're probably wondering how melatonin can do so much in these studies above, but this is nothing compared to what melatonin is doing in the rest of the body! All of the above concerning melatonin is barely a snippet of what melatonin is capable of in the human body! The following August 2020 full study goes into significant detail concerning the broad spectrum beneficial health effects of melatonin in humans and animals.
Keep in mind that the melatonin health benefits highlighted in the above study is not a complete list!
Dr. Neel, Dr. Reiter and Dr. Shallenberger (74 years old) all use melatonin at 100 mg /day or higher for extended periods of time. Dr. Neel uses it in his Covid-19 patients very successfully at 1 mg per kilogram! Dr. Russell J. Reiter is a world renowned melatonin researcher who has been involved in over 600 studies and uses it in his animal studies and himself @ 100 mg+/night for 25 years as a preventative and he is in his 80's. Dr. Shallenberger uses it in all of his patients and himself @ 180 mg / night and up to 360 mg/ day in some of his stage 4 cancer patients. Some researchers are considering over 500 mg/day of melatonin for Covid-19.
In PWP, there is increased potential for heart problems and melatonin is heart protective as well as protective of the major organs, including the brain and vasculature.
The following is only a rat study, but it shows that melatonin protects dopaminergic neurons from death. Keeping in mind that melatonin easily crosses the blood brain barrier and enters all tissues of the body including the substantia nigra in the brain to impose its highly potent antioxidant and multiple radical scavenging activities, it is like another piece of the puzzle being put in place. We already know that 10 mg of melatonin per night confers positive and measurable health benefits in PWP in just 12 weeks with a very good safety profile. The melatonin receptors are there in the substantia nigra pars compacta for a reason. Now we just have to find out what higher dosing and longer duration can do for PWP.
Another animal study shows that melatonin at high dose, protected against nigral dopamine loss and replenished the striatal dopamine loss that resulted in amelioration of rotational behavioral bias in Hcy denervated animals.Melatonin administration significantly improved mitochondrial complex-I activity and protected the SN neurons from the toxic insults of oxidative stress induced by Hcy. Amelioration of oxidative stress by melatonin in Hcy-infused SN was bought by dose-dependently scavenging of hydroxyl radicals, restoration of glutathione level and elevation in the activity of antioxidant enzymes.
There is still more research to be done, but the past and current studies have peeled back many of the layers of melatonin and continues to show what a remarkable and useful molecule it is for human health and PWP. At this point further studies using high dose melatonin in PWPs are warranted and desperately needed to determine the most effective dose.
The following abstract shows that a 100 mg intravenous dose of melatonin in humans was very well tolerated with no adverse effects or sedation :
It took a bit of time, but I have gathered the information regarding the safety or lack of safety of high dose melatonin in the 12 links below. As much as possible I tried to use scientific human studies as opposed to animal studies or test tube studies. The last link lists side effects of melatonin and side effects of Sinemet to give some type of comparison to a known quantity such as Sinemet which is considered as a common and often times frontline treatment for PD. Keep in mind that at the doses used in these studies that we are no longer looking at melatonin as an over the counter sleep aid, but rather as an effective treatment for some fairly serious diseases.
1. The following abstract briefly discusses what is currently known about the safety of melatonin in humans and is in line with the above information :
2. In the following ALS human and mouse study, the mice and humans were given melatonin at 300 mg/day for up to 2 years to very good effect. They also used suppository melatonin for the humans with no next day sleepiness suggesting that the suppository approach may be a way forward for people who report excess next day drowsiness!
3. Melatonin studies using up to 1,000 mg/day in cancer patients have been done with no side effects.
4. This RCT human study gave a one time dose of 50 mg per kilogram of body weight. To put that into context, if you weigh 150 lbs or 68 kg, your dose would be getting 3,400 mg of melatonin!.If you weigh 80 kg, the dose of melatonin would be 4,000 mg! Yes, nobody has ever died or been seriously injured by melatonin.
5. In this study, a 100 mg intravenous bolus of melatonin was given to humans. This study is important because oral dosing only delivers as low as 3% to 15% of the melatonin into the system. So a 100 mg bolus is equivalent to a much much higher oral dose. Other important points to this study are no side effects and no next day sedation effects. Important for people who feel groggy the day after taking melatonin (melatonin hangover).
7. This lengthy new study for treating Covid-19 based on previous studies is suggesting a dose of 8 mg per kilogram or 8 times the dose that Dr. Neel is effectively using for his Covid-19 patients! This a good study and although lengthy, it is interesting reading. Here are a couple of interesting quotes from it :
Nordlund & Lerner (26) treated patients with 1,000 mg melatonin/daily for 3 months and they did not find obvious side effects in these subjects.
Voordouw et al. (27), testing melatonin as a contraceptive medicine, treated 12 women with 300 mg melatonin/daily for 4 months and no significant side effects were reported.
Weishaupt et al. (28) gave to severely ill ALS patients 300 mg melatonin daily for 2 years, without any adverse effects.
For the acute melatonin treatment, the dose can be as high as 50 mg/kg for surgical patients, who tolerated this extremely high melatonin dose well and without serious side effects (29).
All data indicate that large doses of melatonin, whether given chronically or for acute treatment will not cause intolerable or uncontrollable side effects and that the safety margin of melatonin for humans can be up to 3,750 mg/day for a 75kg individual (29).
9. This is an interesting article that discusses high dosing of melatonin in some major diseases including PD. They are suggesting dosing in the 25 ~ 100 mg range. Here is a quote from the article :
>>>Degeneration of the dopaminergic neurons is caused finally by increased oxidative stress and inflammation. Treatment with melatonin at doses between 25 mg and 100 mg are able to significantly reduce oxidative stress in the substantia nigra thus blocking neuron death. This treatment needs to be started at the initial steps of the disease since it is not able to reverse the already degenerated neurons. The combined treatment with L-dopa and melatonin reduces the doses needed of the dopamine agonist and blocks the evolution of the disease, by preventing the oxidative stress induced neuron death. The disease remains stable and does not continue its evolution.<<<
11. The following study used 250 mg / day of melatonin for 8 weeks in T2DM patients and in those 8 weeks significantly lowered markers of inflammation and oxidative stress :
12. In this study melatonin was given as a single dose orally of 50 mg/kg/bw. In a person weighing 176 lbs, this would be equivalent to 4,000 mg of melatonin in one dose. This single dose study proved melatonin to be safe and well tolerated at this very high dose.
I have tried as much as possible through the use of scientific studies to show the potential of melatonin in PD beyond what the 10 mg study showed in terms of safety and efficacy in PWP in 12 weeks. Beyond what you see above I also drew information and ideas from videos by Dr. Russel J. Reiter Ph.D., MD., D.Sc, who has spent the last 25 years of his life espousing the benefits of melatonin in human health and is a world renowned melatonin expert who believes in his research and work so much that he has taken a minimum of 100 mg of melatonin himself for the past 25 years every night. He participated in over 600 studies according to PubMed.
What is needed at this point is an actual 100 mg+ PwP study to prove or disprove the idea that HDM can positively impact PWP to a much greater extent than the 10 mg study in PwP earlier this year, via returning the redox system to equilibrium while reducing inflammation levels to healthy control levels and protecting dopaminergic neurons from death as already shown in vitro and in animal studies. In the DMD study in children who received 70 mg melatonin / day for 9 months, that study also showed a return of redox status to the control normal level while reducing inflammation markers and muscle damage, but it took the full 9 months of the study in order to achieve those results. Similarly, the ALS study which used 300 mg day for up to 2 years also showed a return to control value in terms of oxidative stress. The longest study I found so far is 5 years at 100 mg /day.
I am very interested in seeing if HDM can return redox equilibrium and return inflammatory levels to healthy control levels as shown in other human studies not for PD. I want to know if accomplishing that will significantly slow or stop disease progression and ameliorate symptoms in PwP.
I am not recommending anyone try this idea and definitely not without a doctors support. I have just gathered what I thought were relevant studies in order to show the potential that melatonin may offer PwP as a potential treatment and how it might do that, given the limited prospects currently available short of DBS or FUS, which are cost prohibitive for the uninsured and underinsured. Melatonin is inexpensive.
Art
Written by
chartist
To view profiles and participate in discussions please or .
Just glanced and seems interesting. Will read in detail during the weekend. I gave my mother 10mg of melatonin for more than 3 months and it did not help. Frankly, very nervous to give her a dose as high as 100mg on a daily basis. You know what I mean. It is going to be a hard decision. Will read and then take some time before going ahead (if at all).
But thanks a lot for the article and all the info.
I understand what you are saying about dosing and I am not recommending others take such high dosages. I have taken up to 180 mg of melatonin myself and am currently at the 70~80 mg dose range, because like B1 that I have written about, I wanted to know as much as possible about what I am writing and describing to others so I experimented with B1 up to 4,000 mg day for about a month when I had to stop as it gave me a tremor. My hope is that a research group will do a study of 100 mg or more for PD just as they did on those athletes. There are high dose studies in humans and some were for significant duration, but there has not been one in PwP, only the 10 mg study which did show clear and measurable benefit in PwP!
That's actually very sensible of you. Melatonin is a hormone, it's not a harmless supplement to experiment at such a mega dose despite all the positive highlights, especially while not being actively monitored by a physician.
I asked my pharmacist how high I could increase my 10mg melatonin for my REM sleep disorder. She said that because it is a hormone, the max dose was 10 mg. I didn’t want to create an hormonal problem on top of all my pd symptoms, so I listened to her. Thanks for the links.
Yes it’s a worry isn’t it. The doctor can prescribe and if it goes wrong it’s tough but if a caregiver does it will all get blamed on us if anything goes wrong.
I have tried melatonin before bedtime to improve sleep but find even a low dose (5 mg) leaves me feeling hung over and groggy in the morning , Does anyone have experience with taking it during the day?
You are correct, some people simply can not tolerate melatonin.
I have felt the melatonin hangover and I have taken it during the day to try and replicate a human study I had read years ago where they used 70 mg/day of melatonin in children for 9 months.
What I have found with melatonin is that the hangover normally lasts for 2 to 3 weeks as my body adjusts to having significantly higher levels of melatonin. After 3 weeks, the hangover has faded away.
One thing that helped me with the hangover was staying as busy as possible during the adjustment period instead of just sitting. If I sat at my computer or just read a book, the hangover was very noticeable and I could easily fall asleep sitting down during that period.
Hi Chartist, perhaps I missed this bit but what are the beneficial effects that you have observed in yourself taking the optimal dose of melatonin? Many thanks for the post
I do not know the optimal dose of melatonin. I am experimenting and my best guess is it likely depends on what you are trying to treat. Apparently cancer and ALS require ultra dosing, but Covid -19 only requires high dosing. I have bumped my current dose to 80 to 90 mg/night, but have gone up to 180 mg/night for a brief test.
It has helped bring my severe erythrodermic and pustular forms of psoriasis to about 96% of normal. Both of these rarer forms of psoriasis can be deadly and are extremely hard to control. Here is what they look like :
I looked like some of the worst images in those pictures and had about 95% coverage where it was impossible to see any significant area of clear skin. Oddly some bottles of melatonin say not to use it on an autoimmune disease like psoriasis, but I beg to differ.
I think the dose Dr. Neel is using in his Covid-19 patients is a reasonable general guide based on what I have read. He uses 1 mg per kilogram of body weight and some times higher if he feels it is a tougher case since he has seen two different strains in his practice. Although it varies by the person, when used in a combination as I previously posted, it is quite effective as a sleep aid for me and better than melatonin alone!
In this post is a link to a study where they used a 100 mg melatonin intravenous injection and it produced no side effects or sedation in humans. So this may turn out to be one way to avoid the next day "melatonin hangover". This study is somewhat more important than the 100 mg a day study in athletes which I referenced in the post, because oral melatonin is poorly absorbed with some estimates as low as 3% absorption, whereas the 100 mg injection all goes directly to the blood and could potentially be over 6x stronger than the same oral dose, but more studies would be required to determine accurate serum levels.
I see a parallel or two between melatonin and B-1. One, is the difference in dosing required to achieve an effective dose from an injection as opposed to an effective dose from oral dosing. The other is that some people chose B1 based primarily on its established very good safety profile rather than the incomplete scientific evidence and if studies for HDM in PWP never materialize, there may be a future patient or two who may try HDM based on its established very good safety profile as opposed to incomplete scientific evidence. Obviously, melatonin has many more human and animal studies suggesting applicability to PWP than B1 does and we already know that 10 mg orally has shown benefit in PWP. Now to wait for an HDM study for PD.
Husband stopped B1 injections and that was a huge mistake. We had problems getting the prescription filled in my state although our internist was always willing to prescribe it and he did for a while, but then we had problems with finding someone to inject it. He had to go for an office visit just for the injection which was $50.00 copay weekly. He got tired of driving the distance and pay on top $25 copay. That is why he decided to go oral, but I sure can tell the difference between IM vs oral B1! He is thinking about starting IM again.
Waiting for an HDM study for PD will be long, IMO. If doctors can prescribe HDM, then I would encourage my husband to try it.
By the way, regarding Wriga's latest post, I found this supplement and ordered it--received it today.
Why did your husband stop his B1 injections in the first place? I thought he was at or very close to his optimal dose? If the difference is significant between oral and injections for him, it definitely seems like he should go back to the IM.
I am going to be adding safety information to the original post above. I have been working on that post for awhile and have not had a chance to delve into much else and gathering the safety data is taking time. I will say the information I have found so far is interesting!
It became complicated with unavailability of IM B1. It's not available in my state for starters. Once we found it out of state (originally California and then Missouri), he had to drive about 20 min to have the injection at our Internist's office. On top, he had to pay $50 for an office visit. If he decides to go back to IM, we have to start looking for a state where it's available and they accept out of state prescriptions, don't know anymore!
Please let us know any new information you find about HDM.
That is a very tiny pill! It looks like a sublingual homeopathic pill. I have found that when I first start at a higher dose of melatonin than I have previously been using, it is helpful to try and avoid the melatonin hangover by staying very busy during the day. Let us know how it goes for you.
I look at how close science is to possibly testing melatonin at high dose for PD and I am happy about that, but waiting for the actual study is like watching paint dry, so I hope it comes soon because such a test offers hope for other neurodegenerative diseases also. The high dose has been used in other studies and melatonin has proven safe in other studies for longer time frames. Hopefully that study will happen soon!
Wow, did you read the whole post? That was not what I recommended. I suggested waiting for a high dose study similar to the 10 mg study to be safe about it. Melatonin has a good safety profile, but there aren't any high dose melatonin studies specifically for PD yet to prove the safety and efficacy of a high dose in PWP. The 10 mg study took 12 weeks to see benefit.
grrrr that's what I was afraid of. Art, I know you mean well and thanks for posting all the research tirelessly on the topic but this can backfire and you can't blame people for wanting to jump in after seeing all the potential positives while you promote the supplement as your favorite - that's been the big concern I have.
I'll be on the lookout for your safety disclosures that you've been working on to go with these posts.
Last but not least, in italy there is an anti-cancer therapy created by Dr. Luigi Di Bella many years ago that is rising from the oblio and becoming more and more popular and proven, that uses large amounts of melatonine, in a specific formula with adenosine & glicine to be highly bioavailable and active. The site lists an impressive number of studies on melatonine divided by: in vitro, in vivo (only animals), reviewed, Comments of the author, preclinical studies, in vivo (only on humans)
In the original post at the top of this thread, I linked to an abstract that used melatonin in children with Duchenne Muscular Dystrophy (DMD) at a rate of 70 mg per day for 9 months continuously to very good effect. I had never seen the whole study, but now that I have, their study showed a return of the redox status to that of normal controls as well as a reduction in markers of inflammation and reduced muscle damage from the disease process. Think about that. DMD is a genetic disease and they were still able to reverse the two main damaging effects of it, excess oxidative stress and inflammation and thus reduce the muscle damage more than any other study for DMD has done before or since!
What they did in that study using melatonin along side of standard care is achieve more than all of the science applied to DMD research has ever done. The 70 mg dose that the children received may be comparable to a 100mg dose in adults, but they have never attempted a similar study in any of the different forms of muscular dystrophy for children or adults.
Unfortunately, beyond their follow up abstract, there has been zero further testing of melatonin in any of the muscular dystrophies other than animal studies and that 70 mg study was done in 2010! Sad, but true. Normally when a study has success like that, it is assumed that further studies along that line will be done, but clearly that is a wrong assumption!
I added human studies at the bottom of the original post that illustrate the safety of high dose melatonin for years of use and some I would describe as ultra high dose. This part is above the conclusion paragraph and is numbered as 1 ~ 10.
If you do not have time to read this very lengthy post, I have added this short summary to quickly and easily understand what I am trying to say :
CONCLUSION :
I have tried as much as possible through the use of scientific studies to show the potential of melatonin in PD beyond what the 10 mg study showed in terms of safety and efficacy in PWP in 12 weeks. Beyond what you see above I also drew information and ideas from videos by Dr. Russell Reiter Ph.D., MD., D.Sc, who has spent the last 25 years of his life espousing the benefits of melatonin in human health and is a world renowned melatonin expert who believes in his research and work so much that he has taken a minimum of 100 mg of melatonin himself for the past 25 years every night. He participated in over 600 studies according to PubMed.
What is needed at this point is an actual 100 mg or more PWP study to prove or disprove the idea that HDM can positively impact PWP to a much greater extent than the 10 mg study in PWP earlier this year(2020), via returning the redox system to equilibrium while reducing inflammation and protecting dopaminergic neurons and mitochondria from death as already shown in vitro and in animal studies.
In the DMD study in children who received 70 mg melatonin / day for 9 months, that study also showed a return of redox status to the control normal level while reducing inflammation markers and muscle damage, but it took the full 9 months of the study in order to achieve those results. Similarly, the ALS study which used 300 mg day for up to 2 years also showed a return to control value in terms of oxidative stress. The longest study I found so far is 5 years at 100 mg /day and this is longer than most drug trials by a very significant amount.
I am not recommending anyone try this idea and definitely not without a doctors support. I have just gathered what I thought were the relevant studies in order to show the potential that melatonin may offer PWP as a potential treatment and how it might do that, given the limited prospects currently available short of DBS or FUS.
Art, I apologize if you cited a particular study, article, or video which verifies this, but I missed it. How do you know Dr. Reiter has personally consumed 100+ mgs per day for more than 25 years?
Those words came right out of his mouth in the following video which I already posted . Here is a link to the video and below the video it says where to scroll to, so you don't have to watch the whole video to here it :
He is involved in so much research regarding melatonin that it would be impossible for him to convey all of his knowledge on the subject in one or two videos, but he does try. When you search him, he has been involved in over 1500 studies!
I'm dying for that study to happen. One downside for some people who take melatonin is that they report feeling sleepy the next day. In that post in two studies it was reported that intravenous melatonin and melatonin in the available suppository form avoided the sleepy feeling completely, so apparently there is a work around for that sleepy issue!
I don't even know how they recruit for supplement studies, probably similar to drug studies, but much less elaborate, but that is considerate of you to offer. One good thing about melatonin is that they have never been able to establish an LD50 for melatonin. Dr. Reiter has never had an animal die from melatonin at any dose and I am not aware of any reports of people dying or being severely injured in any of the hundreds of studies I have read about melatonin. Some of the studies I link to for safety of HDM used doses way beyond 100 mg for years with no major side effects!
Thanks a lot for this post. I am really been struggling with insomnia lately. I took fairly high dose, (35mg) I slept great( as good as Parkinson’s patients can sleep) I’ve had a much better day today.
I know you are a fan of up regulation of >>> BDNF <<< as others on this forum are also. You will be happy to know that the most potent antioxidant and radical scavenger in the body, melatonin, does that too, at least in animals and possibly in humans, but I haven't looked for that yet, but I will!
It seems like it, doesn't it? I think the reason why is we have become accustomed to thinking of melatonin as just a very low dose sleep aid.
The U.S. Institute of Medicine of the National Academy of Sciences has established Adequate Intake (AI) levels for vitamin D. The daily levels in International Units (IU) for everyone are as follows according to age: Under the age of 50: 200 IU. From 50 to 70 years-old: 400 IU., but how often do you now hear people say they are taking 5,000 iu or 10,000 iu or even more? I have even seen studies where they are using 35,000 iu of vitamin d per day in humans to good effect over 6 months!
I think as studies reveal more information about these bodily made molecules, the health benefits are better understood and new studies continue to push the envelope until unhealthy results are obtained and a more realistic dosing limit is established.
I started taking Melatonin a couple months ago. started at 1 and then 5 mg, which is infinitesimal when you recognize that your blood stream only get 3% of that. I am currently using Natures Bounty 10 mg. from COSTCO (Canada) . In between I had problems getting the NB brand , a long 3hr drive one way , and the Co-Vid etc forced me to try a different brand at Shoppers Drug , Webber Naturals, they had a large variety of formulations, one with a slow release 5 mg and 5mg of fast release, so fast it was like a Sublingual tablet, and the other was a 10mg. of Melatonin and 150 mg Magnesium containing "Natural Chocolate" - No SUGAR .... with a strange taste.
I thought that I might b e able to not take one of my 200mg of Magnesium Bisglycinate, the PM dose. After the 60 tablets, 1 bottle, were gone I went back to the Natures Bounty and re-added the dropped Magnesium Bisglycinate , 1 Capsule AM and one PM, the absorbtion much better and the cramping much reduced over 24 hrs.
Another point , (I was not getting a consistent sleep on-set not in total time,) I re-read one of the TIMING of Medications posts here about a mention of interference of Synamet, proteins and other drugs and SUPPLEMENTS, it recommended a good period between... so for the sake of seeing if there is any interaction , I took # 1 starter Melatonin pill 60 min before lights out and #2, scant minutes before with the rest of my supplements..... After 3 nights I have slept from ~ 10:30 PM - 11PM to 5 AM , a consistent wake up time for a relief break, a Synamet dosage and 2 hrs. more light sleep.
Comparing the stiffness, when first rising , between the 2 varieties, Magnesium BisGlysinate is the winner for me.
Will go a full week now before adding another 10 mg. of Melatonin
The magnesium glycinate /magnesium bisglycinate is fairly well absorbed, helps to gently relax muscles and is very good as a sleep aid in conjunction with melatonin and if you add in zinc, the three are synergistic together for sleep. I posted about it here :
For the purpose of sleep, you will find that some melatonin has vitamin B6 in it which helps increase melatonin absorption a bit, up from the 3% absorption. So it is good at low dose for sleep in combination with the zinc, magnesium and melatonin combo, but not a good source for high dose melatonin as that will give you way too much B6 and that can definitely be a problem!
Are you having any problem with next day sleepiness? I sometimes have that problem when increasing my dose, but it has always been temporary as my body adjusts to the higher dose and I did not even notice that issue on my last increase, so I suspect my body is adjusting. Staying very busy has helped me work around that issue in the past and going out in direct sunlight for a short period of time is also helpful until I adjust to the new dose. I'm currently at 80~90 mg/night, but tonight I am going to bump it up to 100 and just try hanging there for a minute. I've been higher, but since I have written about 100 mg, I am going to try it out again for a minute.
I have been checking on some of the different types of melatonin that are available and have made the following list of the different types which I thought might appeal to different users:
1. Capsules or pills of varying dosages up to 60 mg per capsule.
2. Intravenous injection and multiple dosing, but this form very likely delivers more melatonin per mg than oral route due to better absorption as melatonin orally is very poorly absorbed at just 3% according to one study, but this varies person to person.
One positive to this form is that it was shown in at least one study to avoid the next day sleepiness or "melatonin hangover".
3. Sublingual melatonin to be absorbed under the tongue. Purported to enter your system more quickly, but oral melatonin enters the system quickly also.
4. Timed release. Has been reported to be more effective to help some people sleep than instant release melatonin and is thought to mimic natural melatonin release by the pineal gland.
5. Delayed release.
6. Chewables/gummies for people who have swallowing issues or children.
7. Combination product with instant release and delayed release in one pill or capsule.
8. Suppository form which according to one study did not cause any next day drowsiness or tiredness. It comes in very high dose of 200 mg or 400 mg. I imagine the high doses are for rapidly advancing diseases like ALS or cancer. Potential for gastro upset is mentioned as a possible side effect of regular melatonin. I wonder if this form would avoid that issue?
9. Liquid form from a bottle that you apply under the tongue with an in bottle dropper.
Again, useful for people with swallowing issues.
10. A vape form that you inhale just like a pen vape and delivers melatonin in the vapor. I wonder if this form would be useful with Covid-19 since it goes directly to the lungs. I also wonder if it might target the brain more than other forms? It only delivers low dose, but if it is really well absorbed this way, perhaps it is okay and I also wonder if this method can avoid any gastro issues? If higher doses are eventually made, this may be a way to target the brain a little quicker than the oral route? On the other hand oral dosing still covers the whole body including the brain, less expensively.
11. Topical melatonin cream, probably not as helpful for sleep as there is a bit of delay with absorption as the melatonin traverses the dermal layers. It will take trial and error to determine the correct timing for each individual. On the other hand if you are using it for skin issues, it seems perfect.
12. An oral spray form which may offer a bit more convenience and usability by people with swallowing issues.
I will check further and add any other types of melatonin I find to this list for easy lookup. If anyone else is aware of other types, please post them and I will add them to the list. Thank you!
The following study linked to below, explains how excess oxidative stress is a main cause for the damage in the brain of PWP. Even the normal function of dopaminergic neurons causes significant oxidative stress as does the dysfunctional mitochondria seen in PWP.
Neuro inflammation also comes into play because it too can add to the total oxidative stress burden seen in PWP and this increased oxidative stress from inflammation, results in further neuroinflammation. Together this continues the vicious cycle of oxidative stress and neuroinflammation which just continues to cause damage and death to the dopaminergic neurons and mitochondria, resulting in continuous disease progression and continuous worsening of symptoms.
This article also discusses standard antioxidant supplements such as vitamin C, vitamin E and Coenzyme Q10 or Coq10 and how their actions are not sufficient enough to have much if any positive effect against the high oxidative stress levels seen in PWP. They do however show how Doxycycline(Doxy) can have some effect and I believe it has been reported on this forum by one or two people that doxycycline had a positive impact on their symptoms when they were taking a course of it for other health reasons and this tends to confirm the reason why, as doxycycline crosses the blood brain barrier and reduces some neuroinflammatory mediators which can reduce some of the oxidative stress.
This is what Doxy did in this study :
1. Suppressed MMP3 gene expression
2. Suppressed Nitric Oxide
3. Suppressed Inflammatory Cytokines
4. Provides protection of the nigral dopaminergic neurons
As expected, melatonin crosses the blood brain barrier and has these same effects and many more which also target different aspects of PD such as increased gene expression of many of the body's own natural antioxidants while also activating Nrf2 and suppressing KEAP1 and acting as a scavenger of multiple radicals, while protecting the mitochondria.
Melatonin is a myeloperoxidase inhibitor. Currently there is a clinical trial running on Verdiperstat, a myeloperoxidase inhibitor, for multiple system atrophy.
Thank you for that, Rhyothermis. Melatonin has so many positive benefits for human health and the drug companies have tried to create their versions of it, but all of them have fallen short of melatonin, by a huge margin. I hope they find something soon for MSA because that one can move really fast. It seems like many diseases that have excess oxidative stress and excess inflammation at their core, may benefit from melatonin. I remember that Dr. Costantini had said that HDT/B1 could help MSA if given early enough, but at a higher dose. At least that was his experience.
Ryothermis, you bring up another good reason to consider melatonin for PD as myeloperoxidase does damage in PD and of course melatonin works against it according to this study.
Hi Art. Thank you for all your hard work and for sharing. My husband finds the time release melatonin most beneficial compared to the immediate release. It enables him to get back to sleep after his many pee trips at night. He is now on 9 mg melatonin and 2 capsules of magtech. I have just ordered the coffee fruit that Getz recommended. After his recent maintenance BCG treatment for bladder cancer he has been waking up 7-10 times a night. It has set us back from the 2-3 times a night. I will slowly work his melatonin dose to 20 mg
You're the one who brought up Dr. Shallenberger, have you considered doing a phone consult with him about your husbands case? It will have to be round the clock dosing at much higher dosing though. Here is a phone listing : (775) 884-3990
Zinc and melatonin have synergy just as melatonin and curcumin do and curcumin and zinc have shown synergy together, so giving consideration to zinc seems reasonable. Zinc also helps with sleep.
Thank you very much Art for the reference articles and contact. Do you happen to have his email contact? You are right about the round the clock dosing- just apprehensive about dose. It is overwhelming to have to deal with PD and bladder CA as well. I will try and email Dr Shallenburger with details and see what he suggest .
If you do decide to incorporate curcumin, it may be worth considering curcumin with piperine in it because although piperine is proven to very significantly enhance bioavailability of curcumin, which is poorly absorbed on its own, piperine itself has anticarcinogenic qualities!
Studies of animal models of MSA indicate that myeloperoxidase inhibition works well if given early but not much if given later. Unfortunately MSA is diagnosed late. Experts say they want early diagnosis, but doctors seem reluctant to make the diagnosis since it is so devastating - which seems counter-productive to me. Neurofilament light chain testing could be helpful - at least it might help those patients who are told their symptoms are 'all in their head' (if doctors are willing to order the test). Japanese researchers are developing a blood test based on phosphorylated alpha-syn in red blood cells.
~
OT - Avenanthramide-C prevents amyloid formation of bovine serum albumin
If it is a non-specific inhibitor of protein aggregation like anle138b, then it could be broadly effective. Avenanthramides are from oats. I eat a ton of oatmeal.
MSA, yes, Dr. Costantini also said that early treatment saw better results in his MSA patients. The rate of progression being what it is in MSA, it is easy to see why early treatment is critical.
Again, this is definitely an area where melatonin has shown inhibitory activity of a/b and fibril formation.
In PD, Sirtuin1 (SIRT1) is known to have neuroprotective and antiinflammatory effects . The following study discusses this at length as it relates to diseases of neuroinflammation such as PD and AD :
This study above also suggests that SIRT1 can ameliorate depression and anxiety associated with neuroinflammation.
In the study link below, it is shown that melatonin promotes SIRT1 as well as Nrf2 and this combination ameliorates much of the damaging effects of neuroinflammation. So this shows another piece or two of the puzzle that is PD. Albert has discussed the Nrf2/KEAP1/ARE pathway at length and this study tends to mirror all that he has described of this pathway which promotes the antioxidant system in the body leading to increased total antioxidant capacity (TAC).
This study further illustrates some of the protective actions of melatonin as regards neuroinflammation. Promoting SIRT1 in the brain, as melatonin does, is also shown to be beneficial in controlling neuroinflammation as well as the subsequent depression and anxiety. Melatonin also protects microglial cells against "pyroptotic cell death" and this is another important aspect of the neural protection that melatonin affords!
Here is another human study in children who were given 70 mg/day of melatonin for 6 months to try and treat Charcot-Marie-Tooth neuropathy (CMT). The results showed that melatonin returned hyper elevated oxidative stress levels and inflammatory levels to normal control values. These results are very similar to an older study using the same melatonin dosage in children with Duchenne muscular dystrophy (DMD) with the same outcome of achieving redox equilibrium and return of elevated inflammation markers to that of healthy controls. In that study it took 9 months for the children to reach healthy control levels, but DMD is a serious disease that attacks the muscles and results in death between the age of 20 and 30 years of age on average.
So once again it is confirmed in human studies that melatonin can return elevated oxidative stress levels and elevated inflammatory levels to healthy control levels.
I have been reading about piperine and it turns out it has many potential benefits in PD and it has some similarities with melatonin in that it significantly reduces oxidative stress, neuroinflammation, dopaminergic neuron death and apoptosis as well as also being an activator of the Nrf2/KEAP1 pathway. Piperine is typically used to increase bioavailability of some supplements such as curcumin and resveratrol, but it also has many other effects of its own such as having anticarcinogenic effects as does melatonin.
For now though, melatonin appears to affect many very important aspects of PD in a very positive manner and on that note, I am continuing my melatonin test of 104/mg night.
With a little more reading, it appears that piperine has no synergy with melatonin, so I won't use the two together, but will likely take both, just not at the sametime.
I've been using black pepper essential oil for the piperine benefits, having added it to cedarwood for the sesquiterpenes, glad to hear it may work well with melatonin, which I've been taking low dose for awhile now for sleep and immune system. I have been able to get my CRP levels down quite a bit lately thanks to scrutinizing my diet. I am going to try slowly upping the melatonin to see if that helps as well for the inflammation. I would really like to get it down to an acceptable level, sooner the better, since I know it's not good for the brain. I see that as a long term benefit, although I know it can be instrumental in reducing body pain as well, in the here and now. Thanks for all your info on this.
Now it would be nice to see a 100 mg study in PWP! I am currently testing 104 mg in myself.
In multiple high dose studies, melatonin was able to return the redox status and the elevated inflammatory levels to healthy control levels and that would be highly desirable in PWP, but a 100 mg PWP study has not occured yet !
Wow that is an awesome amount of data you have gathered on melatonin. Thanks for warning me about the other stuff. Probably just need to get the suppositories. It really looks like it is beyond beneficial!
The article linked to below discusses many of the protective effects of melatonin in ameliorating the effects of free radicals in PD and gives limited comparisons to other molecules that are well established as being useful in PD such as curcumin, EGCG, Trolox, alpha lipoic acid, acetyl l carnitine, nicotine, resveratrol, creatine, nicotinamide, etc.
This is probably one of the most detailed articles I have read on how melatonin protects dopaminergic neurons and cellular mitochondria from death, oxidative stress and how it works toward mitochondrial homeostasis through its multiple antioxidant effects as well as direct and indirect radical scavenging.
The article further describes how excess oxidative stress is a major component of the disease process and how melatonin effectively works against this damaging process. This has been confirmed in other human studies for other diseases where melatonin was shown to return the redox status to redox equilibrium over a period of months.
The article is long, so if you don't have time to read the full article, the conclusion/summary near the bottom of the article is definitely a worthwhile and quick read.
Overall, this study, although being done in 2013, further highlights the need for a high dose melatonin(HDM) study specifically in PwP. The 10 mg study showed significant benefit in PwP, but an HDM study is more likely to expose the maximum benefit that melatonin has to offer PwP.
On that note, I am still at 104 mg melatonin per night.
I've never seen a molecule that can do everything that melatonin can do. It is protective of the organs of the body, the most potent antioxidant in the body, very good safety profile, can be useful against multiple diseases including Covid-19, PD and AD. Being a sirt1 activator, it is thought to have life extending effects as well as being anticarcinogenic. It activates Nrf2 and can improve hair growth. It significantly reduces inflammation. It can help to quell the cytokine storm caused from multiple health issues. It reduces ldl cholesterol. It can help restore circadian rhythms. It protects mitochondria and dopaminergic neurons. It can help with RBD. It helps some people sleep and the list just goes on and on!
I just got done reading this study that shows that melatonin levels are associated with hypothalamic gray matter volume loss and disease severity in PwP.
There is an inverse correlation between melatonin level and disease severity. Correlation does not prove causation, but the 10 mg melatonin RCT in PwP this year tends to prove cause and effect.
In the study abstract below, the neural protective effects of melatonin are discussed. Here is a quote from the brief abstract :
>>> ' melatonin administration showed a total neuroprotective effect in both regions of the substantia nigra. In conclusion, the data here show that melatonin is neuroprotective against mutant alpha-synuclein-induced injury in the substantia nigra. ' <<<
It seems like when I look at problems occurring in PD, melatonin almost always has an ameliorating effect against those problems. Here is a link to the study abstract:
Based on available studies, some studies suggest that PwP men are at elevated risk of prostate cancer (PC) while other studies say that PwP men are at the same risk as the general population while other studies suggest a decreased incidence of PC in PwP men. This means that the science is not yet positively conclusive.
In any case, if it turns out there is increased risk of PC in PwP or not, this new study abstract suggests that melatonin can increase survival when used alongside of standard of care and since the chance of getting PC increases with age without a doubt, the following abstract is relevant:
Although that particular gene variant appears to be an issue in terms of lowering insulin production as relates to melatonin, the actual main damage being done in T2DM is from elevated oxidative stress levels and elevated inflammatory levels and reducing those significantly should increase insulin sensitivity and lower the demand for insulin, making that gene variant less of an issue in terms of decreased insulin production. The reduced oxidative stress and reduced inflammation should also result in reduced damage to beta cells. It should be noted that while low doses of melatonin may not be helpful with that gene variant, HDM is likely to improve disease parameters.
Look at this study using HDM 250 mg/day of melatonin in diabetic patients and look how the total antioxidant capacity (TAC) was improved over an 8 week period! These improvements are likely to increase beyond the study period as mitochondrial protection and repair as well as cellular repair further lowers oxidative stress levels over time beyond the study period.
Melatonin seems quite adept at dealing with many PD associated issues as well as other disease states, unfortunately melatonin levels decline as we age and by the time we reach 50 years of age, production is back down to the level of a 1 year old baby. By age 65, melatonin levels are negligible. Declining melatonin levels when we need it most is not a good thing in terms of diseases that are age related such as PD and AD, but melatonin supplementation has already shown benefit in both diseases at low dosage such as 10 mg/day.
What is lacking is high dose studies of melatonin in PD and AD. This 2020 study in T2DM patients using 250 mg / day of melatonin for 8 weeks clearly shows that melatonin starts to return oxidative stress levels and inflammatory mediators toward homeostasis in just 8 weeks.
Although this study is not about PD, it is important in terms of further illustrating and confirming that HDM can lower these oxidative stress levels and inflammatory markers in multiple disease states.
ncbi.nlm.nih.gov/pmc/articl...
In other HDM studies of longer duration melatonin does return redox status and inflammatory mediators to equilibrium or to levels of healthy controls and that would be a very good thing for PD and AD among many other diseases. Melatonin has shown the ability to be produced in the mitochondria in order to protect against oxidative stress, but when native production in the mitochondria is insufficient, the mitochondria can draw melatonin from outside of the cell, if it is available, to improve protection status via increased TAC. Melatonin is also protective of dopaminergic neurons in the substantia nigra and can protect them against oxidative stress and inflammation.
In general, human studies show that melatonin dose and time dependently improves oxidative stress and inflammatory mediators to levels of healthy controls. Add in the anticovid-19 activities of HDM, anticarcinogenic activities of HDM and its very good safety profile and this would be a blockbuster drug if pharmaceutical companies could patent it.
This would be in line with the 10 mg/melatonin/ PwP study which noted less digestive issues and less sleep issues in the active treatment group, but not in the placebo group. My interest is in a 100 mg or higher melatonin study for 6 months or longer in PwP to see if HDM can return redox status to equilibrium and if it can also lower inflammatory mediators to healthy control levels to see if doing so can halt disease progression and alleviate symptoms.
I have been giving more thought to the use of melatonin to reduce oxidative stress and inflammation to healthy control levels or redox equilibrium. My thinking is that although melatonin has already shown the ability to do this in other high dose human studies, it mainly works at night, but it would be useful and more effective if it also worked during the day at the same level it does at night, but daytime use is generally limited to cancer or other potentially fast progressing diseases such as ALS, plus daytime sleepiness is more likely to be an issue with daytime use and daytime use would likely disrupt the circadian rhythm, and not in a good way.
So based on that idea, I think using another supplement during the day may help to speed up the process so that it doesn't take melatonin many months to reach redox equilibrium as other studies have shown using melatonin in humans.
There are a few supplements that I would consider for this purpose, but I think Acetyl L Carnitine(ALC) is a reasonable consideration for this purpose and it has shown in PD rat and mouse models to have benefit and it also has a very good safety profile in humans. I plan to test ALC in time and I am currently considering dosing in the 1 to 2 gram range, but that may change once I get around to testing it.
In my last update to this thread, I mentioned the addition of Acetyl L Carnitine to melatonin as a complementary daytime treatment with melatonin at night before bed as a means to possibly speed up the length of time melatonin has taken in HDM studies to achieve redox equilibrium since melatonin works mainly while we sleep but is not practical or advised for daytime use except possibly in fast moving, often fatal diseases such as cancer, Covid-19 or ALS.
I would like to add one other alongside ALC, piperine which has similar neuroprotective effects as ALC and melatonin and it does this at relatively low dose. It also has another interesting effect in that it can turn melatonin down during the day which may help people who find melatonin tends to make them sleepy during the day.
All three are Nrf2/KEAP1 pathway promoters.
So melatonin at 100 mg + at night, ALC at 1 to 2 grams with piperine at 20 mg in the morning with breakfast. One other to consider would be quercetin because it has shown synergy with melatonin and piperine in studies, but the three seem to have multiple protective effects of the brain on their own, as all 3 cross the blood brain barrier and help to protect dopaminergic neurons and mitochondria from elevated oxidative stress, death, apoptosis and elevated inflammation levels in PwP. These 3 do much more than that, but those would be a great start in the fight against Parkinson's disease progression. The addition of these two is to speed up and increase the efficacy of melatonin to weeks instead of months to reach redox equilibrium and to return elevated inflammatory levels to healthy control levels.
I'm still at 104 mg/night of melatonin and just ordered ALC and already have bioperine and will begin this phase of the experiment as soon as the ALC arrives.
Art: "My thinking is that although melatonin has already shown the ability to do this in other high dose human studies, it mainly works at night, but it would be useful and more effective if it also worked during the day"
For this purpose, the forbidden French trial was using Valentonine, the real sleep hormone, plus 6-MH:
3mg of Melatonin at 10pm on the dot. orally served with a night patch containing 400micrograms of Valentonine and 100micrograms of 6-Methoxy-harmalan.
I have been giving more thought to the idea of what to add to melatonin as a potential regimen for PD or other health conditions. Although melatonin is a great supplement with huge potential, when you look at its activity a little closer, you realize that it is only highly active for a fairly short period during the night of about 6 hours and I think this explains why the earliest that I have seen melatonin in studies reach redox equilibrium is 3 months while other studies have shown 6 to 9 months. No matter how potent HDM is, if it is only active for approximately 1/4th of the day, it is going to be slow to show positive effects such as redox equilibrium or the return of elevated inflammatory levels to healthy control levels.
In that line of thought, I have been considering other supplements that may have somewhat similar activities to melatonin that could be active during the remaining hours of the day in order to speed up the process of reaching redox equilibrium and reduction of elevated inflammatory levels to healthy control levels.
The supplements I am currently looking into are acetyl l carnitine, bioperine and hesperidin.
I have seen ALC cause sleeplessness at night, especially when combined with alpha lipoic acid (ALA) and since insomnia is a common complaint in PwP, ALC may have to take a backseat to piperine and hesperidin. Bioperine has an interesting effect where it tends to degrade melatonin and I am thinking that taking bioperine upon awakening might help fend off the "melatonin hangover" for those who seem to be sensitive to it. Bioperine is well noted for having neuroprotective effects and these effects could become active during the other 3/4ths of the day when melatonin is not very active at all.
As far as hesperidin, I am currently testing it myself alongside HDM, for its highly potent antioxidative stress and antiinflammatory qualities and I must say, I am very impressed with hesperidin. One of the main reasons I am impressed with hesperidin is because of its very good safety profile which is always important to me.
As I have noted before, I have severe psoriasis in its two forms which are both capable of killing you if they run too far amuck. I never thought I would say this about the psoriasis that I have, but in a sense, it can be very useful in determining the efficacy of drugs and supplements, because positive results by whatever you are testing can be seen very quickly whether it be drug, supplement or alternative treatment. In my case, I am testing hesperidin as the other supplement that can be useful for the other 18 hours of the day when melatonin is not or is barely active. Recently I had a serious flare up of erythrodermic psoriasis with an intense pustular psoriasis at the same time. This flare up rapidly covered at least 50% of my body in just a few days and was rapidly spiraling out of control. It was looking like I was going to have to go to the hospital in just another day or so. I have previously tested hesperidin multiple times in the past and had found it fairly effective at reducing inflammation, but that testing did not exceed 2,000 mg/day. Due to the severity of my condition as well as the very good safety profile of hesperidin, I decided to take my dosing up significantly to see if it could potentially slow the current flare up in conjunction with the HDM I am also taking.
I raised my dose to 2.5 grams of hesperidin with breakfast and 2.5 grams of hesperidin with dinner or more than double my previous hesperidin dosing, for a total of 5 grams of hesperidin per day. To say I was very impressed with the results would be an understatement! On the first day of supplementation, I noticed no difference. On the second day of dosing, I had the impression that the flare up was calming down. On the third day of high dose hesperidin (HDH), The flare up appeared to stop advancing. On every day after the third day, there was a clear reversal of the flare up and a clear and measureable improvement of the symptoms at a rapid rate that was as fast or faster of a reversal than any other previous flare up I have had, and there have been many.
In about two weeks time, I have gone from at least 50% covered with pustules, lesions and fiery inflamed red erythrodermic peeling skin, to less than 10% coverage, no more pustules and no more brilliant red inflamed erythrodermic peeling skin. What remains are just remnants of what was, and these remnants are clearing at a faster rate than I have previously ever seen with any other supplements I have tested for this purpose.
With psoriasis, you can actually see how fast something is working compared to other things used in the past. What this test is showing me is that, as the hesperidin studies have indicated, It is a highly potent antiinflammatory and highly effective radical scavenger and potent antioxidant. Prior to my recent test of HDH, the best my psoriasis looked was upon awakening which I attributed to the activity of HDM during the night while I slept, but as the light of day reduces melatonin levels, the flare up would fly into action and resume its destructive course. HDH in combination with HDM appears to be giving this flare up a one two knockout punch. At my current rate of clearing, I should be clear by New Years day. I think this is the fastest I have ever cleared. Previously it would take two months or more to clear as much as I have in the past two weeks!
The reason I am discussing psoriasis on this forum is simply to illustrate just how potent HDH is. With an internal disease such as liver or kidney disease, improvements would not be so readily apparent as they are with psoriasis, but I think the potency of HDH would be promoting rapid reductions in elevated inflammation and oxidative stress levels all the same wherever disease is occurring. HDH and HDM both cross the blood brain barrier and enter the CSF. Both are noted in studies for being protective of many different areas of the body.
As it turns out, hesperidin has also shown neuroprotective effects which could apply to PwP.
One last thing I would like to add is that this 5 gram dose of HDH has been very well tolerated by me with no apparent side effects and in fact a possible unexpected health benefit of improved mobility as relates to my spine! I think this information about HDH is very important and worth sharing with the forum members as PD is a disease that is mainly driven by excess inflammation and excess oxidative stress, similarly to severe psoriasis.
It is definitely helping me, but it is my hope that others do benefit from this information! Look at the recent Qunol thread and combine that Qunol information with the post you were responding to regarding HDM and HDH.
I look at that trio and wish there would soon be a PwP study combining those three supplements at high dose, which all three have a very good safety profile and look very likely to synergistically work to the benefit of PwP all while bringing other health benefits with it!
All three of these supplements are heart protective and HDH and HDM are both proven stroke preventatives as well as viable treatments for people who have already had a stroke . PwP are at elevated risk for heart disease and stroke. In my most recent post regarding the use of melatonin to both treat and prevent stroke, the studies are very clear on this benefit.
HDH has shown in studies to reduce gastrointestinal inflammation while also helping to add useful gut bacteria, which to me sounds like a good idea for PwP who are noted for having gastrointestinal issues and constipation. Reduction of gastro inflammation is contributing to the amelioration of the total inflammatory burden of PwP.
All three supplements are mitochondria protective which is extremely important for PwP. HDM and HDH are both neuroprotective. HDH and HDM are both inexpensive and readily available in the US. This trio would be an excellent combination toward improving overall health, but they clearly show potential to be very beneficial for PwP!
Art, I am dumbfounded by the use and testing of high dose melatonin. I’m glad you are so organized and keep files here, for our collective review. Given this information, I’m curious about pharmaceutical grade (2/9/21 edit: replace “mannitol” w “melatonin” ) supplements - acknowledging that therapeutic absorption can be an issue, it makes sense to bump the dosage accordingly.
I have been at 106 mg/night of three different types of melatonin for just over 4 months now. Fortunately I tolerate melatonin quite well!
The post on melatonin and stroke is important because current medicine is underpowered in this area, so having other options can be helpful. If you have ever known anyone who has had a stroke, you will immediately be able to appreciate the usefulness of this post as a preventative measure or treatment option. Here is a link to that post:
I was going to put another post on COPD/melatonin up on this forum, but there was insufficient interest so I just sent it to a few members who expressed interest. For me, I see melatonin as a very interesting molecule that offers multiple benefits for multiple health issues that seems to exceed anything I have previously seen. As you can see from the original post, the long term high dose melatonin study is what is needed. My best guess at an appropriate dose, if I had to guess, is in the 1 to 1.5 mg /kg/bw/day, but a well designed study could also figure dosing out.
You changed the question on me, so my original answer is not of use.If you meant pharmaceutical grade "melatonin", that is all that is available in some countries, but the US is otc. Yes, bioavailability is poor and I believe it is estimated to be about as low as 3% and as high as 15%, but you have to remember that melatonin is converted to metabolites by the human body and that would be difficult to ever know how that actually plays out in the body.
I think this is a game changer: I was totally blown away by the fact that melatonin is not only a sleep aid.
We who think this information important have to experiment with this ourselves.
There is no way you are going to find a multi dose, multi-center, randomized, placebo controlled study with a statistically significant cohort that the naysayers would like.
With a molecule this safe, we have to become the crucible for this experiment 🌺
The following study link shows that melatonin also reduces alpha synuclein assembly while reducing a-Syn cytotoxicity as well as blocking a-Syn fibril formation.
Just thought I would update this post with a new study (2/2021) showing another melatonin benefit for PwP, reduced nocturia (night time urination) using only 2 mg of melatonin per night. Here is a link to the abstract :
This rat PD model study from January shows that HDM in the 6 OHDA lesioned rat model of PD had beneficial effects in terms of motor and memory disturbances in the PD rats, but not in the normal rats . Here is a quote from the abstract that is interesting :
>>>' In animals with PD, melatonin pretreatment exerted a neuroprotective effect, manifested as a significantly decreased number of apomorphine-induced rotations, reduced number of falls in the rotarod test, and improved memory performance. The brain DA and ACh concentrations in the same animals were restored to the control levels, and those of NA and Sero did not change. Our results demonstrate a beneficial effect of melatonin on memory and motor disturbance in 6-OHDA-lesioned rats. ' <<<
The dosing used in the study is high and would be a human equivalent of approximately 3.25 mg per kilogram of body weight . So a person who weighs 180 lbs or roughly 82 kilos would require about 266 mg/day of melatonin.
This new abstract is also of the opinion that melatonin studies in humans in the 100 mg/day range are appropriate and needed based on previous animal and human studies.
I am currently over 5 months at 106 mg+ per night of melatonin. Recently I have gone to 118 mg on some nights.
Hello Art, I have been anxious to report, I’ve started taking 12 mg of melatonin this week. I took 12 mg per night for three days and last night I increased to 24 mg and plan on increasing thanks to all the research you’ve put within our very easy reach. I send you a great big hug of appreciation for the work you put in my friend, thank you. Well as you may know I have tremor dominant Parkinson’s on my right dominant side (my right arm shakes like a leaf except when the ldopa from mucuna reaches the brain and my right foot gets slight cramping and toe curling). I’ve been walking regularly at least 3 miles daily for the past three months, but yesterday I walked 9 miles and I think it’s due to the effect melatonin is having on my health, the cramping on my foot is also greatly reduced and the tremor on my right arm is slightly reduced. I experienced lethargy only on the first day (slept for four hours), then thereafter it has been quite the opposite (lots of energy). I’ve also reduced the amount of levodopa I take and I am able to better manage the tremor without it. I think you have provided us with substantial information backed by solid research and I am eager to see more positive results as I increase dose.
Good to hear from you! I don't know that the benefits you mention are from melatonin, but I am happy you got them and are improved! I'm glad to hear you are doing well and are testing melatonin! It has a very good safety profile for those who tolerate it and apparently you tolerate which is a good thing. Other members have reported testing melatonin.
I would write about many more of the benefits of melatonin as there are many more, but they do not necessarily pertain to PD so are inappropriate for this forum. I didn't put the melatonin post up on this forum regarding COPD because there was little interest in it. That is one of the reasons I take HDM, not that I have COPD, but because melatonin can help prevent COPD and act as an adjuvant treatment.
The other part is that sometimes people just get tired of hearing about melatonin and I understand that. I am mainly using it as a prophylactic against multiple health issues and diseases that it has shown the potential to treat, prevent or reduce symptoms based on hundreds of studies I have read. I'm still waiting for an HDM study for PwP, but it has not materialized and may never happen, but I'll keep my fingers crossed!
Jay, your approach to melatonin supplementing seems fairly safe in case you turn out to be a person who does not tolerate melatonin. Working up slowly can help prevent a bad reaction for those who do not know if they tolerate melatonin or not. Please keep us updated on your testing of melatonin at multiple dosing amounts.
Of those two melatonin products, I would choose the second product in the green bottle because it is a relatively unadulterated product compared to the first one.
This new study abstract below suggests that melatonin is protective of the heart and pancreas while improving glucose homeostasis and improving oxidative stress, inflammation and apoptosis in T2DM rats.
Although this new study is about T2DM, it is important for PwP because they use 250 mg/day for 8 weeks showing that these high melatonin doses are doable!
This HDM study just begs for another one in PwP after showing impressive results in T2DM patients! The 10 mg study was helpful, but it is way past time for a HDM study in PwP!!!
Although melatonin displays almost no side effects, even with high-dose and long-term
administration, in patients in most clinical studies, some adverse reactions of melatonin—including fever, headache, vomiting, thrombosis, drowsiness, hyperkinesia or restless leg syndrome—may occur.
Cellular Mechanisms of Melatonin: Insight from Neurodegenerative Diseases
If you are thinking that you are going to take an active treatment for health issues like PD and not encounter side effects, you will be very disappointed. Metformin is a common drug that is considered to have moderate side effects such as the following:
NAC is a very common supplement taken by many PwP for the purpose of boosting glutathione and is considered to be a fairly safe supplement. Here is a list of side effects for NAC :
Since this is a PD forum, we might as well look at the potential side effects of the gold standard treatment for over 50 years, Sinemet. This one has a crazy amount of potential side effects and yet many many PwP use it effectively :
I used Drugs.com to reference these side effects for the above to make the field as level as possible and what the above links say to me is that, yes, they all have side effects, but melatonin and vitamin D-3 are the safest bets in the bunch. Even vitamin D-3 and vitamin B-1 have side effects and it will be impossible to find any potential treatment for PD that doesn't. I'm not even going to mention the side effects of Amlodipine because that list well exceeds 50 items and is the craziest list of side effects I have ever seen, but patients still use and do well on it, but of course these side effects lists are there because those side effects have been reported for each of the above.
The following study abstract link below, discusses the importance of inhibition of NLRP3 Inflammasome in neurodegenerative diseases such as PD and mentions this inhibition as a potential treatment for neurodegenerative diseases. Although not discussed in this abstract, melatonin has shown itself to be a potent inhibitor of NLRP3 Inflammasome, in fact this is one important aspect of how melatonin is able to rapidly reverse Covid-19 symptoms in Dr. Neel's Covid-19 patients. Here is a link to that new ( March 2021 ) abstract :
That is probably the safest way to test melatonin to see how you react to it. I would not expect 5 mg or less of melatonin to do much except possibly help with sleep, but I no longer look at melatonin as a sleep aid because the benefit seems to vary considerably from person to person, so I just consider it for its many other potential health benefits, but it seems that it takes HDM in order to see those effects. That's why I am currently at 106 mg+ of melatonin per night for the last 6 months and am considering going higher after reading the results of that new 250 mg RCT in T2DM patients that showed significant benefits in just 8 weeks.
I don't have PD, but I want to be as aware as possible about what I am writing about and I have written a lot about melatonin. My main reasons for taking it is to take advantage of its healthful effects and to deter as many potential health issues as possible while potentially extending my life.
B6 helps with the absorption of melatonin, but generally, melatonin studies do not use melatonin with other agents in it and too much B6 can be a problem for some PwP.
For some PwP nocturia is a very real problem that can affect up to 60% of PwP and though this has been passingly mentioned before, it is good to know that just 2 mg of melatonin before bed can be useful to help reduce nocturia.
I am just starting to read Albert's paper about oxidative stress as it might relate to PD initiation and progression. I wanted to write this down while the idea is fresh in my mind because I can see the importance based on what Albert has written.
On page 5 he is discussing axon degeneration and it seems worth noting here that this is another area where melatonin has shown relevance in its ability to promote regeneration of injured motor axons via MT1 receptors as outlined in the following study :
When you start listing the deficits and causes of those deficits associated with PD, melatonin continues to show its ability to ameliorate many of these issues! The body has melatonin receptors throughout, including the brain, so this tends to suggest that the body has many uses for melatonin and the studies are clearly in line with this line of thinking.
This new article link below discusses the cytoprotective effects of melatonin in PD. It also discusses the low levels of melatonin, melatonin receptor 1 and 2 in in the Substantia Nigra and amygdala of PwP. It further discusses the use of melatonin and dosing for REM sleep behavior disorder (RBD).
Here is a quote from the study :
>>> ' Daily bedtime administration of 3-12 mg of melatonin has been demonstrated effective in RDB treatment and may halt neurodegeneration to PD. "<<<
This very brief abstract suggests that melatonin blocks alpha synuclein fibril formation and destabilizes preformed alpha synuclein fibrils. Melatonin also decreased alpha synuclein cytotoxicity.
This full study further highlights the need for high dose melatonin studies in PwP in order to see if melatonin can reverse the low level inflammatory damage as well as prevent the neurodegeneration as it has been shown to do in experimental PD models. These models suggest that starting melatonin early in the disease process may have the best outcome in these models. Early low dose studies in PwP are showing positive results, but the high dose studies in PwP are what is currently needed. Two of these type of high dose melatonin studies have been done in diabetic patients at 250 mg/day of melatonin and both studies showed very positive benefits in these patient groups.
So far, melatonin studies indicate that melatonin has shown the ability to ameliorate many of the issues that come up in PD through potent antioxidant and radical scavenging as well as its potent antiinflammatory effects and neuronal cell and mitochondria protective effects.
Until fairly recently I thought that was the major features of melatonin that might be helpful for PwP, but after reading the very good results of the Fecal Microbiome Transplant (FMT) study where they take the stool from a healthy donor and put it in PwP for the purpose of altering the gut bacteria away from pathogenic bacteria toward more healthy bacteria, creating more of a balance between the good and bad bacteria in the gut for the purpose of significantly improving PD symptoms, I decided to see what effects, if any, melatonin might have on the gut bacteria.
Unfortunately these type of studies are minimal in humans, so I had to look at animal studies (mainly mice) to get an idea of melatonin's effects on the gut bacteria. Interestingly, it appears that melatonin also tends to shift the gut bacteria away from bad pathogenic bacteria toward more healthful bacteria. Here is a link to a mouse study that shows how a moderate dose of melatonin, that is less than Dr. Neel has successfully used to treat his over 1,000 Covid-19 patients, in these mice started to cause this shift toward more healthful bacterial balance between good and bad bacteria. Here is a link to the study :
This study shows a positive shift in the gut biome of colitis mice by melatonin by increasing the ratio of Firmicutes/Bacteroides, inhibition of growth of E. coli and promotion of mucin and wound healing all suggesting that melatonin may be useful for treatment of IBD :
This third review is important for PwP as it discusses melatonin use with exercise and discusses how melatonin works against muscle frailty possibly through the microbiome.
Here is a quote from the review :
>>> ' In our opinion, this review reinforces the relevance of melatonin as a safe nutraceutical that limits skeletal muscle frailty and prolongs physical performance.' <<<
All of this plus what I have previously discussed about melatonin as relates to PD, further illustrates the need for a high dose melatonin study in PwP similar to the two recent melatonin studies utilizing melatonin in diabetic patients at 250 mg/day to good effect.
It is worth noting again that melatonin is released from the pineal gland each night, but is also produced in the gut at a rate of approximately 400 times the pineal gland, so clearly melatonin plays an important part in the body, but possibly more so in the gut. This rate of production and the fact that the body has melatonin receptors throughout suggests that melatonin is very important, unfortunately, melatonin production declines sharply with age and even more so in PwP as the Substantia Nigra is low in melatonin and melatonin receptors when compared to people without PD.
In the mean time I will be searching for human gut microbiome studies utilizing melatonin to further confirm the positive effects that animal studies are showing on the gut microbiome.
The link below to a new study abstract (May 2021) suggests that in newly diagnosed PwP, it was found that Inflammasome NLRP3 is hyper expressed along with the receptor P2X7. This combination is inflammatory in the brain of PD patients and may be able to modulate alpha synuclein.
In the following rat model study of Gulf War Illness (GWI) study it is shown that high dose melatonin (HDM) at multiple dosing levels of 5 mg/kg, 10 mg/kg, 20 mg/kg, 40 mg/kg and 80 mg/kg was able to reduce NLRP3 Inflammasomes starting at 10 mg/kg, alleviated simple and associative recognition memory dysfunction and anhedonia ( The inability to gain pleasure from normally pleasurable experiences), along with reduced oxidative stress, enhanced glutathione and complex III, and reduced NLRP3 inflammasomes, IL-18, TNF-α, and IFN-γ. With each further dose increase, melatonin was able to do even more in terms of health benefit. At 20 mg /kg, melatonin was able to normalize Nrf2 and Catalase. Melatonin at 80 mg/kg activated the BDNF-ERK-CREB signaling pathway, enhanced neurogenesis and diminished synapse loss in the hippocampus, and improved a more complex hippocampus-dependent cognitive function.
It is a rat model of GWI, but the results seem impressive over the 8 week test period. There are no current treatments for GWI other than to try and treat symptoms which has not proven to be effective.
To give an idea of what these doses would like like in an 80 kg (or about 175 lbs.) human :
5 mg/kg - 65 mg/day
10 mg/kg - 130 mg/day
20 mg/kg - 260 mg/day
40 mg/kg - 520 mg/day
80 mg/kg - 1,040 mg/day
If you think you've been poisoned into getting PD via an insecticide or other toxic agent such as Agent Orange, GWI seems more like Agent Orange on steroids if you read the study! These results further highlight the need for an HDM / PwP study!
So it is well established from the previous posts in this thread that melatonin has multiple beneficial effects in the PD condition and I want to mention one more beneficial aspect of melatonin.
More recent studies are showing that melatonin also has positive effects on the gut microbiome and melatonin production in the gut is at least 400% higher than in the pineal gland, illustrating that melatonin has an important role in the gut.
Interestingly, at any time of the day or night, the gut contains at least 400 times more melatonin than the pineal gland, once again emphasizing the functional importance of melatonin in the gut. No photoperiodic cyclical secretion of melatonin was observed in the gut, which is in contrast to the typical secretion pattern for melatonin from the pineal gland.
Mannitol is noted for having symptom relieving qualities in some PwP. It has also been shown that mannitol can increase butyrate production. Butyrate is shown in rat studies to increase gut mucosal melatonin levels to control levels via its positive interaction with the gut microbiota.
>>> ' Melatonin was demonstrated to improve the oxidative stress resistance of mice with colitis and regulate the intestinal microbial flora, thus improving intestinal health. '<<<
More and more studies are showing how strong the gut microbiota is in having a positive or negative impact in PwP. Newer melatonin studies are showing how melatonin has a positive effect on the gut micro flora. Unfortunately, studies also confirm that melatonin levels decline with age, but fortunately, studies also show that butyrate and melatonin supplementation can increase melatonin in the gut to improve the gut bacterial balance.
This is just one more benefit that shows melatonin may be helpful in the fight against PD.
In my opinion it's too low of a dose. He has only scratched the surface in his melatonin research, but as he delves deeper, he will see how important melatonin is in PD and many other diseases at the right dose.
Human studies show that melatonin just starts to show benefit in PwP at 10 mg.
>>> ' Overall, melatonin supplementation for 12 weeks to patients with PD had favorable effects on the UPDRS part I score, PSQI, BDI, BAI, hs-CRP, TAC, GSH, insulin levels, HOMA-IR, total-, LDL-cholesterol, and gene expression of TNF-α, PPAR-γ and LDLR, but did not affect other metabolic profiles.'<<<
At 50 mg dosing melatonin barely starts to show modest improvement in motor symptoms during off times in PwP.
>>> ' The motor activity of the patients in OFF showed a tendency for a lower score with MEL than placebo (d = 0.43) Table 4. ' <<<
Both doses are too low to see exactly what melatonin can do for PwP.
By contrast, look at this study of melatonin in diabetic patients at 250 mg/day that showed improvements in just 8 weeks that reduced aspects of the disease that are likely to significantly improve the disease itself.
>>> ' It is concluded that melatonin supplementation may be effective in controlling arterial blood pressure including SBP, MAP, and PP and improving the anthropometric indices in T2DM patients. ' <<<
To give a clear example of why his dose is useless for anything other than possibly sleep, here is another diabetes study that used 6 mg in diabetes patients :
>>> ' During an eight-week RCT among patients with T2D, it was observed that adding 6 mg/day nightly melatonin to the background pharmacological management of patients did not have any favorable impact on HbA1c, FBG, insulin resistance/sensitivity indices, beta cell function, and hs-CRP levels. Actually, compared to the placebo group, in melatonin users, HOMA1-IR and HOMA1-S tended to be unfavorable at the end of follow-up. ' <<<
If he continues to research melatonin, these points should become clear to him and then he can consider increasing his melatonin dose to a more effective dose as used in the first diabetic study.
You're welcome, Farooqji. I have a question for you. Was what I said clear to you and understandable?The main thing I was trying to do was show how correct dosing determines the benefit of melatonin in people.
Yes, it's simple and straightforward. Self explanatory and supported by scientific studies. I was wondering if it is such an effective remedy, why it is not trialed at large scale yet (just like coq10). Have you come across any PD patient who takes it in such a large dose and benefitted from it (I haven't read any anecdotal evidence on this forum at least).
There are three people on this forum who have mentioned taking it, one at 60 mg/day and one at 70 mg/day (Sapeye), and one at 80 mg/day who claimed it kept his symptoms away, but then never reported back to say any more. Sapeye has noticed benefit in other areas, but as far as I know, not in PD symptoms, 70 mg is still too low. I use 106 mg/night for 8 months now, but do not have PD, so is of no value in the context of PD. The diabetes study used 250 mg/day and they saw significant benefit, but that was a short study and likely would have shown more benefit over time.
Yes, the studies indicate melatonin should be useful for multiple aspects of PD, a high dose study is needed for a significant period of time. Based on all of the studies, I would expect the right dose of melatonin to stop progression, but even if you just stop progression, the most you might expect is that tomorrow, you will be the same as today and next year, you will still be the same as today and 5 years from now you will be the same as today with adjustment for natural aging, but melatonin, based on studies may even help with that.
Based on studies though, melatonin should also help with the repair process, in which case you should also improve, not just stop progression.
As to why aren't more people testing melatonin, they might if a high dose study like the diabetes study shows benefit. The 10 mg/day melatonin study already showed significant benefit, but those benefits are not readily apparent to a PwP, even though beneficial things are happening in the body.
After reading the following article, it is hard to imagine me not taking melatonin for the rest of my life! When it comes to PD and melatonin, it all adds more clarity of why melatonin is useful in many ways for PD. This is a very comprehensive article on the effects of melatonin in neurodegeneration and more than I have previously seen in one article and it covers much of everything that is known about melatonin in relation to neurodegeneration. Obviously, to cover as much ground as the author is covering, it is very long, but that speaks directly to amount of effects that melatonin has in animals and humans and is to be expected.
This article begs the question, why isn't melatonin study part of the required curriculum for doctors of all types, but especially neurologists and movement disorder specialists? There are clearly many reasons why the body makes melatonin and has melatonin receptors throughout and this article is only mainly covering those aspects of melatonin relating to neurodegeneration, but melatonin does much more than that!
I sometimes here on this forum, complaints regarding back issues related to the spine and Intervertebral disc degeneration (IDD) resulting in significant pain and reduced mobility. In this new study (June/2021) it is suggested that melatonin may have usefulness in this area. Here is a link to the brief abstract :
Intervertebral disc degeneration (IDD) is a common degenerative disease of the musculoskeletal system that develops with age. It is regarded as the main cause of chronic low back pain in the elderly. IDD has various causes, including ageing, mechanical overloading, and nutritional deficiency. Melatonin is a pleiotropic indole hormone secreted by the pineal gland and plays an important role in resisting various degenerative diseases. The serum levels of melatonin decline with age and are reported to be negatively correlated with the symptomatic and histopathological scores of IDD. In vivo studies have shown that exogenous administration of melatonin could maintain the structural integrity of the intervertebral disc and inhibit the development of IDD. Mechanistically, by interacting with its membrane or intracellular receptors, melatonin can promote autophagic flux, scavenge free radicals, inhibit the release of pro-inflammatory factors, and block apoptotic pathways, thereby enhancing anti-stress abilities and matrix anabolism in different types of disc cells. Therefore, melatonin supplementation may be a promising therapeutic strategy for IDD. This review aimed to summarize the latest findings regarding the therapeutic potential of melatonin in IDD.
I wrote about this and explained what these type of studies are missing and why they came to the wrong conclusions. If you notice this study is not supplementing melatonin, but rather measuring existing blood levels and I have previously explained why this is completely different from when you look at studies where melatonin is actually supplemented. It is already well established that melatonin levels decline with age. I copied and am pasting what I have previously written on this subject over a year ago because I thought the same thing:
>>> chartist
1 year ago
I'm pointing out a study from last year that discusses the relationship of glutathione, melatonin and PD. The reason I am pointing this study out is because the study by itself might give the impression that melatonin is not good for PD, but what this study may actually be showing is that melatonin is elevated in PD because more melatonin is needed as the body tries to compensate by increasing melatonin production as the glutathione level drops well below normal.
They didn't use melatonin in this study, just measured native levels of melatonin and glutathione. Now with the arrival of the new 10 mg study, it appears that the reason that glutathione is low in PD is because it is being used up so fast because of the elevated oxidative stress levels associated with PD and the melatonin production is increasing as the bodies way of trying to compensate for the declining glutathione by increasing production of melatonin within the limitations of the body and this increased melatonin production is insufficient to boost the glutathione high enough to offset the high burn rate of glutathione in PD. The new study shows how supplementing just 10 mg/night of melatonin is able to reverse the negative correlation between melatonin and glutathione shown in the older study. In the 10 mg study, melatonin raises the blood level of melatonin and also shows that this increase in melatonin results in an increase in glutathione or essentially the opposite of what the older study shows. Context is important!
Keep in mind that in the PD/Melatonin 10 mg /day study , the addition of melatonin increased the total glutathione level and the melatonin level as is reflected in many other studies where they actually supplement melatonin as opposed to just analyzing native levels. I think the newer study puts the older study into proper perspective and just begins to shed light on the value of melatonin in PD treatment. Melatonin also improved non motor symptoms in the 10 mg study.
The older study is one reason why I never really tried to discuss melatonin as it relates to PD, but now I think I have a better understanding of that study and what it is really showing.
Some important points we don't know from this newer 10 mg study is what would the numbers look like had the study gone for an additional 12 weeks? Would the improvement have continued upward? What would the results have looked like at 50, 100 or 180 mg/day instead of 10 mg/day?
Dr. Reiter and Dr. Shallenberger are both using 180 mg /night and Dr. Reiter has been doing that for over 25 years so clearly he believes in the value of melatonin for humans. <<<
I wrote this over a year ago but you can see that comparing native melatonin levels in PwP is absolutely not the same as looking at response to melatonin supplementation. The 50 mg study in PwP did not delve into this aspect, so I did not use it for comparison, but it did show that at 50 mg melatonin barely started to show motor symptom improvement during "off time".
Context can be important! I hope this answers your question.
Melatonin supplementation and the effects on clinical and metabolic status in Parkinson's disease: A randomized, double-blind, placebo-controlled trial
Found this other article sites yours: It seems you are right on track Art!
2021 Apr 15
Melatonin as a Chronobiotic and Cytoprotective Agent in Parkinson's Disease
Indeed, RBD patients may evolve to an α-synucleinopathy within 10 years of RBD onset. Daily bedtime administration of 3-12 mg of melatonin has been demonstrated effective in RDB treatment and may halt neurodegeneration to PD. In studies on animal models of PD melatonin was effective to curtail symptomatology in doses that allometrically projected to humans were in the 40-100 mg/day range, rarely employed clinically.
Even in animals it shows exactly the same that higher native levels correlate with worse disease condition, but when they actually give animals melatonin they improve.
Interesting info. I'm hypothyroid so this may be bad news for me (or not).
22 September 2018
6 MELATONIN AND INFLAMMATION IN NEURODEGENERATIVE DISEASES
Low-grade brain inflammation, which is already developing in the course of normal aging, is further aggravated in neurodegenerative diseases.16 This is particularly evident in the most severe forms of dementias such as Alzheimer's disease (AD). Nevertheless, neuroinflammation is also a characteristic of other diseases of entirely different etiologies, such as Huntington’ disease, Parkinson's disease, amyotrophic lateral sclerosis, spinocerebellar ataxia, and multiple sclerosis.144 Inflammation leads necessarily to oxidative stress and, under conditions of strongly elevated NO levels, to nitrosative/nitrative stress, too. However, oxidative stress, especially when caused by mitochondrial malfunction, can also induce inflammatory responses. The pivotal role of oxidative stress in these pathologies has been recently reviewed.145 Melatonin is a broad-spectrum antioxidant that acts by various mechanisms that comprise direct and indirect detoxification of free radicals, mitochondrial protection, reduction of free radical formation by inhibiting electron leakage and NADPH oxidases, prevention of neuronal overexcitation and several anti-inflammatory actions.2, 14, 16, 80, 82, 146, 147 From this point of view, melatonin can be assumed to counteract inflammation by reducing both possible causes of oxidative stress and proinflammatory signaling. In fact, several encouraging findings have been obtained by using melatonin in various neurological disorders, however, not yet on a sufficiently broad basis that would justify a more general clinical application.148 Moreover, it seems important to avoid inappropriate generalizations. The existence of antioxidant and anti-inflammatory actions does not exclude additional undesired effects of melatonin in certain neuropathologies. In the case of multiple sclerosis, the autoimmune etiology has to be taken into consideration. As melatonin can also display proinflammatory properties, for example, in arthritis,121-123 caution is due in all autoimmune diseases. In the case of Parkinson's disease (PD), numerous preclinical findings have indicated a beneficial role of melatonin,149-151 however, mainly in models based on mitochondrial dysfunction in the nigrostriatum and mostly without considering the early pre-motor symptoms that reflect the initial stages of the disease. Moreover, several findings have remained contradictory.13, 152 Melatonin had been even regarded as a detrimental factor in PD and treatment with melatonergic antagonists had been reported to be beneficial.153, 154
Materials and methods: In study were taken 51 patients from 25 to 63 years to manifest hypothyroidism (on a background of autoimmune thyroiditis), with anxiety-depressive syndrome and sleep disturbance. Thyroid hormones were determined by ELISA (Vector-Best Russia) Anxiety-depressive syndrome in patients with hypothyroidism were analyzed on hospital Anxiety and Depression Scale HADS. Patients were divided into 2 groups. First group with manifest hypothyroidism (25 patients) received standard replacement therapy with L-thyroxine and symptomatic therapy for 1 month. Second group with manifest hypothyroidism (26 patients) along with L-thyroxine and symptomatic therapy additionally received melatonin (15 mg/night)
Conclusion: The inclusion of melatonin in the standard therapy for symptomatic hypothyroidism showed that the drug can affect the pituitary–thyroid system, removing anxiety and depression.
I'm trying medium dose (106+ mg/day), but not so much for neuroprotection as heart, cardiovascular, stroke, eyes, diabetes, cholesterol, triglycerides, psoriasis and lung protection and any other protections that dose may offer including neuroprotection.
I take 10 mg and have trouble getting out of bed in the morning.
I think one of those studies said if you take the melatonin as a suppository it does not cause drowsiness. I wonder if a regular capsule can be used as a suppository? I read that the rectum is the place where it is best absorbed.
I've been at 106 or more milligrams of melatonin for over 8 months now and I feel about as what I know as normal. On the nights I have gone above 106 mg, I can get the melatonin hangover the next day, but not always. As long as I stay at any consistent dose, my body seems to adjust and then the hangover goes away. When I stay busy, any melatonin hangover is nil or very little.
Yes, at least one study indicated that next day drowsiness was not a reported side effect when using melatonin in suppository form at high dose. The same was reported for injected dosing in at least one study.
I went from taking 30+ mg/night for a long time and then went almost straight up to 80 mg for a brief period and then up to 106+ mg for over 8 months now. Years ago I did 70 mg/day for 9 months to try and replicate a study dose regimen of melatonin. While at 106 mg, I briefly went up to 180 mg/day, the dose that Dr. Shallenberger said he suggests to all of his patients. He also gives his stage 4 cancer patients up to 360 mg/day around the clock.
You're preaching to the choir. Dr. Reiter is a world renowned authority on melatonin and melatonin research. Look at the number of studies he has either headed or been a part of on PubMed!
Watched the Dr Shallenberger video and get the idea that it is not really good for you to take melatonin during the day. Says he only has his sickest patients take it during the day.
I was hoping I could start taking most of mine during the day and avoid the morning grogginess.
Any thoughts on daytime consumption of melatonin? I'm thinking I could take 10 mg twice a day during the day.
I don't take melatonin during the day. I think that should be reserved for serious illness such as stage 4 cancer that he mentioned or something fast moving and devastating like ALS. I did take it during the day when I thought I might have Covid-19.
Now you are starting to really get an idea of why I like melatonin so much and are starting to get a glimpse of what melatonin can offer to human and animal health!
Hello Art ~ Thank you for all of this fabulous research and information!! I feel like I have a direction to move toward. My husband has been taking 10 mg of Melatonin for just over a month now, having slowly worked up to that amount over a few weeks and without any discomfort/grogginess. He seems to have hit a plateau with his symptoms. I think I will start increasing his Melatonin slowly and see where we go. Today he just started the Dual Coronet Infrared Light hat thing. I probably should wait on one or the other so I would know exactly what we are getting a benefit from ~ but I can't. I just can't handle seeing him so miserable when his tremor ramps up and causes such anxiety. So ~ here we go!!
Again thank you for all or your incredible research, knowledge and time!!!
Normally I would agree that starting more than one remedy at a time is not the best way to go, however, this particular situation might be an exception.
One Photobiomodulation (PBM) study showed that PBM increases oxidative stress as part of its working process and melatonin is the most potent antioxidant and radical scavenger in the body and is also able to cross the blood brain barrier (BBB) as would be needed in order to target the area being directly treated by the red light therapy as applied by the Dual Coronet.
Imo, these two are likely to be complementary to each other with the melatonin potentially negating the increased oxidative stress generated by the regular use of the Coronet and the Coronet acting in synergy with the known brain health benefits of melatonin. With melatonin inhibiting the oxidative stress that PBM can produce, the PBM is likely to work more optimally.
If I may suggest, taking notes is likely to be helpful and also taking videos similar to what Dr. Costantini asked his HDT/B1 patients to take before therapy and during therapy at regular intervals. Longer videos seem likely to make it easier for the untrained eye to determine beneficial changes in symptoms. The reason for this is because many of his patients who were slow responders to HDT, believed that they had not improved at all, but once he played back their videos of before they started HDT, the improvements were obvious. Without those videos, people might just discontinue treatment thinking that they are non responders to HDT.
PBM, from what I have seen so far is a slow process that takes months of regular use in order to see discernible improvement and when it takes months, similarly to B1 slow responders, it is often easy to forget exactly how bad you were before treatment and videos are a means to provide evidence of exactly how you were compared to your current state.
Good luck on this journey with your husband and please keep us updated on how it goes for the both of you!
Thank you Art for the encouragement and, again, more information! I am kind of on this journey alone without medical support at the moment. We have an appointment with a "new to us" neurologist, but not till October so I do rely on this forum for information and direction.
I will try to do the videos. Documenting by video is kind of a difficult thing for me to do since his symptoms aren't hugely noticeable. I can usually tell when's feeling awful just by looking at him but not always (he's not a complainer). Most people don't know he has anything wrong other than just being old. He has told me more than once that he always feels like something isn't "right". He NEVER has times of feeling good or normal so that is why I am on this mission to find him some relief. I try not to read about prognosis/progression. I only read about what might be or is helpful in stopping symptoms and progression. I will say he is much better than when we first got the diagnosis in December and unfortunately I don't know which of the many things we are doing has been of benefit, but I'm ok with that.
Again, thank you for the encouragement, information, and your time! I will update as time continues to march on!
Have a fabulous weekend!! gail
(By the way as a side note ~ When we had prostate cancer 11 years ago I knew more about diet and supplements than our oncologist. And this past March we both got Covid and I had it worse than he did! He barely had symptoms! And we both came out of it without too much of a problem.)
>>> ' I can usually tell when's feeling awful just by looking at him but not always (he's not a complainer). ' <<<
Whatever it is you are seeing in these instances, you should try and capture that on video also. If your treatment plan is working, these episodes should start to decrease in intensity and frequency.
On a somewhat related note, if he likes pistachios, this will likely make a very good and healthful snack for him that has shown the ability to alter the gut microbiome in a positive way. If he is taking mannitol as part of his treatment plan, even more reason to give him pistachios very frequently!
I believe that thiamine is likely to be helpful because of its antiinflammatory properties and track record and in combination with other things like melatonin, pistachios, mannitol and PBM therapy could be quite useful, but if you do them all at once, it may be impossible to tell which is most beneficial.
So where to you come down on mannitol? I'm probably a bit too rule oriented, and mannitol is on the "No" list for the SCD so I ruled it out of my treatment plan. Mannitol works as a diet sugar substitute because it is not easily digested, which exactly what SCD avoids. Your body does not digest the mannitol, but the bad bacteria does
Yes, we are on two different roads trying to get to the same place and as such we will deal with multiple different milestones along the way. I think that mannitol is possibly not digested exactly as you said , but rather it is fermented in the small intestine in the presence of SCFA producing bacteria (provided by the pistachios) that together could result in the production of short chain fatty acids which include acetate, propionate and butyrate which are all deficient in PwP, especially propionate. The addition of propionate in PD mice models has shown the ability to recover some lost motor function activity. Ultimately, I do not want to easily discount mannitol which has already shown benefit in some PwP in terms of symptom reduction, on the contrary, I would want to include something that has already shown such benefit in PwPs.
You are currently incorporating the SCD, melatonin and B1 on your road, whereas I am looking at all things to improve the gut microbiome and mannitol being a prebiotic will attempt to feed the healthy bacteria in the gut and in conjunction with pistachios which increases butyrate producing bacteria in the gut, which is depleted in PwP as is butyrate, which has shown the potential to heal leaky gut. So these two together are likely to increase butyrate production which can heal the leaky gut and lower inflammatory levels with the potential to reduce symptoms and increase hydrogen sulfide production which will add potency to the antiinflammatory activities. Butyrate will also have histone deacetylase inhibiting activities (HDACi) which should be neuroprotective. All beneficial actions for PwP and the gut microbiome.
I think thiamine which is naturally produced in the healthy gut, may be insufficiently produced in the perturbed gut of PwP where it can be transferred to the brain through at least two pathways as well as other areas of the body where it is needed to improve many bodily functions. So adding HDT may be useful in order to allow more B1 to reach the brain where it is anti neuroinflammatory.
Regular thiamine testing does not show the amount of thiamine in the brain or other tissues. Again, I want to include things that have already shown symptom improvements in PwP, so B1 is definitely on my list as is melatonin based on the 10 mg melatonin study in PwP. Melatonin has also shown the ability to promote the mucosal barrier repair in the gut while offering antiinflammatory effects there as well as potent antioxidant and radical scavenging activities . Melatonin is naturally produced in the gut in much much larger quantity than by the pineal gland and melatonin produced in the gut does not cause the melatonin hangover. The estimated production of melatonin in the gut is said to be 500 to 1,000 times that of the pineal gland production of melatonin! That right there tells you that melatonin plays an important role in the gut microbiome.
Dang you are good Art! I like that. Pistachios plus mannitol. I am definitely up for pistachios. I will probably get to the mannitol. Added 200 mcg selenium today (mostly for my HT, but I think dealing with HT will help with my REMSBD. Adding Lions Mane tomorrow and inositol Tue (goes will with selenium for for HT).
One possible way to get higher melatonin dosing and avoid the next day tiredness or "melatonin hangover" is by eating large amounts of pistachios! As I wrote about the value of pistachios earlier today, these are a very healthy snack food for people in general and PwP in particular because they have positive effects effects on the gut microbiome, increase bacteria in the gut that produce short chain fatty acids (SCFAs) including butyrate, acetate and propionate and also increase all three of these which are important in PwP. The increase in butyrate producing bacteria is likely to be helpful for anyone taking mannitol or planning to take mannitol as mannitol interacts with these bacteria to produce even more butyrate.
Here is a very lengthy article on the melatonin content of many different foods and you will have to scroll down to "Pistachios " to see the content which is quite high compared to other foods :
Clearly you can not get anywhere near the dose of melatonin that I am taking by eating pistachios, but for those who are subject to the melatonin hangover with very small dosing of melatonin, this may be a possible solution. I think the most important aspects of pistachios is the increased fiber, increased SCFAs including increased butyrate producing bacteria and its ability to improve the gut microbiome balance. It seems likely to work well with Mannitol because the PwP gut is deficient in SCFAs as well as SCFA producing bacteria.
This is a high fiber food that I can eat, but actually enjoy the taste of!
Very interesting Art! I will put a dose of pistachios in my daily diet, I like them a lot too. I use to eat walnuts for breakfast because they contain a lot of zinc and other minerals, this brand of walnuts in Italy is very good and fresh which makes the difference in effectiveness. Minerals are very important and it is difficult to find a supplement that works so I solve with lots of fresh fruits and vegetables and nuts, now I'll add pistachios. There are a lot of fiber-based diets, very complicated but I like good things and pistachios and nuts will do just fine. Simple and good and effective, perfectly aligned with my philosophy: "make your life as beautiful and interesting as a work of art", (food and culinary art context)). Thank you Art.
photo: my breakfast this morning. my sister-in-law made the chocolate chip cookies, they are soft and very good. birch xylitol and walnuts. Coffee with milk. 😁
I like xylitol also and am currently using it along side two small cups of pistachios per day. Xylitol is similar to mannitol in terms of increased butyrate production. I believe in terms of butyrate, walnuts may actually be better in terms of increased production, but pistachios I like and could eat them for the rest of my life. I have to go now and refill my pistachio cup!
Increased butyrate with xylitol. I had no idea. I think it was Dr. Mark Hyman that said it’s bad for the gut. But if it increases butyrate than he is wrong I think. Ghee is supposed to be good for butyrate production. (If I ask the same question as I previously have, I apologize. If I do this, I don’t mean to.). Have you heard of Immunocal? It is a supplement that is a glutathione precursor. I want to make it work but it’s hard to get down and I don’t know if it’s worth it?
I'll put it gently, he needs to review the evidence before making a statement like that.
Xylitol is a polyol as is mannitol and it has done wonders for gut issues I previously had. It also increases SCFAs of which one is butyrate and another is propionate and the other is acetate and all three are deficient in PwP, especially propionate. In PD mouse model studies propionate partially restored some motor function.
Propionate and butyrate both help repair and maintain the gut barrier function and the butyrate is known to reduce inflammation in the gut and brain and promotes a healthier gut microbiome.
If you tolerate melatonin, it increases glutathione and increases gene expression of many of the bodies own potent antioxidants such as Catalase, Glutathione, Glutathione Peroxidase, Superoxide Dismutase to name a few. It is a more potent antioxidant and radical scavenger than glutathione and it can neutralize at least 10 oxygen radicals while vitamin E or C can only neutralize one each. It readily crosses the Blood Brain Barrier (BBB) as well as all body tissues and it helps fight off osteoporosis, cardiovascular disease (CVD) and stroke, all of which PwP are at higher risk to get. Melatonin help repair the gut, modulate inflammation and oxidative stress in both the gut and brain, while protecting the mitochondria and dopaminergic neurons. It also fights cancer from 8 different pathways as Dr. Shallenberger has discussed at length. I can go on quite awhile, but do I need to? Melatonin is a much more potent antioxidant than glutathione.
Or you can force down the Immunocal and potentially get some more glutathione.
If they fit in your diet, don't forget the pistachios! They are useful all on their own, but probably better with xylitol or mannitol because the pistachios increase butyrate producing bacteria in the gut and both mannitol and xylitol interact with those bacteria to increase butyrate. PwP are lacking in the short chain fatty acids like butyrate, propionate and acetate.
Hi Art ~ Thank you for the guidance of what to video. Obviously I was at a loss as to what to video. The only videos I saw were the ones Dr. Constantini had of people walking and doing the push test and my husband walks just fine and has good balance. So thank you very much!!!I haven’t checked into mannitol yet. I will move it to the top of my list of “check this out”. And I will definitely go through the link you sent.
As far as gut ~ I feel like he’s in really good shape. For several years we’ve been taking Kombucha with Fire Cider mixed in it (yuck!!). A while back we started adding a fermented cabbage mix. Most recently I added 3Tbs of flax seeds mixed with MCT oil. He has no problems with constipation at all. But, I will definitely add pistachios to his diet. He’ll be excited about that!!
Thank you sooooo much for all your wonderful help and information and time! This is such new territory for me to be investigating and I know so little!!
Once you read the FMT post I put up a couple of weeks ago, if you haven't already, the importance of the gut microbiome balance in PD and many other diseases becomes much clearer. No other adjuvant treatment for PD seems to be able to do as much as making the gut microbiome similar to non PD healthy people.
Melatonin is a natural hormone mainly secreted by the pineal gland that regulates different physiological functions. Melatonin is also synthesized by other organisms, such as bacteria, invertebrate animals, and plants [118]. The consumption of foods rich in melatonin such as pineapple, orange, and banana, can increase the antioxidant capacity of the organism [119]. Melatonin has also been identified in vegetables, meats, and sprouts [120, 121]. Meng et al. evaluated that eggs, fish, nuts, cereals, and some seeds are the foods with the highest melatonin content [122]. Melatonin is known for its antioxidant properties and anti-inflammatory and cardiovascular effects. Melatonin has properties that inhibit tumor proliferation in the autoimmune system and provide a neuroprotective effect [123–127]. The main interest in the investigation of the effects of melatonin on PD arises from the relationship between the decrease in the activity of the pineal gland and melatonin in these patients [128]. MT1 and MT2 melatonin receptors are also decreased in PD [129]. Melatonin neutralizes ROS and induces the expression and activity of antioxidant enzymes [130, 131]. In mice, the effect of melatonin counteracts the progression of dopamine by increasing the activity of the mitochondrial complex I by decreasing the levels of lipoperoxides and nitrites in the cytosol and mitochondria of brain cells [132]. Other studies have shown antiapoptotic, neuroprotective, and antidepressant activity in mouse models with PD [133–135]. Other studies have shown that melatonin treatment can help improve sleep disorder and increase neuroprotection in PD patients [136, 137]. However, the consumption of melatonin has not been able to improve the motor symptoms of PD [138]. Some studies reported that melatonin could promote ROS generation. In vitro studies showed that melatonin has prooxidant effects mainly at lipids and proteins [139]. However, high concentrations of melatonin (10-1000 μM) are reported to promote ROS production by inducing cytotoxicity and apoptosis in human leukemia cells [140]. Similar effects were found in an Alzheimer's disease model culture, where melatonin concentrations of 1 mM increased oxidative stress markers, while concentrations < 0.1 mM reduced oxidative damage [141]. The prooxidant mechanisms of melatonin have not been fully described. Leukocyte studies show that melatonin has little interaction affinity for calmodulin and that this phenomenon seems to favor ROS production [142]. The benefits and risks of melatonin supplementation in PD patients require more clinical evidence to support the previously described findings.
I think these parts about melatonin increasing oxidative stress markers is concerning me. However, high concentrations of melatonin (10-1000 μM) are reported to promote ROS production by inducing cytotoxicity and apoptosis in human leukemia cells [140].
When you are aware of the potent anticancer effects of melatonin, generating ROS in leukemia cells might not only be expected, but highly desirable. Many normal things that the body goes through generate ROS and oxidative stress, such as walking, exercising and yes, even breathing! That is what the human antioxidant and radical scavenging system are in place for to, scavenge these radicals and neutralize oxidants either directly or indirectly and melatonin is the most potent antioxidant in the human system.
These other studies that they refer to in their review are pretty ridiculous. Look at Table 1 and right below melatonin they list vitamins. Look at what they say about vitamin C :
>>> ' Vitamin C can induce OS in the presence of free transition metals and H2O2 [156] '<<<
How about the fact that free transitions metals and H2O2 can generate oxidative stress whether vitamin C is there or not, but vitamin c will try to quench it if it is there.
Whereas you look at the 10 mg melatonin/PwP study and somehow, increased melatonin caused increased levels of glutathione. Don't you think that if melatonin is such a huge generator of oxidative stress, that the already low levels of glutathione in PwP would be even further depleted by melatonin and the patient would worsen and not improve if the review was right?
You are so spot on Art. I get rattled sometimes, but the studies are there.
Speaking of vitamin C. I had heard ascorbic acid is industrial waste and you should only buy whole food vitamin C. Whole Food Vitamin C has copper! Any thoughts on the best vitamin C?
In this study they gave the rats Berberine intraperitoneally and this increased cytotoxicity in the rats and it decreased dopamine levels and caused the DA neurons to degenerate. All that and yet Berberine is noted for increasing production of Levodopa in the gut and then transporting the levodopa to the brain to be converted to Dopamine and thus improving motor symptoms. This is bad research by the review team that wrote this review.
The article was written in 2010 and their review was listed in 2020. Obviously in 2010, they did not know the method of action of Berberine, but in 2019, they had a better understanding of how Berberine works to help in PD which the review team should have checked on to understand why the study results were so contrary to newer study results using Berberine in PwP. In the 2010 study, the researchers did not realize that the benefit of Berberine actually begins in the gut and not the brain and since they delivered the berberine intraperitoneally (via injection directly into the peritoneal cavity, the berberine essentially bypassed the gut and not only lost all benefit but caused degeneration. The review team should have reviewed that study more thoroughly and realized the error. I'm going to give "the review" a bad review!
Great point Art. It also relates to something I have noticed, in that people poo poo PK treatments that can't pass the BBB, when maybe the brain should not be the target anyway.
Now I just need to figure out what high concentrations of melatonin (10-1000 μM) means. μM is a micro mol, but this is saying a concentration, not a specific amount of melatonin.
I know, it is easy to underestimate the importance of the circadian rhythm, but imo, that could be a mistake to do so. This is why I was thinking ALCAR for the daytime help out or possibly Bioperine since it may help alleviate the melatonin hangover if taken near wake up time.
>>> ' Conclusion: Due to its highly lipophilic and small size properties, melatonin accesses all intracellular organs by easily passing via the cell membrane and prevents protein, DNA damage, and lipid peroxidation. In particular, melatonin, by protecting and reducing oxidative stress in mitochondria, can normalize homeostasis and mitochondrial function and ultimately prevent apoptosis and cell death. ' <<<
In PwP, it is established that insulin resistance is common and effectively promotes the disease process through multiple methods such as mitochondrial dysfunction, abnormal alpha synuclein production and enhanced degeneration of dopaminergic neurons to name only a few.
As melatonin studies evolve, it becomes more clear that when you think of specific issues seen in PD, melatonin often times seems to ameliorate that problem. There is a reason that melatonin and its receptors are made in the brain, in the gut and in every mitochondria to name only a few places of melatonin production and utilization in the body. Melatonin is absolutely essential for human health, animal health and plant health. The body starts making melatonin and its receptors from the time we are born and it is for far greater reasons than sleep.
Unfortunately melatonin production declines with age, with age 50 years appearing to be a critical juncture where age related diseases like PD increase while melatonin production has declined very significantly to the level of a newborn. It certainly begs the question, what would happen if the melatonin level in humans was maintained at the level of a seven year old for the rest of your life?
In this 2021 study the discussion is about problems with DNA damage repair in PD and how science is looking into this as another potential target in PD.
Here is another double-blind, cross-over, placebo-controlled randomized clinical trial study conducted in 26 patients who received either 25 mg of melatonin or placebo at noon and 25 mg, 30 min before bedtime for three months. It is worth mentioning that this is the same group who did a melatonin/PwP study in July 2020 that also used 50 mg of melatonin per day in PwP and found positive results. Here is a link to that 2020 study:
In this latest study, they were measuring other parameters related to oxidative stress and mitochondria functionality. Again, they showed positive results in the treatment group after 3 months of treatment that was significantly better than the placebo group. Here is a link to this new study :
>>> ' At the end of the trial, in patients who received melatonin, we detected a significant diminution of lipoperoxides, nitric oxide metabolites, and carbonyl groups in plasma samples from PD patients compared with the placebo group. Conversely, catalase activity was increased significantly in comparison with the placebo group. Compared with the placebo group, the melatonin group showed significant increases of mitochondrial complex 1 activity and respiratory control ratio. ' <<<
>>> ' In conclusion, melatonin administration was effective in reducing the levels of oxidative stress markers and restoring the rate of complex I activity and respiratory control ratio without modifying membrane fluidity. This suggests that melatonin could play a role in the treatment of PD. ' <<<
>>> ' Taken together, our data showed that melatonin supplementation recovers mitochondrial function and diminishes oxidative stress. Thus, this indolamine could play a role as an adjuvant in the treatment of PD. ' <<<
To get a better idea of how well melatonin reduced the representative markers of oxidative stress, you will have look at the included graphs and charts, but it is safe to say that melatonin at 50 mg/day significantly lowered these markers.
Higher dose melatonin studies are still needed in order to clarify just how much melatonin can do in PwP.
Melatonin and its metabolites not only cross the blood brain Barrier (BBB) to exert its potent antioxidant and anti inflammatory effects in the brain to reduce neuroinflammation and damaging oxidative stress, but it protects the BBB integrity and improves the barrier against permeability :
This is important because neuroinflammation can damage the BBB, neurons, glia and mitochondria. If the underlying neuroinflammation and damaging oxidative stress and nitrosative stress is not controlled, damage to the blood brain barrier will continue as will damage to neurons and mitochondria, so all three things are needed, protection of the BBB, reduction of neuroinflammation and control of oxidative and nitrosative stress closer to normal healthy control levels. Melatonin and its metabolites appear to meet these criteria.
>>> ' N-acetyl-5-methoxytryptamine (melatonin), was discovered as a potent antioxidant in 1993 [236]. Since then, melatonin’s ability to protect all cells and organs from oxidative/nitrosative damage has been confirmed in more than a thousand publications [17, 79, 128, 178, 197]. The indoleamine melatonin is produced in all animals from unicells to humans [71, 91, 92, 141, 248, 259] and also in plants [14, 60, 94, 142, 159, 162, 172, 195, 240, 241] ' <<<
Here is some updated information on how melatonin works against PD. It does more than what is mentioned below, but these are clearly important in PwP.
Melatonin has shown the ability in PD models to reverse the disease to varying degrees in most of these models, it has an excellent safety profile, it is produced in every cell in the body, it activates Nrf2, it increases TAC which is depleted in PwP, it protects all mitochondria as it is naturally produced there to almost instantaneously neutralize ROS as it is produced in the mitochondria, it protects DA neurons until it no longer can as melatonin and its receptors become depleted in the Substantia Nigra pars compacta, it protects the gut biome and assists in preventing dysbiosis along with gut permeability including the associated inflammation and oxidative stress until it no longer can fully protect it due to the age related decline of melatonin, it protects the heart and cardiovascular system which are at increased risk for damage due at least partially to the chronic low grade inflammation as well as the elevated levels of oxidative stress.
Melatonin has reduced the elevated oxidatative stress levels seen in PwP back toward healthy control levels in 3 months, It decreases NF kappa B, IL-17, IL-8, IL-6 and TNF-alpha to reduce other inflammatory mediators in the inflammatory cascade, it increase many of the bodies natural antioxidants at the gene level, freely crosses the BBB, but its metabolites also repair the BBB to further protect the brain against neuroinflammation, it helps neutralize Covid-19 which in some PwP has caused exacerbated symptoms, it helps ameliorate the oxidative stress caused by C/L, it helps to maintain gut biome homeostasis which is where, a growing number of researchers feel the disease process may begin.
It assists in the protection of the organs of the body including the skin and eyes, it has already shown benefit in PwP at 10 and 50 mg/day dosing, it improves PD perturbed sleep patterns in some PwP, it is considered useful for RBD which is often seen before the onset of PD, melatonin can up regulate or down regulate excessive Mitophagy, melatonin can also increase or decrease Autophagy, it helps prevent a-syn agglomeration and reduces a-syn levels, melatonin itself has at least 10 metabolites which can also act as potent antioxidants and radical scavengers, melatonin reduces Homocysteine levels which is elevated in PD at least partially because C/L increases Homocysteine levels and oxidative stress in PwP.
Melatonin increases SCFA production in the gut, another way that melatonin down regulates neuroinflammation in PD is by down regulating Inflammasome NLRP3 which is up regulated in PD and Covid-19. SIRT1 ameliorates oxidative stress induced neural cell death and is down-regulated in both PD and AD and melatonin up regulated SIRT1. Melatonin has shown improvement in PwP with nocturia.
Here is a new (May 2022) study in just 12 PwP showing marginal benefit from very low dose melatonin (2 mg prolonged release melatonin/night) for PD, but I don't get the point of doing a 2 mg study when there is already a 10 mg and two 50 mg studies for melatonin in PD? How about a 250 mg/day study as has already been done in diabetics to good cardiovascular effect. Did they think that a 2 mg dose was some how going to be better than 10 mg or 50 mg? They did use prolonged release melatonin which is different than the other 3 studies, but still rather frustrating and just 12 participants is not helpful either. I consider this a wasteful use of study resources!
>>> ' Sleep latency significantly decreased from T0 to T1, but no other significant differences were found in PSG parameters. Melatonin PR treatment significantly reduced the ESS scores from T0 to T1, while the PSQI scores presented a trend of improvement from T0 to T1. Motor dysfunction was not improved by melatonin PR, although there was a trend in decreasing UPDRS-III. Both clinical global improvement and patient clinical global impression documented an improvement in insomnia symptoms at T1. ' <<<
Honestly, any positive results at this low of a dose is a surprise, but still I consider it a waste of study resources!
Sorry, I did not read all. I'm sure all was worth-wild. It took years to develop PD. In old-age are we deficient, probably yes. My gut says our brains are deficient in B1.
This new (June 2022) systematic review discusses in detail how melatonin should be useful for neurodegenerative diseases and cardiovascular diseases and possibly other age related diseases. Dr. Reiter is a contributor to this review :
Here are some very relevant quotes from this review :
>>> ' Melatonin also prevents mitochondrial dysfunction and cellular aging by limiting the oxidation of cardiolipin, a phospholipid localized in the inner mitochondrial membrane. Cardiolipin plays a key role both in multiple mitochondrial bioenergetic mechanisms and in the stability and dynamics of the mitochondrial membrane, as well as in several apoptotic events that involve the mitochondria (Paradies et al., 2017; Figure 2). ' <<<
>>> ' Other mechanisms by melatonin which exerts anti-aging effects are the modulation of the sirtuin1 (a deacetylase that regulates metabolic activity in response to cellular stress) pathway and the modulation of autophagy, which is decreased during aging. Autophagy is a natural cellular homeostatic mechanism of removing damaged cells, in order to regenerate newer, healthier cells. ' <<<
>>> ' Together, melatonin and sirtuin 3 influences mitochondria dynamics and scavenges free radicals, thus preventing or delaying cellular aging and its derived diseases, which are usually developed as a consequence of a redox imbalance (Reiter et al., 2018). In fact, it was observed that the expression patterns of melatonin and different sirtuins (sirtuin 1,3, and 6) significantly decreased in samples of buccal epithelium from old patients compared to young patients, and even more evidently in those who suffer from hypertension. This finding reinforces the likely relationship between age-related diseases (such as hypertension) and melatonin levels (Carbone et al., 2020; Figure 2). ' <<<
>>> ' In addition to its action on sirtuins, melatonin may also upregulate Nrf2 (Nuclear factor erythroid 2-related factor 2), an antiinflammatory transcription factor) and downregulate NF-κB (a proinflammatory transcription factor) to attenuate inflammatory processes at the cellular level. Likewise, this indoleamine also stimulates the release of anti-inflammatory cytokines such as IL-4 and IL-10, as well as promoting the polarization of macrophages from a proinflammatory phenotype (M1 phenotype) to an anti-inflammatory phenotype (M2 phenotype). Additionally, melatonin suppresses other proinflammatory events, such as β- amyloid toxicity, NO release, cyclooxygenase-2, and NLRP3 inflammasome activation, TLR4, and mTOR signaling, and cytokine release by senescence-associated secretory phenotype, among others. Together, these actions significantly contribute to the anti-aging effect of exogenous melatonin, since aging and its related pathologies are usually associated with chronic proinflammatory processes, which are a consequence, at least in part, of reductions in endogenous melatonin secretion (Hardeland, 2019). ' <<<
>>> ' The clinical trials related to the potential therapeutic use of melatonin to alter aging processes in humans have not used especially high doses. The dose issue is generally considered to not be a major problem when melatonin is used because of its uncommonly low toxicity and its safety over a very large dose range. ' <<<
>>> ' The bulk of the melatonin produced in mammals is believed to be from the mitochondria of every cell, where its synthesis presumably occurs 24 h a day and is not impacted by the light/dark cycle (Suofu et al., 2017). Importantly, the availability of nano-encapsulated melatonin preparations which are available will likely become highly advantageous. Their regular use could well improve availability and sustain intracellular concentrations at a level where they would provide health advantages against aging-derived pathologies, including cardiovascular and neurodegenerative diseases (Sarkar et al., 2017; Martín Giménez et al., 2020; Chuffa et al., 2021). ' <<<
>>> ' We clearly observed that MLT significantly improved the motor functions and prevented DA neurons from loss. In addition, MLT ameliorated neuroinflammation by increasing the expressions of anti-inflammatory M2-like phenotypes in microglial cells. Further investigation in BV2 cells confirmed that RORα mediated the anti‐inflammatory effect of MLT. Moreover, this MLT‐RORα axis changed the phenotype of microglia via the STATs pathway. Taken together, our study introduced an essential nuclear receptor, RORα, which was an important endogenous mediator of MLT‐exerted anti-inflammation against PD (Fig. 6c). ' <<<
Given the known excellent safety profile of melatonin even at high dose, this begs the question of why there has not been a very high dose melatonin study in PwP to date?
The two 50 mg melatonin / PwP studies just put a bigger question mark on the question! Such a study could be potentially done in two to three years depending on size and design.
A new study showing yet another method of action by which melatonin fights against PD, by protecting against MPP induced neuronal toxicity through its anti inflammatory and antiapoptotic effects.
A major concern about using high dose melatonin is that many people are not aware of the safety of melatonin even at ultra high dosing. In the following study, women between the age of 45 and 55 were given 3000 mg of melatonin everyday for 6 months :
' Forty women aged 45-55 years and at least 6 months of amenorrhea were enrolled in this study. They were randomly assigned to two groups of 20 each. One group took myo-inositol (myo-Ins) (2 g twice a day) and the other group took 2 g/d myo-Ins plus 3 g/d melatonin before sleeping. '
In this next study, they gave participants a one time dose of 50 mg/kg/bw. In a person like myself weighing about 80 kilos, that would be equivalent to 4000 mg :
' Melatonin treatment resulted in lower postoperative transaminases over the study period (P = 0.6). There was no serious adverse event in patients after melatonin treatment. '
These studies give some clues about the safety of melatonin.
Interestingly, they gave mice melatonin at a dose that would be very similar to the 132 mg+/day that I take. They only treated the mice for 7 days at this dose, but found that melatonin had a significant impact on the disease process in just one week. It makes me wonder what would have happened after 3 months instead of just one week.
Here is a quote from the study :
' Of a 1-methyl-4-phenyl-1,2,3,6-tetrahydropyridine (MPTP) - induced mouse model with RORα levels reduced in the midbrain tissue, MLT treatment (intraperitoneal 20 mg/kg/d for 7 days) significantly increased the RORα levels and protected dopamine neurons, with decreased inflammation and increased anti-inflammatory M2-like phenotype in the microglia. Furthermore, siRNA-mediated knockdown implied the involvement of signal transducer and activator of transcription (STAT) pathway. In conclusion, MLT ameliorates neuroinflammation by inhibiting STAT-related pro-inflammatory (M1-like) polarization of microglia, revealing alternative options for neuroprotective treatment of PD. '
It is good to see that they are delving deeper into the science to better understand why melatonin helps people with PD.
' We found that treatment with BLT, exogenous melatonin or melatonin agonists seemed to have positive effects on sleep quality, depression and some other non-motor symptoms, and interestingly, also on motor function in PD (Fig. 2). Taking into account the low prevalence of side effects and the relative ease with which these treatments can be administered, they hold promise for future more widespread use in PwP. '
Content on HealthUnlocked does not replace the relationship between you and doctors or other healthcare professionals nor the advice you receive from them.
Never delay seeking advice or dialling emergency services because of something that you have read on HealthUnlocked.
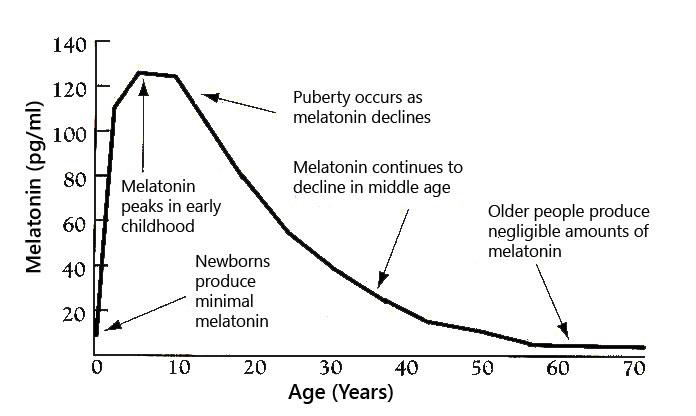


")