This post, prepared in collaboration with AussieNeil , draws together some earlier posts relating to SARS-CoV-2 infection and CLL.
COVID-19 RISK FOR CLL PATIENTS
Due to their impaired humoral and cellular immune function, CLL patients are at particular risk for infection, including SARS-CoV-2 infection.
CLL patients can experience:
• Covid-19 symptoms of varying severity. On the whole, though, they will usually clear their infection more slowly and are at a heightened risk of a serious outcome.
In addition, they may experience:
• Treatment-related immunodeficiency (such as that resulting from anti-CD20 monoclonal antibody treatment such as Rituximab (Mabthera/Rituxan), Obinutuzumab (Gazyva) or ofatumumab (Arzerra)
In a recent study, ‘individual risk factors associated with a poor prognosis included
• advanced age of 75 years and older, a CIRS [cumulative illness rating score] score in excess of 6, chronic renal disease, and asthma’. ( physiciansweekly.com/death-... )
PREVENTATIVE MEASURES
VACCINE PROTECTION AGAINST SARS-CoV-2:
People with CLL are likely to mount a reduced response to vaccines, not just to SARS-CoV-2 vaccines.
However, vaccination is very strongly recommended for them, even for those taking a BTK inhibitor like ibrutinib, acalabrutinib, zanubrutinib and pirtobrutinib which may impair their vaccination response further.
This October 2024 post Patients with CLL are immunocompromised and recommended to receive COVID-19 vaccination regardless of treatment status or specific therapy, references a letter by authors including the internationally highly respected CLL specialists Drs Jennifer Brown and John Seymour, regarding an AMPLIFY trial study, confirming the advantage of COVID-19 vaccination during treatment. healthunlocked.com/cllsuppo...
Those contemplating anti-CD20 monoclonal antibody treatment are advised to get vaccinated before starting treatment, if at all possible. Otherwise they are unlikely to generate an antibody response until at least 12 months after their last infusion.
In many places, the current protocol for CLL patients is that they should have a three-dose primary vaccination course followed by a fourth, booster vaccination. In late March 2022, the FDA recommended "immunocompromised people receive five doses of mRNA vaccine in total: a three-dose primary series, and two boosters."
There is some suggestion that mixing vaccines may provide a stronger immune response. In general, mRNA vaccines are currently recommended for the CLL cohort. Seropositive responses (ability to produce antibodies) in the immunocompromised is reduced or lacking and so ongoing vaccination will most likely be needed. It’s likely that new vaccines may be needed to respond to any emerging SARS-CoV-2 variants. The task of developing vaccines that could be used for all coronavirus infections (PAN Vaccines) and that reduce transmission further is ongoing. See Universal coronavirus vaccines in development: healthunlocked.com/cllsuppo... One possibility is combined annual flu/coronavirus vaccinations.
There has also been a study indicating that a patient’s age, treatment and time between end of treatment and vaccination can impact a CLL patient’s response to vaccination. It also showed evidence that those who received the Moderna 100μg mounted a stronger response than those who received the Pfizer 30μg, indicating that the amount of spike mRNA administered is important for CLL patients.
Currently, vaccination alone isn’t enough to completely remove the risk of SARS-CoV-2 infection and so additional preventative measures are necessary. A ‘vaccine plus’ approach recommends social distancing wherever possible, hand hygiene, good ventilation, air filtration, quality mask wearing and global vaccine equity. A good N95, P2/FFP2 or KF94 mask is preferred. Many authorities around the world have also started the process of improving air quality in public buildings as a result of the pandemic.
NOTE: DON'T WAIT UNTIL YOU'VE TESTED POSITIVE TO WORK OUT YOUR TREATMENT ACTION PLAN. Time will be of the essence if you do test positive for Covid-19 so be prepared: work out your treatment action plan ahead of time by discussing your needs with your specialist and /or primary health care provider.
PRE-EXPOSURE:
MONOCLONAL ANTIBODIES
Evusheld is a combination of two human monoclonal antibodies, tixagevimab (AZD8895) and cilgavimab (AZD1061). It is not intended to be used as a substitute for vaccination against COVID-19 for the general public.
It is administered by injection, with one intramuscular injection for each antibody, given one immediately after the other. It is given:
• To people with moderately to severely weakened immunity or to people who cannot be fully vaccinated due to a history of severe reaction to coronavirus vaccines
On 24 February 2022, the FDA updated its emergency use authorization for Evusheld (tixagevimab co-packaged with cilgavimab), in response to concerns that it may be less active against certain Omicron subvariants. The supply of Evusheld was limited before this decision which will, no doubt, make it harder to source.
'With this EUA revision, FDA has increased the initial authorized dose to 300 mg of tixagevimab and 300 mg of cilgavimab. Patients who have already received the previously authorized dose (150 mg of tixagevimab and 150 mg of cilgavimab) should receive an additional dose of 150 mg of tixagevimab and 150 mg of cilgavimab as soon as possible to raise their monoclonal antibody levels to those expected for patients receiving the higher dose.'
Updated ..on June 29, 2022, FDA revised the Evusheld Fact Sheet for Healthcare Providersfda.gov/media/154701/download to recommend repeat dosing every six months with a dose of 300 mg of tixagevimab and 300 mg cilgavimab if patients need ongoing protection. The previous Fact Sheet for Healthcare Providers did not provide a specific recommendation on the dosing interval.
We continue to monitor the neutralizing activity of Evusheld against emerging SARS-CoV-2 variants and will provide additional updates as needed.
24th March 2022 EMA recommends authorisation of COVID-19 medicine Evusheld
EMA’s human medicines committee (CHMP) has recommended granting a marketing authorisation for Evusheld, developed by AstraZeneca AB, for the prevention of COVID-19 in adults and adolescents from 12 years of age weighing at least 40 kg before potential exposure to the SARS-CoV-2 virus.
In Australia from 7th March 2022, "Evusheld (tixagevimab and cilgavimab) has provisional approval for the pre-exposure prophylaxis of COVID-19 in adults and adolescents aged 12 years and older weighing at least 40 kg,
- who have moderate to severe immune compromise due to a medical condition or receipt of immunosuppressive medications or treatments that make it likely that they will not mount an adequate immune response to COVID-19 vaccination or
- for whom vaccination with any approved COVID-19 vaccine is not recommended due to a history of severe adverse reaction (for example., severe allergic reaction) to a COVID 19 vaccine(s) and/or COVID‐19 vaccine component(s).
Evusheld is not recommended as a substitute for vaccination in individuals for whom COVID 19 vaccination is recommended."
— In lab study, monoclonal antibodies required much higher concentrations versus Omicron subvariant
While two monoclonal antibody combinations showed neutralizing activity against the Omicron subvariant BA.2, both required substantially higher concentrations to produce a response in patients with COVID-19, Japanese researchers said, while antivirals appeared to be less affected.
Casirivimab/imdevimab (REGEN-COV) and tixagevimab/cilgavimab (Evusheld) inhibited BA.2, but the titer of monoclonal antibodies "required for a 50% reduction in the number of infectious foci" for BA.2 was higher by a factor of 43.0 to 143.6 for the former and by a factor of 1.4 to 8.1 for the latter compared with the ancestral strain and other variants, reported Yoshihiro Kawaoka, DVM, PhD, of the University of Tokyo, and colleagues.
EVUSHELD OMICRON UPDATE: 31st May 2022 - “Using national real-world data from predominantly vaccinated, immunocompromised Veterans, administration of tixagevimab/cilgavimab was associated with lower rates of SARS-CoV-2 infection, COVID-19 hospitalization, and all-cause mortality during the Omicron surge.” medrxiv.org/content/10.1101...
There are two types of testing readily available to those who suspect they have been infected with SARS-CoV-2:
Nucleic acid tests such as PCR (polymerase chain reaction) tests and
RAT/LFT (rapid antigen/lateral flow) tests
We also have the first COVID-19 breathalyzer model authorised by the FDA, the InspectIR
PCR tests are generally better at detecting COVID-19 than rapid antigen tests. Their downside is that a PCR test must be analysed in a laboratory, not at home.
While RAT/LFT tests are generally best performed within the first 7 days from when symptoms first appear and are most accurate if you have symptoms, they still can be useful to determine if an asymptomatic person might be likely to be infectious with COVID-19 and can be performed anywhere.
They work best, not as a one-off test, but as a test repeated over a few days or on an ongoing basis as a monitoring test. Recently, RAT/LFTs have been used as a workplace screening tool and in schools to monitor disease spread. In some places, they can be provided as proof of infection instead of a PCR. Different places have different protocols for both PCR and RAT/LFTs so check with your local health authority. 15 things not to do when using a rapid antigen testtheconversation.com/15-thin...
These earlier posts contain more detailed information about RAT/LFTs.
On 14th April 2022, the FDA authorised the use of the InspectIR COVID-19 Breathalyser, which can deliver test results in under 3 minutes! healthunlocked.com/cllsuppo...
TREATMENT:
Should a CLL patient become infected with Covid-19, it is recommended that they take early proactive action. Currently, there is a small number of suitable post infection treatments and they are in short supply in many places:
a) Monoclonal antibody treatments such as Sotrovimab which is administered as an infusion. In Feb 2022, the FDA gave Emegency Use Authorisation for another monoclonal antibody treatment, named Bebtelovimab, also administered by infusion. On 25 March, US health officials 'stopped the further deployment of the Covid-19 treatment sotrovimab to places where the BA.2 coronavirus variant is now causing the majority of infections, given laboratory studies showing the treatment likely doesn’t work against the variant.'statnews.com/2022/03/25/fda.... aspr.hhs.gov/COVID-19/Thera... On 5 April, the FDA announced that ‘Sotrovimab is no longer authorized to treat COVID-19 in any U.S. region due to increases in the proportion of COVID-19 cases caused by the Omicron BA.2 sub-variant’. fda.gov/drugs/drug-safety-a...
On 7th April, Australia's Therapeutic Goods Administration (TGA) received an application from GlaxoSmithKline (GSK) Australia Pty Ltd for a higher (1000 mg) dose of its COVID 19 treatment, sotrovimab (XEVUDY). This higher dose will be considered for treatment of patients suspected to have infection caused by the Omicron BA.2 sublineage. tga.gov.au/media-release/tg...
FDA has approved OLUMIANT® (baricitinib) for the treatment of COVID-19 in hospitalized adults requiring supplemental oxygen, non-invasive or invasive mechanical ventilation, or extracorporeal membrane oxygenation (ECMO) with a recommended dose of 4-mg once daily for 14 days or until hospital discharge, whichever comes first.
b) Antiviral treatments such as Paxlovid, administered in pill form. Process followed to avoid Paxlovid Drug-Drug interactions is covered in How to Recognize and Manage Drug–Drug Interactions:
Both monoclonal and antiviral types of treatments need to be administered soon after infection so it is important to act early. Recent advice (June 2022) in a Leukaemia Foundation webinar for patients in Australia was that they should not waste time waiting for a RAT/LFT to be able to determine if they are positive but to access a PCR test as soon as possible if Covid is suspected.
‘Disease rebound’ has been experienced by some people taking Paxlovid - 2-8 days after recovery. The CDC issued a statement about the potential recurrence of COVID-19 after Paxlovid treatment on on 26 May 2022. Treatment extension is not currently recommended: emergency.cdc.gov/han/2022/...
On 17th March 2023, given Paxlovid reduces the chance of hospitalization and death by about 60 to 85 percent for seniors and adults who have health issues that include obesity, diabetes, lung disease, and immune system disorders, an FDA advisory panel voted 16-1 that the Pfizer drug remains a safe and effective treatment and should be given full approval. The FDA is expected to make a final decision on full approval by May,
If none of the above treatments is available or suitable for you, you might be able to access the antiviral molnupiravir. healthunlocked.com/cllsuppo...
CANADIAN TREATMENT INFORMATION AND LOCATOR WEBSITE:
In the USA a further 20 million courses of Paxlovid have been secured and there are plans to offer this antiviral at up to 20,000 more pharmacies. (April 26th 2022)
In mid June 2022, Pfizer released a statement that suggests that Paxlovid is more effective in those who are at high risk of becoming severely ill with Covid-19 and less effective in those with average risk. The company has stopped enrolling people into its Phase 2/3 trial which failed to demonstrate that the antiviral treatment reduced the relative risk of contracting COVID-19 and did not produce statistically significant data that it reduced the risk of hospitalizations and deaths in the general population. However, it does plan to continue testing its efficacy in high risk patients.
This COVID-19 therapeutics locator for the USA may also assist those seeking monoclonal antibodies or antivirals: covid-19-therapeutics-locat...
The following two sites were recommended by Marcia B on the CLL ACOR List
The best locator for Evusheld was developed by Roy Relyea, a Microsoft engineer whose wife had cancer and was an Evusheld candidate, This site has helped thousands.
SeymourB notes that "the locations shown are where doses were shipped, not places that doses are available. Large medical providers often have doses shipped to a central location, and then re-ship to their other locations. I suggest trying to call the pharmacy at what ever location is listed to find out the procedures."
He (Roy Relyea) also has sister sites for help in locating the other monoclonal antibodies.
Another source is a facebook group, devoted to Evusheld only, where we all help each other find specific locations.
CoVac-1, a COVID-19 vaccine, that has induced T-cell responses in patients with B-cell deficiencies, including those with lymphoma and leukemia, according to study results presented during American Association for Cancer Research Annual Meeting in April 2022.
ResApp, a mobile phone app that can assist in the diagnosis of Covid. Pfizer has reportedly considering a $100 million offer to the Queensland, Australia, developers of this app which uses information about the person being tested and the sound of their coughs to diagnose if they have Covid. It's very early days for this technology but definitely worth a watch.
Per the Fact Sheet for Healthcare Providers pdf on 3rd October 2022
. VLPs pseudotyped with the SARS-CoV-2
spike of Omicron BA.4.6 showed reduced susceptibility to tixagevimab (>1,000-fold) and to
cilgavimab (>1,000-fold). The effects of the individual substitutions in Omicron spike glycoproteins on neutralization susceptibility are being investigated
Thank you! This is the most thorough and clear explanation I have seen. We all need to read and take note. If only the UK government acted on scientific/medical advice and explained the precautions needed as clearly.
The image I’ve just uploaded to this post is from a journal pre-proof titled Antiviral agents for the treatment of COVID-19: progress and challenges by Manmeet Singh and Emmie de Wit (the journal is Cell Reports Medicine).
‘The value of administering direct-acting antivirals to at-risk patients early after diagnosis is clear’ and that
‘ . . . their efficacy increases even with small reductions in time to treatment initiation’.
‘Combination treatments consisting of two or more direct-acting antivirals from a different class (e.g., a nucleotide analog plus monoclonal antibody) will likely reduce the chance of escape variants to emerge and may improve the clinical benefit of treatment. Combination treatment should therefore be investigated in clinical trials.’
‘. . . there is an ongoing search for broad-acting antivirals that are effective against multiple viruses within one family, or even against viruses from different families. However, we also need to invest in research that will help us determine which of these newly discovered viruses form a pandemic threat.’
Two experts in the field of infectious diseases, Luciana Borio, MD, and Rick Bright, PHD, consider the probability that SARS-CoV-2 will develop resistance to antivirals
Dr Borio. "The idea of monotherapy for an RNA virus I think is concerning. And I would like to be able to see us move it into combination antiviral therapy to treat SARS-CoV-2.
I think it's a matter of time before we begin to see resistance emerge, and to get to this idea of combination therapy -- you know, this is what I call the work of government. It doesn't happen without government intervention to bring companies together, to bring assets together, to help establish protocols for setting combination therapy, to help generate agreements between the pharmaceutical sector so they can collaborate on this, the regulatory pathways to get combination therapy approved.
That is the work of the government, and it needs to be done because it's a matter of time before we lose valuable drugs.
Bright: I'll jump in there too, just to add. Dr. Borio is exactly right. We should anticipate that the viruses will outsmart and evolve around these antiviral drugs. We will see antiviral resistance."
The NEJM has printed an article that reports the results of the phase 2–3 double-blind, randomized, controlled trial of 300 mg of nirmatrelvir plus 100 mg of ritonavir (PAXLOVID). For details, see: healthunlocked.com/cllsuppo...
Can Coronavirus Antibody Testing Measure Your Protection Against Covid-19?
Long, but non technical and informative read, where Bruce Y. Lee explains why "A single number rarely can tell you enough to make a decision". Includes a 10 minute audio presentation of the article:
"All in all, don’t use antibody tests to decide what to do about face mask wearing, quarantining, other social distancing measures, and ventilation or whether to get vaccinated. Instead, try to maintain at least three types of Covid-19 precautions at all times and follow public health recommendations, regardless of what your antibody levels are. Having had natural infection is not a replacement for vaccination. As I have covered previously for Forbes, studies have shown that vaccination may offer much better protection than natural infection, especially since natural infection can be so variable in its course and severity and the resulting immune response."
Relevant statement by Dr Rick Furman to the CLL/SLL groups.io community
"Re: Results from antibody test
From: Rick Furman
Date: Fri, 18 Feb 2022 10:56:00 ACDT
The only data that matter are the clinical outcomes data. We do know that vaccines are effective at preventing symptomatic COVID-19 infections because when the did the studies, those vaccinated had a much lower risk of developing symptomatic disease and the severity was far less. Those are the data from the studies and importantly, the data that matters.
Rick Furman"
Updated to include Dr Furman's statement on antibody test results
Covid-19 transmission is still high in many places, and, unfortunately, the US and Europe look as if they may be at the start of another surge. This statement aims to address the specific impact of the pandemic on immunocompromised blood cancer patients (both acute and chronic), and to recommend solutions and actions to mitigate those risks'.
Prescribing Paxlovid (Nirmatrelvir–Ritonavir) : How to Recognize and Manage Drug–Drug Interactions: acpjournals.org/doi/10.7326...
Added 27th March 2022, from CLL/SLL groups.io
From: Rick Furman
Date: Sat, 26 Mar 2022 12:45:08 ACDT
Ibrutinib should be held while on Paxlovid. Since Paxlovid is only five days, it should not be an issue. A lower dose is an option, but only if you are on capsules, as you could not get a new prescription quickly enough.
Rick Furman
Flow chart covering prescribing process for Paxlovid.
Note: "A booster dose of vaccine improves your protection against Omicron. Vaccine effectiveness against hospitalisation is 83% ten or more weeks after the booster.
Protection against symptomatic disease increases too. Vaccine effectiveness is 65-75% two to four weeks after the booster, reducing to 45-50% ten weeks after the booster.
Pfizer and Moderna have also developed an Omicron-specific vaccine which they are about to test in clinical trials and could be available in the second half of 2022."
We measure how contagious a disease is by the basic reproduction number (R0). This is the average number of people an initial case infects in a population with no immunity (from vaccines or previous infection).
New mutations give the virus an advantage if they can increase transmissibility:
- the original Wuhan strain has an R0 of 3.3
- Delta has an R0 of 5.1
- Omicron BA.1 has an R0 of 9.5
- BA.2, which is the dominant subvariant in Australia at the moment, is 1.4 times more transmissible than BA.1, and so has an R0 of about 13.3
- a pre-print publication from South Africa suggests BA.4/5 has a growth advantage over BA.2 similar to the growth advantage of BA.2 over BA.1. That would give it an R0 of 18.6.
This is similar to measles, which was until now was our most infectious viral disease.
How likely is reinfection?
BA.4/BA.5 appear to be masters at evading immunity. This increases the chance of reinfection.
How severe is the disease from BA.4/5?
A recent pre-print publication (a publication that has so far not been peer-reviewed) from a Japanese research group found that in lab-based, cell-culture experiments, BA.4/5 was able to replicate more efficiently in the lungs than BA.2. In hamster experiments, it developed into more serious illness.
However, data from South Africa and the United Kingdom found that their BA.4/5 wave didn’t see a major increase in severe disease and death.
This is possibly because of the high rates of immunity due to previous infections. Our high rates of vaccine-induced immunity might have a similar protective effect here.
Will BA.4/5 change long COVID?
At this stage, we do not know whether any of the Omicron subvariants differ in their ability to cause long COVID.
However, we do know that full vaccination (three doses for most people) does provide some protection against long COVID.
How protective are our vaccines against BA.4/5?
Each new subvariant of Omicron has been better able to evade immunity from vaccination than its predecessor.
Although current vaccines based on the Wuhan strain will still provide some protection against serious illness and death against BA.4/5, they are unlikely to provide much, if any, protection against infection or symptomatic disease.
What about new vaccines?
The good news is second-generation vaccines are in clinical trials. Moderna is trialling a vaccine containing mRNA against the original Wuhan strain and Omicron BA.1.
Early results are very promising, and likely to give much better protection against BA.4/5.
I found a decent source of Evusheld and Paxlovid in a small pharmacy just 5 miles from home, vs. a one hour + trek 30 miles into NYC ( +$18 tolls, +$30 parking)Thanks
I've updated this post to reflect the recent and disappointing news that the FDA is now limiting distribution of sotrovimab to areas where the Omicron BA.2 variant is not dominant.
Sotrovimab is effective against Omicron BA.1 but lab tests are showing it to be much less useful against BA.2.
This is not the first time that a monoclonal antibody has been found wanting in the event of a new variant. Creating a monoclonal antibody treatment that will work well when new variants arise is predictably proving to be a challenge.
Lab data for Bebtelovimab suggests it will be effective against BA.2 and it was authorised by the FDA last month.
We've been learning a lot about how Omicron BA.1 and BA.2 compare in recent weeks. Here's a summary table that I compiled and will update when more data become available
"I’ve previously written about, we’re very lucky) there is no drop-off between BA.1 and BA.2 with respect to vaccine effectiveness. For both, the protection vs infections starts out low, approximately 50%, and falls off substantially after a few months (which is why we had an enormous number of breakthrough infections in the first Omicron wave). But, importantly, the mRNA vaccines hold up well with a fresh booster against BA.1 or BA.2 vs hospitalizations and deaths. It has been estimated that about 40% of Americans were infected with the first wave of Omicron (with BA.1 or BA1.1) so there will be cross-reactive immunity/protection that should help reduce the severity of the wave, especially in people with hybrid immunity of vaccination and Omicron BA.1 infection. Here’s a summary Table of the features of the 2 main Omicron variants. Please note that the vaccine effectiveness vs hospitalization is an under-estimate from the UKHSA most recent (March 24) report. A recent study from Qatar, which also partitioned BA.1 and BA.2, showed very high (>99%) short-term 3-shot effectiveness for both Omicron variants vs hospitalizations and deaths."
I’ve updated this post to add the new US Govt website that can help people there find information about getting masks, vaccines, tests and treatments. I've also added information about the UK arrangements for people who are at highest risk of becoming seriously ill if they contract Covid-19 .
Mystic75 has posted tips for US members facing the Omicron BA.2 variant wave. How serious this wave will be is hard to determine. While this variant is being observed in waste water testing and the US level of vaccination is lower than most other affluent countries, there may be a higher than expected level of community immunity from prior COVID-19 infections: healthunlocked.com/cllsuppo...
(Reuters) – Two drugs that looked like promising treatments for COVID-19 in preliminary studies - remdesivir for hospitalized patients and camostat for patients who are not seriously ill - failed to show a benefit in those groups in randomized controlled trials, researchers reported in two separate papers.
In five European countries, researchers studied 843 COVID-19 patients who were hospitalized between March 2020 and January 2021 with hypoxemia and who needed supplemental oxygen or mechanical ventilation.
Patients received either Gilead Sciences’ antiviral remdesivir - sold as Veklury - for up to 10 days, plus standard of care, or standard of care alone. At 15 days, there was no difference between the groups in signs of improvement, investigators reported.
InspectIR COVID-19 Breathalyser gains FDA emergency use authorization
Today (14th April 2022), the U.S. Food and Drug Administration issued an emergency use authorization (EUA) for the first COVID-19 diagnostic test that detects chemical compounds in breath samples associated with a SARS-CoV-2 infection. The test can be performed in environments where the patient specimen is both collected and analyzed, such as doctor’s offices, hospitals and mobile testing sites, using an instrument about the size of a piece of carry-on luggage. The test is performed by a qualified, trained operator under the supervision of a health care provider licensed or authorized by state law to prescribe tests and can provide results in less than three minutes.
Experts Break Down What Could Help Improve Access to Paxlovid (USA perspective)— "A lot of it boils down to a lack of patient and provider familiarity with the medication"
A further 20 million courses of Paxlovid have just been secured for the US and there are plans to offer this antiviral at up to 20,000 more pharmacies.
Per this Medpage Today article, as of 20th April 2022, Omicron subvariant BA.2.12.1 accounted for more than 75% of sequenced cases in Central New York and about 42% of cases across New York. Nationwide, this subvariant has grown from 3.5% to nearly 30% of cases in little more than a month.
"What we're seeing right now is a version of the virus that is much more transmissible than previous versions of the virus, perhaps, but also less likely to cause severe disease," Perry Halkitis, PhD, MPH, dean of the Rutgers School of Public Health, told MedPage Today.
"None of this is odd," Halkitis said. "What is problematic is the speed with which it seems to be spreading. And the speed with which it seems to be spreading, to me, has something to do with the virus, but more to do with human behavior."
Individuals have been going about their business without mitigation measures, he explained. They haven't been masking in public places, they've been going to extremely large gatherings, and they haven't been getting boosted and have waning antibodies.
"All of this in combination puts us in the situation that we see right now," Halkitis said.
However, there hasn't been the same magnitude of hospitalizations and deaths as with previous iterations, he added.
:
In light of new variants, the reformulation of the COVID vaccine will be significant, Halkitis said. "That is the future, right there," he said.
Pfizer Inc on Friday said a large trial found that its COVID-19 oral antiviral treatment Paxlovid was not effective at preventing coronavirus infection in people living with someone who had been exposed to the virus.
The trial enrolled 3,000 adults who were household contacts exposed to an individual who was experiencing symptoms and had recently tested positive for COVID-19. They were either given Paxlovid for five or 10 days or a placebo.
Those who took the five-day course were found to be 32% less likely to become infected than the placebo group. That rose to 37% with 10 days of Paxlovid. However, the results were not statistically significant and thus possibly due to chance.
How can it be 32% or 37% better for 1,500 people and not be statistically significant- that blows my mind.
-
The only thing I could understand, is if the writer of the article misunderstood the comment and the 5 day 32% and the 10 day 37% were not statistically different from each other but the 32 % was significant over placebo.
-
And I find the added comment to be extremely significant for me: Pfizer said safety data in the trial was consistent with previous studies, which had shown the pills to be nearly 90% effective at preventing hospitalization or death in COVID patients at high risk of severe illness when taken for five days shortly after symptom onset.
Pfizer released another statement regarding Paxlovid on 14 June 2022 which reported on its trial for "standard-risk" adults. That trial has now stopped taking enrollments after failing to demonstrate sufficient benefit in that population. It will, however, continue its study in higher-risk patients as previous data has shown strong efficacy in that group.
The company announced this change 'after failing to prove the antiviral treatment reduced the relative risk of contracting COVID-19'. In addition, the ' drugmaker could not produce statistically significant data on whether the nation's most prescribed COVID-19 treatment was effective in reducing the risk of hospitalizations and deaths'.
'A study of more than 2,200 patients at high risk from Covid-19 showed that Paxlovid cut the risk of hospitalization or death by 89% compared with a placebo.
Pfizer said it would stop enrolling study participants in the standard-risk group and focus instead on those at higher risk of severe outcomes, which still amounts to a substantial number of people.' (my emphasis)
' . . . many important questions about Paxlovid are still unanswered: Can it decrease the risk of long Covid, for example? Can it cut the chances that an infected person could pass it to someone else?
May 11th 2022 The U.S. Food and Drug Administration (FDA) has approved OLUMIANT® (baricitinib) for the treatment of COVID-19 in hospitalized adults requiring supplemental oxygen, non-invasive or invasive mechanical ventilation, or extracorporeal membrane oxygenation (ECMO) with a recommended dose of 4-mg once daily for 14 days or until hospital discharge, whichever comes first.
While this article by a freelance science journalist provides good coverage of the current status and anticipated developments for vaccines and antivirals, it doesn't cover monoclonal antibodies, nor treatments for hospitalised patients. We also need a similar article covering Non Pharmaceutical Interventions.
'Sars-CoV-2 continues to infect millions of people worldwide and cause an estimated 10,000 deaths per day, as the US alone approaches one million dead. It is widely expected to become endemic, remaining in circulation for the foreseeable future, and continuing to cause substantial numbers of hospitalisations and deaths, especially among vulnerable groups. ‘Covid kills about tenfold more people than flu, based on historical information,’ says Penny Ward, professor of pharmaceutical medicine at King’s College London, UK.
Existing vaccines reduce the probability of severe disease, but do not protect against infection. Immunity also wanes within months, particularly against the newest emerging variants. This leaves room for companies to develop more effective antivirals and vaccines in the coming months or even years.
:
The eventual fate of the Sars-CoV-2 virus remains uncertain. There is a strong suspicion that it will follow a path towards becoming a ‘common cold’ coronavirus, although how long it would take to reach this destination is unknown. ‘It might become a regular human endemic coronavirus over the next eight to ten years,’ says Penny Ward, ‘and I think omicron is going to carry us from pandemic to endemic, but we don’t know how much pathogenicity an endemic Sars-CoV-2 will carry with it.’
Regular boosters of vulnerable groups may be needed for years to come to protect against severe disease, with Covid-19 sticking around to cause cold symptoms amongst healthy adults and severe illness among vulnerable people. Treatments for vulnerable patients will continue to be needed, especially in countries where vaccination and/or infection rates have been relatively low.'
"A new @bmj_latest systematic review of 53 studies of boosters and mix and match shows marked benefit of boosters but little difference for mixing (mRNA and adenovirus) vs matching (3 mRNAs)"t.co/QsoBUwyIhxt.co/euWoXj3ul8
From a living Systematic Review with Network Analysis
Today's COVID-19 vaccines are all based on the original version of the coronavirus.
Experts say they still provide strong protection against severe disease, hospitalisation and death, even after the appearance of the Omicron variant — especially if people have had an initial booster dose.
But the virus continues to mutate rapidly in ways that let it evade some of the vaccines' protections and cause milder infections.
US regulators and the World Health Organization are considering whether to order a change in the vaccine recipe for a new round of booster shots later this year, when colder weather in the northern hemisphere is expected to drive yet another surge.
FromModerna's Omicron-specific vaccine could replace current booster, study shows promising results
Key points:
- Preliminary results show people given the jab experienced a higher boost in Omicron-fighting antibodies
- Pfizer is also studying a combination shot
- Antibodies wane over time, so it is not clear how long protection could last
(Also, study results showing are not yet peer reviewed)
Large companies such as Pfizer and Moderna can feasibly make an Omicron-specific vaccine for testing within a week or so, says Colin Pouton, a pharmaceutical biologist at Monash University.
"And if an Omicron vaccine is going to be any good to you and I, it has to produce new antibodies against Omicron."
So first, they test if the Omicron vaccine does that in mice.
"But if you do animal experiments [with an Omicron-specific booster shot], and look for protection against Omicron, an Omicron version of their vaccine actually doesn't do any better than the original Wuhan vaccine," Professor Pouton says.
So, what's going on?
Giving a person (or mouse) multiple vaccines with ever-so-slight differences in their makeup can cause a phenomenon called "immunological imprinting".
"When you give a vaccine, you prime the immune response to produce antibodies … then you boost it by giving a second dose or a third dose," Professor Pouton says.
But if you're then vaccinated against a slightly different variant, you might make fewer antibodies that specifically work on that new viral variant.
That's because, when confronted with a similar vaccine, your immune system prefers to recruit existing antibody-producing B cells back into action, rather than develop new ones.
... non-neutralising antibodies make up the lion's share of COVID-vaccine-generated antibodies, says Dale Godfrey, an immunologist at the Peter Doherty Institute for Infection and Immunity.
"Only about 10-20 per cent of antibodies bind the receptor-binding domain compared to the rest of the spike protein when people are immunised with whole-spike vaccine."
:
The vaccines in the trial are based on the Beta variant, as that was the variant of concern when the project began.
The Beta variant shares some of Omicron's mutations, Professor Godfrey says.
"As to whether this means the vaccine will provide superior protection against Omicron, we think and hope so, but don't know yet."
Pfizer and Moderna are continuing with clinical trials to see how their Omicron-specific whole-spike vaccines fare in people. (see above - Neil)
Moderna is also trialling a "bivalent" version that combines the original vaccine, as well as the new Omicron-specific spike mRNA.
We might not have to wait too long to find out how well they work.
Israel study finds Paxlovid reduces risk for severe COVID-19, death by 46%
Among the 180,351 eligible patients included in the study, 4,737 were treated with Paxlovid and 135,482 had an adequate COVID-19 vaccination status.
The study demonstrated that both Paxlovid and adequate COVID-19 vaccination status were associated with a significant decrease in the rate of severe COVID-19 or mortality (adjusted HR = 0.54; 95% CI, 0.39-0.75 and aHR = 0.20; 95% CI, 0.17-0.22, respectively). They also found that the effect of Paxlovid was seemingly more significant among older patients, immunosuppressed patients and patients with underlying neurological or cardiovascular disease (P < .05).
“COVID-19 vaccination remains the most effective intervention to prevent disease progression and death among COVID-19 patients,” Najjar-Debbiny said. “However, another effective intervention would be the use of Paxlovid in high-risk patients suffering from a mild to moderate disease.”
Thanks to cllady01 for providing the links to the latest information about drug interactions with Paxlovid which I've added to the main post.
The recommendations for the different BTK Inhibitors, ibrutinib, acalabrutinib, zanubrutinib differ slightly and there is separate advice regarding venetoclax. See the link in the main post for details (they're in bold print and underlined to help them stand out).
The tables are not necessarily all-inclusive or all-comprehensive so it's best to check with your medical team before starting treatment for Covid but they do provide a very good guide.
A message for Australian members: Late last month, the Leukaemia Foundation in Australia held a webinar for Australian blood cancer patients to provide them with important Covid-19 related information.
"As the COVID-19 pandemic continues and we enter the winter flu season, you may be wondering how to best avoid infection and manage your health. It can be hard to keep on top of the new variants and ATAGI guidelines around vaccination, treatment, testing and isolation.
We know that many people with blood cancer are looking for trusted sources of information to help them make informed decisions. In this webinar we helped answer some of those questions and show you how to create your own COVID-19 Action Plan."
The three guest speakers are:
* Associate Professor Nada Hamad (Clinical Haematologist, St Vincent’s Hospital)
* Dr Krispin Hajkowicz (Infectious Diseases Specialist, Royal Brisbane & Woman's Hospital)
* Deborah Henderson (Living with CLL) (aka Debinoz)
The webinar was recorded and the video is available on the foundation's Youtube channel:
One of the important points made in this webinar is that RATs are no longer accurate enough for the immunocompromised to rely on them and that they should, wherever possible, try to get a PCR if they suspect they have Covid-19. This was also made clear in a news article in The New Daily today. Dr Chris Moy, Vice President of the Australian Medical Association, said:
'“The RATs have been useful at various stages of the pandemic, but they now have reduced sensitivity,” Dr Moy said.
“As the variants have grown worse the efficacy has really dropped off.”
Dr Moy said RATs had always been presumed to deliver negative results with 80 to 90 per cent accuracy.
“I think they are 60 per cent [accurate] now,” Dr Moy said.
“But the other issue is that they are now picking [Omicron COVID strains] up late.” . . . the advent of oral antivirals as a COVID treatment made it imperative that infections were tested within five days because the medication lost its effectiveness beyond that point.
“If you have a test that is either negative where it shouldn’t be or picking (the virus up) on day four or five, which we’re seeing more of, you run out of time,” he said.
This complicated the question of subsidising the tests for concession card holders, Dr Moy said, who were often older or otherwise had medical conditions that made them susceptible to severe infection.
“The usefulness of RATs in that group is actually worse (than average),” he said.'
Am I being exceptionally dim, but when I looked at the contra list it was very long and if I was unlucky enough to catch Covid I would have to make sure I am clear on all the medications I am on. I knew about Ibrutinib but unaware of any others.
Unfortunately, one of the challenges with some COVID-19 medications in particular, is the risk of serious interactions with other medications. Nirmatrelvir/Ritonavir (Paxlovid) is probably the most challenging in this regard. The other issue with the list is that drug marketing names can vary by country and the list uses drug names used in the UK. For example, Paracetamol (acetaminophen) on the list, is also known as APAP or Tylenol, depending on your country of residence. Yet there's no entry for APAP or Tylenol, the marketing names used in Europe and the USA respectively for Paracetamol (acetaminophen).
Switching to the 'Class' can help you find the entry for drugs you may be on.
The other issue is supplements. Anything that has a pharmacological effect can potentially interact with drugs. The notable exception is true homeopathic remedies, as they contain (hopefully) purified water with a "memory" of something which is supposed to cure you, in other words, the ultimate placebo.
I was just surprised by the lengthy list, but now I am more aware of the issue.
Having a problem with swallowing large pills I was concerned about the size of Paxlovid because prior to starting on Ibrutinib I had a choking problem with a painkiller that I still remember.
I was also interested with your comments on homeopathy because my lovely friend and osteopath is also a fan and uses Ainsworths in London. Recently I have become nervous of using homeopathic remedies ( apart from ) Arnica, so as a general comment do you think they are safe to use ? Cramp is a recent issue but my GP didn’t recommend extra magnesium ( levels good ) and I understand there is a homeopathic remedy.
In theory, nothing could be safer to use than a homeopathic remedy, because it's just a biochemically inert substance, usually water. Per Wikipedia "All relevant scientific knowledge about physics, chemistry, biochemistry and biology[6][7][8][9][10][11][12] contradicts homeopathy. Homeopathic remedies are typically biochemically inert, and have no effect on any known disease." and "The fundamental implausibility of homeopathy as well as a lack of demonstrable effectiveness has led to it being characterized within the scientific and medical communities as quackery and fraud."
The risk from a correctly prepared homeopathic remedy generally comes from not actually treating something which could become a serious illness. That's because homeopathy relies on the placebo effect.
With respect to Arnica, Healthline covers it well:
Homeopathic products have on occasion been recalled due to contamination concerns (e.g. bacterial) or insufficient dilution due to process control issues. Per WebMD webmd.com/balance/what-is-h...
...Treatments for other ailments are made from poison ivy, white arsenic, crushed whole bees, and an herb called arnica.
Homeopathic doctors (who also are called “homeopaths”) weaken these ingredients by adding water or alcohol. Then they shake the mixture as part of a process called “potentization.” They believe this step transfers the healing essence. Homeopaths also believe that the lower the dose, the more powerful the medicine. In fact, many of these remedies no longer contain any molecules of the original substance. They come in a variety of forms, like sugar pellets, liquid drops, creams, gels, and tablets.
I have only on rare occasions used Arnica to help with bruising which I personally have found effective and had no idea about it’s other uses, especially pain relief.
The American Society of Hematology journal, Blood, has published an article by Petra Langerbeins and Michael Hallek from the German CLL study group, titled 'COVID-19 in patients with hematologic malignancy'. It provides an excellent summary of where we are currently in the pandemic concerning the risk to patients with hematologic malignancy and treatment approaches for them. While not CLL specific, its general observations and advice hold for CLL patients.
" . . . the ongoing pandemic will remain a major challenge for patients with hematologic malignancy and their caregivers who need to constantly monitor the scientific progress in this area."
"Active immunization by vaccination remains an important element of protection for these patients. As the recent SARS-CoV-2 variants of concerns have increased their transmissibility, a first and second booster vaccination should be given to all patients with HM regardless of serologic results.
As the protection by COVID-19 vaccines is significantly reduced in patients with lymphoid malignancies or patients receiving B cell–directed treatments, preventive passive immunization with monoclonal antibodies (pre-exposure prophylaxis) is another milestone in containment of the pandemic and should be offered to all such patients with HM and to vaccine nonresponders.
Antiviral drugs and monoclonal antibodies for early treatment of COVID-19 have become available and should be given to all SARS-CoV-2–infected patients with HM to prevent severe or fatal courses. The treatment selection is based on efficacy against the current dominating SARS-CoV-2 variants, potential contraindications, drug interactions, and availability in different health care systems.
Moreover, we feel that it is important to establish specific programs and registries at a national and global level for patients with HM during this historic pandemic because they represent a particularly vulnerable group of patients with regard to COVID-19 in our society."
Petra Langerbeins, Michael Hallek; COVID-19 in patients with hematologic malignancy. Blood 2022; 140 (3): 236–252. doi: doi.org/10.1182/blood.20210...
The same edition of Blood contains related articles, about:
- vasculopathy n COVID-19,
- COVID-19 convalescent plasma and
- cellular therapies for the treatment and prevention of SARS-Cov-2 infection
Robert Flaumenhaft, Keiichi Enjyoji, Alec A. Schmaier; Vasculopathy in COVID-19. Blood 2022; 140 (3): 222–235. doi: doi.org/10.1182/blood.20210...
Aaron A. R. Tobian, Claudia S. Cohn, Beth H. Shaz; COVID-19 convalescent plasma. Blood 2022; 140 (3): 196–207. doi: doi.org/10.1182/blood.20210...
Susan R. Conway, Michael D. Keller, Catherine M. Bollard; Cellular therapies for the treatment and prevention of SARS-CoV-2 infection. Blood 2022; 140 (3): 208–221. doi: doi.org/10.1182/blood.20210...
Visual abstract: COVID-19 in patients with hematologic malignancy
News of President Biden testing positive for Covid-19 after he previously tested negative after a course of Paxlovid has raised interest in rebound infection and in the question of how long someone with Covid-19 might be infectious.
This Nature article provides a good summary of what scientists know so far about those things:
It's a reminder that immunocompromised people, who need to be cautious about how soon they catch up with family and friends who have been infected with Covid-19, should not rely on how long those people have been isolated but on evidence of whether they are likely to be infectious or not. This article suggests that it would be better to be guided by lateral flow (or ‘rapid antigen’) tests than any particular number of days.
'Although the question is simple — for how long is someone with COVID-19 contagious? — experts caution that the answer is complicated. “We always think of it as a black and white thing … if somebody’s infectious or not infectious — but in reality, it’s a numbers game and a probability,” says Benjamin Meyer, a virologist at the University of Geneva in Switzerland.
And that numbers game has shifting rules and baselines. Emerging variants, vaccination and varying levels of natural immunity provoked by previous infection can all influence how quickly someone can clear the virus from their system, Meyer says, and this ultimately dictates when they stop being infectious. Behavioural factors matter as well. People who feel unwell tend to mix less with others, he adds, so the severity of someone’s symptoms can influence how likely they are to infect others.
Something most scientists are confident about is that PCR tests can return a positive result even after someone is no longer infectious. This probably occurs when the tests, which detect viral RNA, pick up non-infectious remnants left behind after most of the live virus has been eliminated.
By contrast, lateral flow (or ‘rapid antigen’) tests offer a better guide to infectiousness, because they detect proteins produced by actively replicating virus.'
‘Michael Mina, a former Harvard University infectious-disease epidemiologist and immunologist who is an expert on rapid tests, said two tests 24 hours apart might provide extra security, like a double lock on your door. If people have access to tests, then “two tests in a row is just better form, better protection, than one negative test.” ‘
The journal Blood contains an article (dated 18 August 2022) titled "How I treat and prevent COVID-19 in patients with hematologic malignancies and recipients of cellular therapies". It presents a number of case studies, summary points, and a treatment algorithm.
The authors note that there are some limitations to their discussion, including the fact that the 'understanding of COVID-19 is evolving, and the data provided in this “How I Treat” article are based on the available literature and experience at the time of this publication (Algorithm). To address this limitation, we have provided hyperlinks to online resources for the most up-to-date information on treatment guidelines and therapies."
They also include a list of special considerations (in the form of answers to frequently asked questions) and conclude:
"SARS-CoV-2 remains a major threat to patients with hematologic malignancies and recipients of HCT and cellular therapy. SARS-CoV-2 vaccination remains the mainstay strategy to prevent severe COVID-19. However, given decreased vaccine immunogenicity and increased risk for breakthrough infections, additional therapeutic modalities are needed to complement vaccination strategies in patients with hematologic malignancies and recipients of HCT and cell therapy, such as preexposure COVID-19 mAbs (Table 3). Well-designed clinical trials that include this vulnerable patient population are critically needed to identify novel therapies with greater potency and more favorable toxicity profiles to prevent or treat SARS-CoV-2 infection."
Firas El Chaer, Jeffery J. Auletta, Roy F. Chemaly; How I treat and prevent COVID-19 in patients with hematologic malignancies and recipients of cellular therapies. Blood 2022; 140 (7): 673–684. doi: doi.org/10.1182/blood.20220...
Some updates about Sotrovimab, Bebtelovimab and Evusheld
Although it's not being used as much as it was, Sotrovimab is still being used in some places to manage Covid-19, particularly in patients for whom Paxlovid might not be suitable and where bebtelovimab is not available.
A recent report warns about using Sotrovimab in the immunocompromised, showing that they "face a considerable risk of prolonged viral shedding and emergence of escape mutations after early therapy with sotrovimab. These findings underscore the importance of careful monitoring and the need to conduct dedicated clinical trials for this patient population."
"Combination therapy with remdesivir significantly reduced the selection of escape variants."
The background statement for that study states:
"Monoclonal antibodies (mAb) targeting SARS-CoV-2 are predominantly less effective against Omicron variants. Immunocompromised patients often experience prolonged viral shedding and are therefore at increased risk for viral escape mutations, when mAbs are used as monotherapy."
Another recent study showed that "Monoclonal antibody treatment with bebtelovimab among COVID-19 outpatients is associated with lower odds of hospitalization or death, particularly among immunocompromised and older patients."
Finally, this week, the FDA "added important information to the authorized Fact Sheets for Evusheld (tixagevimab co-packaged with cilgavimab) to inform health care providers and individuals receiving Evusheld of the increased risk for developing COVID-19 when exposed to variants of SARS-CoV-2 that are not neutralized by Evusheld."
Detailed neutralization data can be found in Table 6 in the Evusheld Factsheet for Health Providers.
Omicron is showing poor efficacy against BA.4.6 which accounted for 12.8% of new cases in the US (and as high as >20% in some places) as of the week ending October 1 2022, a marked increase since the middle of the year.
Having said that, the "FDA continues to recommend Evusheld as an appropriate option for PrEP to prevent COVID-19, in combination with other preventative measures like getting vaccinated and boosted as recommended, as Evusheld still offers protection against many of the currently circulating variants and may offer protection against future variants."
The Medical Journal Of Australia has published an important review of early intervention treatments for Covid-19 in that country.
It contains information about currently available treatments, a treatment algorithm provided by NSW and the challenges with the current situation.
It concludes: "the number of available COVID‐19 treatment options will continue to grow over the coming months as new treatments that are currently being trialled become available. While hopefully supporting the treatment of COVID‐19 among a broader range of patient groups, an increase in the overall number of different options available would also appear to be our best chance at being able to live alongside the rapidly evolving SARS‐CoV‐2.'
Medications for early treatment of COVID‐19 in Australia, Adam Polkinghorne and James M Branley, Med J Aust || doi: 10.5694/mja2.51750, Published online: 24 October 2022
Of particular interest is a suggestion that clinical trials that involve more at-risk groups, including the immunocompromised, are needed to determine what approaches will work best for them, with a 5-day vs 10-day Paxlovid course being given as an example.
Thanks for this Australian update, CLlerinOz. I note that it also states what isn't recommended as follows:-
To date, clinical trials do not exist or have failed to show any improvement in survival or hospitalisation for patients with COVID‐19 for approved drugs such as ivermectin,43 hydroxychloroquine44,45 and azithromycin46 and for dietary supplements such as vitamin C,47 vitamin D48 and zinc.49 Outside of research studies, these treatments are not recommended for use in the treatment of patients with COVID‐19 in Australia.14"
Embarrassingly for Australia, given the use of ivermectin for COVID-19 got its start from cherry picked Australian research news.com.au/lifestyle/healt... I note ivermectin just bombed out again in a US double-blinded, randomized, placebo-controlled platform trial during a period of Delta and Omicron variant predominance, which included 1, 591 adult outpatients with COVID-19. https:/jamanetwork.com/journals/jama/fullarticle/2797483
The US National Institutes of Health (NIH) has chosen the antiviral drug Paxlovid as the first treatment it will study in patients with long COVID/post-acute sequelae of COVID (PASC).
The study will test the hypothesis that persistent infection is the reason for long Covid.
The phase 3 study will have two groups:
1) normal Paxlovid dosage (two of nirmatrelvir and one of ritonavir) twice daily for 15 days
2) placebo dosage (two placeboes and one of ritonavir) twice daily for 15 days
It is listed on clinicaltrials.gov but is 'not recruiting' yet. Eligibility criteria is detailed in the clinicaltrials.gov entry:
Meanwhile, we also await findings about whether a longer course of Paxlovid (eg 10 days instead of 5) might be preferable for some people immediately post-infection.
Remember, Paxlovid interacts with several other medications (see links provided earlier), so it may not be suitable for some people.
A yet-to-be-peer-reviewed article about a systematic review of the effectiveness of Evusheld for prophylaxis of COVID-19 in immunocompromised patients has been released online ahead of print this week. The review was undertaken by a research team led by the University of Birmingham with academics from King’s College London and the UK Health Security Agency.
"17 clinical studies were included, comprising 24,773 immunocompromised participants of whom 10,775 received Tixagevimab/Cilgavimab. Most studies reported clinical outcomes during the SARS-CoV-2 Omicron wave. Six studies compared a Tixagevimab/Cilgavimab intervention group to a control group."
The clinical effectiveness of prophylactic Tixagevimab/Cilgavimab against COVID-19 was:
40.47% breakthrough infection
69.23% hospitalisation
87.89% ICU admission
"For prevention of all-cause and COVID-19-specific mortality, overall clinical effectiveness was 81.29% and 86.36%, respectively."
It "demonstrates the clinical effectiveness of prophylactic Tixagevimab/Cilgavimab at reducing COVID-19 infection, hospitalisation, ITU admission and mortality for immunosuppressed individuals. It is important that ongoing larger-scale and better-controlled real world studies are initiated and evaluated to provide ongoing certainty of the clinical benefit of prophylactic antibody treatment for immunocompromised patients in the face of new variants."
The BMJ has a related article about this research, highlighting the effectiveness of Evusheld while commenting on some of the limitations of the analysis.
"The authors acknowledged limitations of the analysis, including that the real world studies differed in quality, did not have perfect controls, and comprised different groups of patient. And while most studies reported clinical outcomes during the omicron wave, the authors noted that the original Provent licensing study—the only one they scrutinised that included a randomised controlled trial—was performed before the recent waves driven by the omicron variants."
Regarding the current situation in the UK where Evusheld is not yet available on the NHS, the article states:
"A spokesperson for the Department of Health and Social Care for England said that the government would not be procuring any doses “at this time.” They said that the UK National Institute of Health and Care Excellence had begun its appraisal of Evusheld and that should the treatment prove to be clinically and cost effective “it will be made available on the NHS in the usual way.”
As reported elsewhere, EVUSHELD can be obtained privately in the UK but at a cost of around £1,000 per dose (£1,200 including VAT).
Some places are also using EVUSHELD for the treatment of symptomatic disease caused by SARS-CoV-2.
According to the CLL Society's latest Covid-19 update about the situation in the US, "the preliminary data indicate that Evusheld will no longer be effective against the following variants: BA.4.6, BA.2.75.2, BQ.1, BQ.1.1, BF.7, XBB. These six variants together made up over 55% of cases nationwide as of November 4th."
"While the nationwide average of BA.5 is now only 39.2%, there are significant regional differences in the percentage/prevalence of all the variants of concern . . . "
"...at this time CLL Society still believes that receiving Evusheld and Bebtelovimab is worth obtaining for those who are eligible until the FDA and CDC determine that they are no longer effective!"
In Victoria, Australia, with another Covid-19 wave starting, the Chief Health Officer, Brett Sutton, today reminded people of the six things they can do to help protect themselves and others against Covid-19:
1. Be in well-ventilated spaces indoors - open doors and windows, use fans/HEPA filters
2. Wear a good mask, especially where you can't ensure good ventilation
3. Get tested if you suspect you might have Covid-19
4. If positive, isolate at home until you are no longer infectious
5. If eligible, access treatments to protect against severe illness
6. Be up to date with any Covid-19 vaccine you are eligible to receive
On 16 November 2022, NICE (the National Institute for Health and Care Excellence) in the UK released for public consultation a statement outlining its draft guidelines for Covid-19 treatment,
"NICE has been asked to review the clinical and cost-effectiveness of medicines currently being used in the NHS to treat COVID-19. The appraisal is about routine commissioning of these medicines and does not address their use in exceptional (i.e. pandemic) circumstances.
Although much of the clinical evidence available to the independent committee was based on studies done before the emergence of the Omicron variant, and is therefore uncertain, nirmatrelvir plus ritonavir, tocilizumab and baricitinib are recommended because there is some evidence suggesting they are effective in treating COVID-19. These treatments were found to be cost effective."
"Helen Knight, interim director of medicines evaluation at NICE, said: “Our task has been to evaluate the clinical and cost-effectiveness of treatments for COVID-19, many of which are currently being made available in England under interim UK-wide pandemic-specific access arrangements. In doing so we need to strike a balance between the effectiveness of a treatment and the best use of public funding as we come out of the pandemic, to ensure the NHS can continue to deliver maximum value to the taxpayer."
According to the draft guidelines, the only recommended treatment for those with Covid-19 who do not require hospitalisation would be Paxlovid. There are currently "no technologies recommended' for those hospitalised without supplemental oxygen. Tocilizumab and Baricitinib would be recommended for those hospitalised who require supplemental oxygen.
"Several other medicines are not recommended at this stage. However NICE stands ready to work with companies and NHS England to look for solutions during the public consultation."
The NICE statement concludes: "The recommendations published today are draft and could change following public consultation. Until NICE publishes its final guidance, access to COVID medicines will continue to be guided by the published UK-wide clinical access policies agreed by the UK Chief Medical Officers. Once published, the final guidance will inform routine commissioning decisions for these treatments."
The latest CLL Society Covid-19 update about the situation in the US states: "The most concerning variants in the US remain to be BQ.1 and BQ.1.1, since they are showing the most marked growth advantage over other variants, and both evade Evusheld and Bebtelovimab. Bebtelovimab is often reserved to treat those who are at high-risk of developing severe COVID-19 due to either not being able to take Paxlovid or whose symptoms are progressing despite already being on Paxlovid."
"It’s great news that Paxlovid and Remdesivir are still very effective antivirals and are holding up well against all current variants of concern. However, keep in mind that Paxlovid must be started within five days of symptom onset. So, test early and often if you have known exposure or symptoms occur (preferably obtaining a more sensitive PCR test) so you can qualify for these treatments should you test positive."
Eric Topol has been maintaining a commentary on Covi-19 through a weekly update which, this week, gives a good indication of where things are currently situated in terms of the BQ.1.1 variant that is circulating in many countries. Topol concentrates on its prevalence in the US. This week's newsletter also has some good information about the BA.5 bivalent vaccine (which isn't available everywhere).
Also in the news this week, is a report by The Lancet Covid-19 Commission's Task Force on Safe Work, Safe School, and Safe Travel titled "Proposed Non-infectious Air Delivery Rates (NADR) for Reducing Exposure to Airborne Respiratory Infectious Diseases"
See the following post for an update about some research that shows that COVID-19 is not 'just a respiratory infection' but that, for some, it increases the risk of associated medical events beyond the initial COVID-19 illness:
As well as the article referenced in that post, there was also a good article in the latest edition of Insights+ (Issue 46, 28 October 2022) on the topic of long COVID. It is an edited version of a submission presented by Dr Benjamin Veness, co-founder of Health Care Workers Australia and a founding member of OzSAGE, to an Australian House of Representatives Standing Committee on Health, Aged Care and Sport that will inquire into and report on long COVID and repeated SARS-CoV-2 infections. This submission advocates for improved healthcare worker and patient safety from COVID-19.
"LONG COVID is a syndrome that follows some cases of COVID-19, ranging from very mild acute COVID-19 disease to the most severe forms."
"The most effective way to prevent long COVID is to prevent COVID-19. A primary objective of the Australian health response to COVID-19 ought therefore be to minimise the number of cases of COVID-19, as opposed to merely aiming to minimise severe acute disease and death."
"Regard must be paid to the social determinants of health, including the ability of individuals to access effective risk mitigants for an airborne virus such as SARS-CoV-2."
BEBTELOVIMAB IS NOT CURRENTLY AUTHORISED FOR EMERGENCY USE IN ANY US REGION
This week, the FDA announced that bebtelovimab is not currently authorised for emergency use in any US region" because it is not expected to neutralize Omicron subvariants BQ.1 and BQ.1.1". BQ.1 and BQ1.1 currently account for "above 50% [of cases] in all individual regions but one, and data shows a sustained trend of increasing prevalence across all regions."
The statement lists other treatments which could be considered instead, including Paxlovid, Veklury and Lagevrio .
"In addition, COVID-19 convalescent plasma with high titers of anti-SARS-CoV-2 antibodies is authorized for the treatment of COVID-19 in patients with immunosuppressive disease or receiving immunosuppressive treatment, in inpatient or outpatient settings."
There's more information about the use of convalescent plasma (CCP) in severely immunocompromised patients in this National Institutes of Health article:
It states: "Evidence to support the use of CCP for the treatment of COVID-19 in patients who are immunocompromised is limited."
"Despite the absence of definitive evidence, there is a physiologic rationale for the use of SARS-CoV-2 antibody-based therapies in patients who are immunocompromised. For example, these patients are at risk of having reduced antibody responses to SARS-CoV-2 infection and COVID-19 vaccination, having suboptimal control of viral replication, and progressing to severe disease."
"Under the revised EUA issued on December 27, 2021, CCP is authorized for the treatment of COVID-19 in nonhospitalized or hospitalized patients who have immunosuppressive disease or are receiving immunosuppressive treatment."
". . . the Panel has concluded that there is insufficient evidence for a definitive recommendation. However, given the need for treatment of COVID-19 in people who are immunocompromised, some Panel members would use CCP in certain situations."
"When considering the use of CCP in patients with a history of severe allergic or anaphylactic transfusion reactions, consultation with a transfusion medicine specialist is advised."
In October, 2021, an article cautioned that the use of convalescent plasma in CLL patients requires careful follow up and may not lead to immunity or complete viral elimination:
"This case report was published in the British Journal of Haematology.“This case highlights that long-term follow-up of such patients is important because combined therapy with remdesivir and convalescent plasma may not lead to immunity or complete viral elimination,” noted the authors."
This week, a study posted to bioRxiv gave some updated information about convalescent plasma's effectiveness against Omicron variants, including BQ1.1:
"Conclusions: In summary, boosted VaxCCP neutralized more than 95% of SARS-CoV-2 Omicron BQ.1.1, BF.7, and XBB. Samples collected within a six-month window from boosted individuals without prior infection had half the nAb levels as VaxCCP specimens. Taken together, boosted VaxCCP could be a viable substitute for anti-SARS-CoV-2 mAbs for passive immunotherapy of IC patients. The researchers suggested revising guidelines to include boosted VaxCCP for COVID-19 treatment in IC patients."
I don't think CLL is specifically mentioned in the study.
The European Medicines Agency's Emergency Task Force released a statement about Evusheld on 9 December 2022.
It "cautioned that monoclonal antibodies currently authorised for COVID-19 are unlikely to be effective against emerging strains of SARS-CoV-2."
"Although it is not yet known to what extent the reduced neutralising activity translates into reduced benefits for patients, healthcare professionals will need to consider alternative treatments, especially if subvariants such as BQ.1 and BQ.1.1 become prevalent.
Antiviral treatments such as Paxlovid (nirmatrelvir / ritonavir) and Veklury (remdesivir), which have different mechanisms of action, are expected to retain their activity against the emerging strains. These treatments are approved in the EU for patients with COVID-19 who do not require supplemental oxygen and are at increased risk of their disease progressing to severe COVID-19.
The ETF therefore encourages EU Member States to ensure that healthcare professionals have access to these antiviral treatments for patients at increased risk of severe COVID-19."
Additional evidence in favour of receiving a bivalent vaccine booster against SARS-CoV-2 and COVID-19 infection was published on 21 Dec 2022 in the New England Journal of Medicine.
Although the study was small and had some limitations, the finding was that "These serologic data show an overall neutralization benefit with bivalent booster immunizations."
Check the eligibility in your country to receive a bivalent booster and get up-to-date if you satisfy the criteria. Unfortunately, it's not currently possible for those who have already received a primary course (of three vaccines for the immunocompromised) plus two vaccine boosters to receive a bivalent in Australia.
Neutralizing Responses against the WA1/2020 Strain and Omicron Subvariants
UPDATE ABOUT COVID-19 TESTING - ADVICE ABOUT PCR TESTS, RAPID ANTIGEN TESTS AND HOME RAPID PCR TESTS
This week, the CLL Society published an article that answers many questions you might have about COVID-19 testing. It provides up-to-date advice about how to get the most from each type of testing and explains when it might be more appropriate to use one type of test rather than another.
Written by CLL Nurse, Robyn Brumble, MSN, RN, it's for a US audience and provides update about home rapid PCR testing which isn't yet available in many places. However, it's encouraging that this type of testing is starting to be available more widely and, hopefully, that will mean it will become more affordable, too. The article also provides information about Rapid Antigen Tests and PCR testing which will be helpful wherever you are located. Here are some of the questions about those tests that are answered in the article:
What Are the Differences Between the Two Types of COVID-19 Tests?
"PCR (molecular) tests are ideal for those who are pre-symptomatic or who are just beginning to have symptoms because they can identify COVID-19 at an extremely low viral level which allows for earlier detection.
When someone has a POSITIVE antigen test result, this means they are very likely to be infected. But it is important to know that this type of test has a very high propensity of FALSE NEGATIVE test results! So, if you are symptomatic and take this type of test you should continue to isolate until you can obtain a PCR test and/or keep repeating the antigen tests every 48 hours until you have taken at least three of them in a row."
When Should a Certain Type of Test Not Be Used?
"PCR (molecular) tests should not be used to determine how long you are still infectious after it has been determined that someone has been infected.
. . . antigen tests should not be considered a reliable tool for diagnosing COVID-19, especially in those who are not symptomatic or early on in their infection."
What Type of COVID-19 Test is the Most Reliable?
"Without a doubt, the most reliable is going to be a PCR test."
Are Antigen Tests Ever a Good Tool for Testing?
"Yes, absolutely. They are of particular importance for determining when an individual is no longer shedding the virus AFTER a diagnosis of COVID-19 has been confirmed.
Whenever using a COVID-19 antigen test you should always repeat testing following a negative result whether you have symptoms or not, to reduce your risk of a false negative test result.
If you have a negative antigen test result, it is recommended to test again 47 hours after the first negative test and then again 48 hours after the second negative test for a total of at least three antigen tests.
You can still consider yourself infectious until you have received TWO CONSECUTIVE negative antigen tests that were taken 24 hours apart."
My Antigen Tests Have Expired, Can I Still Take Them?
"Perhaps. Typically, the recommendation would be to not use COVID-19 Tests that are beyond the expiration date printed on the box. However, the FDA has extended many of the expiration dates for these test dates."
Australian CLL patients who have been waiting for the updated vaccination recommendations from ATAGI that have been promised since the start of the year will be disappointed with today's update that still doesn't give those of us who have previously taken every opportunity to be vaccinated the chance to receive a bivalent booster.
Those, like me, who followed government advice and haven't had their vaccination schedule interrupted with infection or CLL treatment, will have previously received five vaccines, none of them bivalent, with their last vaccine now being up to eight or nine months ago.
Note: Australian CLL Patients who have previously received three or four COVID-19 vaccines may receive the bivalent vaccine as their next vaccine. See the table in the link above for more information.
The FDA is considering switching completely to bivalent COVID-19 vaccines, including for primary series doses, according to briefing documents fda.gov/media/164699/download released ahead of an advisory committee meeting later this week, and the agency is planning to offer an updated booster each fall similar to the flu vaccine.
On Thursday 26th January, the Vaccines and Related Biological Products Advisory Committee (VRBPAC) will vote on whether to harmonize primary series and booster doses of all COVID-19 vaccines to a single bivalent composition containing components targeting BA.4/5 and the original SARS-CoV-2 strain.
This week, on 30 Jan 2023, the WHO decided to extend the COVID-19 pandemic's status as a public health emergency of international concern (PHEIC) while anticipating that it may be lifted later this year.
In its public statement, it highlights the ongoing toll the virus is having on individual health and health systems and outlines some of the challenges to be overcome during this next transition phase in the pandemic.
Although there is only scant reference to the particular needs of the immunocompromised in the statement, it does outline seven recommendations of a more general nature. They are:
1. Maintain momentum for COVID-19 vaccination to achieve 100% coverage of high-priority groups guided by the evolving SAGE recommendations on the use of booster doses. States Parties should plan for integration of COVID-19 vaccination into part of life-course immunization programmes.
2. Improve reporting of SARS-CoV-2 surveillance data to WHO. Better data are needed to: detect, assess, and monitor emerging variants; identify significant changes to COVID-19 epidemiology; and understand the burden of COVID-19 in all regions.
3. Increase uptake and ensure long-term availability of medical countermeasures.
4, Maintain strong national response capacity and prepare for future events
5. Continue working with communities and their leaders to address the infodemic and to effectively implement risk-based public health and social measures (PHSM).
6. Continue to adjust any remaining international travel-related measures based on risk assessment, and to not require proof of vaccination against COVID-19 as a prerequisite for international travel.
7. Continue to support research for improved vaccines that reduce transmission and have broad applicability, as well as research to understand the full spectrum, incidence and impact of post COVID-19 condition, and to develop relevant integrated care pathways.
UPDATE RE PAXLOVID and LAGEVRIO/Molnupiravir in the US: The FDA has announced that doctors and pharmacists can now prescribe these treatments to some patients without a positive test for Covid-19.
The Emergency Use Authorization (EUA) still requires that adults and kids 12 years of age and older have a “current diagnosis of mild-to-moderate COVID-19” and that they be at risk of progressing to severe COVID.
The change is that individuals with recent known exposure with signs and symptoms may be diagnosed by their healthcare providers with COVID even if they have a negative test result.
From Endpoint News which contains a link to the reissued authorization letter to Pfizer re Paxlovid: endpts.com/fda-axes-require...
Concerns Lagevrio could spur mutations have dogged its use and, as a result, it's not been widely used, with Paxlovid being preferred where possible.
A new study has been published online as a pre-print. It has not been peer-reviewed but it again highlights issues about molnupiravir saying that some patients might not fully clear SARS-CoV2 infections, with the "potential for onward transmission of molnupiravir-mutated viruses".
Yesterday, the CDC in the US released its Morbidity and Mortality Weekly Report (MMWR) which states that "Bivalent COVID-19 booster doses protected against infection and death during BA.4/BA.5 circulation. All eligible persons should get 1 bivalent booster dose ≥2 months after their COVID-19 primary series or last monovalent booster dose."
"Bivalent booster recipients in 24 U.S. jurisdictions had slightly higher protection against infection and significantly higher protection against death than was observed for monovalent booster recipients or unvaccinated persons, especially among older adults."
"For the best protection against severe COVID-19, all persons should stay up to date with recommended COVID-19 vaccination, including receipt of a bivalent booster by eligible persons."
On 26 Jan 2023, the US announced that Evusheld is not currently authorised for emergency use.
"Data show Evusheld is unlikely to be active against certain SARS-CoV-2 variants. According to the most recent CDC Nowcast data, these variants are projected to be responsible for more than 90% of current infections in the U.S. This means that Evusheld is not expected to provide protection against developing COVID-19 if exposed to those variants."
On 16 Feb 2023, the UK announced its decision not to provide Evusheld on the NHS, saying "Evusheld is unlikely to prevent infection with most of the variants circulating in the UK now and in the near future".
NICE says evidence that COVID-19 treatment Evusheld is effective in protecting vulnerable adults against current variants is lacking as it announces new rapid update process for COVID-19 medicines - nice.org.uk/news/article/ni...
Stocks of Evusheld available through the National Medical Stockpile (NMS) in Australia expired on 31 Dec 2022 and, at this stage, "it is highly unlikely that further stock will be available from the NMS in 2023". See the following post reply for more details:
Recently, there has been mixed news regarding at-home testing for COVID-19.
On 24 Feb 2023, the FDA authorised the Lucira home-testing product. However, on the same day, the company that produces it filed for bankruptcy. It's hoped a buyer will restart manufacturing it.
"Lucira is seeking a strategic or financial partner for the resumption of manufacturing and development of additional home diagnostic products."
Accurate, affordable, quick testing remains a priority for the immunocompromised who need to be able to identify quickly if they've been infected with SARS-CoV-2 (or, indeed, other viruses) so they can access antiviral treatment in a timely manner.
Research continues on other products. This week, there was news about Caltech research conducted in the laboratory of Niles Pierce. The researchers there have "developed a new at-home test for COVID-19 that is more than twice as sensitive as current state-of-the-art antigen tests. While the test was developed for COVID-19, the technology can be used as a platform for designing tests to detect other pathogens as well."
"In the new work, researchers in the Pierce lab have combined the ease of an instrument-free at-home test with amplification techniques. To do so, they utilized a technology called hybridization chain reaction (HCR), which boosts the signal of the reporter molecules. With the new test, every viral protein captured then grows a long tail of DNA. This DNA does not encode for anything biological but rather acts as a specially designed scaffold upon which many colorful reporter molecules can attach. In this way, each viral particle emits a much “brighter” signal. In a skillful engineering process, the team designed the amplified test so that each step occurs sequentially in a disposable device about the size of a playing card without user intervention.
The team compared their new HCR test with five commercially available antigen tests. Their test was 2.5 times more sensitive than the best at-home test and 100 times more sensitive than the worst, despite not having access to the proprietary antibodies that are used in the commercial tests."
"The team plans to continue improving both tests and connect with industry partners to bring the tests to the market."
"NIH-Funded Study Suggests Need to Boost CD8+ T Cell Response After Infection"
The National Institute of Health (NIH) in the US has provided an update about research it co-funded with the National Institute of Allergy and Infectious Diseases (NIAID) which suggests that people need to boost their CD8+ T-cell response after being infected with SARS-CoV-2.
The investigators "designed a very sensitive tool to analyze how immune cells called CD4+ T cells and CD8+ T cells respond to SARS-CoV-2 infection and vaccination. These cells coordinate the immune system’s response to the virus and kill other cells that have been infected, helping prevent COVID-19. The tool was designed to identify T cells that target any of dozens of specific regions on the virus’s spike protein as well as some other viral regions."
They studied CD4+ and CD8+ T-cell responses in blood samples from three groups of volunteers:
- never infected with SARS-CoV-2 and received 2 x Pfizer BioNTech COVID-19 vaccine doses
- previously infected with SARS-CoV-2 and received two doses of the vaccine.
- had COVID-19 and were unvaccinated
They found that vaccination of people who had never been infected with SARS-CoV-2 "induced robust CD4+ and CD8+ T-cell responses to the virus’ spike protein. In addition, these T cells produced multiple types of cell-signaling molecules called cytokines, which recruit other immune cells—including antibody-producing B cells—to fight pathogens."
"However, people who had been infected with SARS-CoV-2 prior to vaccination produced spike-specific CD8+ T cells at considerably lower levels—and with less functionality—than vaccinated people who had never been infected. Moreover, the researchers observed substantially lower levels of spike-specific CD8+ T cells in unvaccinated people with COVID-19 than in vaccinated people who had never been infected."
"Taken together, the investigators write, these findings suggest that SARS-CoV-2 infection damages the CD8+ T cell response, an effect akin to that observed in earlier studies showing long-term damage to the immune system after infection with viruses such as hepatitis C or HIV. The new findings highlight the need to develop vaccination strategies to specifically boost antiviral CD8+ T cell responses in people previously infected with SARS-CoV-2, the researchers conclude." (my emphasis)
CLL changes the CD4:CD8 ratio by boosting CD8 T cells, so we need specific CLL-related research on SARS-CoV-2 and T cell changes.
FDA UPDATE ABOUT COVID-19 VACCINATION: 18 APRIL 2023
"Individuals 65 years of age and older who have received a single dose of a bivalent vaccine may receive one additional dose at least four months following their initial bivalent dose.
Most individuals with certain kinds of immunocompromise who have received a bivalent COVID-19 vaccine may receive a single additional dose of a bivalent COVID-19 vaccine at least 2 months following a dose of a bivalent COVID-19 vaccine, and additional doses may be administered at the discretion of, and at intervals determined by, their healthcare provider."
I was just going to post this, but you beat me to it. 😀😀 Thank you for being on top of it!
"The FDA’s decision will now be handed off to the Centers for Disease Control and Prevention [CDC], which has scheduled a meeting with its panel of outside advisers for Wednesday [today]. If the panel votes in favor of the additional boosters, and Dr. Rochelle Walensky, director of the CDC, signs off, immunizations could begin immediately." nbcnews.com/health/health-n...
I reached out to my GP's office, who said they couldn't give me another booster until the CDC approves it. They suggested I ask my oncologist for a prescription, which would circumvent the process. My plan is to give it another couple days to see if the CDC comes through, and if they don't, I'll ask my CLL specialist for the prescription.
Happy for you to write a separate post. 😀 This post was written as a reference post for our pinned post collection and then, as things kept changing with COVID0-19, it grew beyond what was originally intended. It's been on my mind to write something to replace it for our pinned post section but I thought I'd wait until the dust settles a bit and we have some more certainty about Covid vaccination schedules, prophylactic availability and treatments.
Thanks for the updates. Does anyone know if the"updated" bivalent vaccine referred to is the same as what's been available since last fall, or is actually updated for the newest variants?
Also how long is the shelf life of the updated Moderna and Pfizer vaccines?
There's been no change to the formulations approved for this rollout. The next CDC announcement is planned around June for the FALL 2023 vaccination period and it may include changes to the formulations if they're deemed necessary.
The Pfizer bivalent BA.4/5 vaccine has a shelf life of 18 months if stored frozen at –90°C to –60°C. Shelf life shortens when the vaccine is stored at higher temperatures. The CDC storage and handling guidelines for the Pfizer BioNTech vaccine gives specific details: cdc.gov/vaccines/covid-19/i...
The Moderna bivalent BA.4/5 vaccine lasts longest stored at –50°C to –15°C and cannot be stored below –50°C. Again, the shelf life shortens when the vaccine is stored at higher temperatures. The CDC storage and handling guidelines for the Moderna vaccine gives specific details:
There has been considerable mis/disinformation about the risk of cardiovascular, more specifically thromboembolic events (blood clots, strokes, heart attacks) from COVID-19 vaccinations, despite evidence from reputable sources showing the risk from a COVID-19 illness is much higher. This large study adds to the risk vs reward evidence for those uncertain about COVID-19 vaccinations/boosters.
Payne AB, Novosad S, Wiegand RE, et al. Effectiveness of Bivalent mRNA COVID-19 Vaccines in Preventing COVID-19–Related Thromboembolic Events Among Medicare Enrollees Aged ≥65 Years and Those with End Stage Renal Disease — United States, September 2022–March 2023. MMWR Morb Mortal Wkly Rep 2024;73:16–23. DOI: dx.doi.org/10.15585/mmwr.mm...
Thromboembolic complications of COVID-19 include ischemic stroke, venous thromboembolism, and myocardial infarction. COVID-19 vaccines are effective in preventing severe outcomes, including hospitalization and death.
What is added by this report?
During September 2022–March 2023, receipt of bivalent mRNA COVID-19 vaccine was 47% effective in preventing thromboembolic events among immunocompetent persons aged ≥65 years and 51% effective among adults aged ≥18 years with end stage renal disease (ESRD) receiving dialysis, compared with receipt of the original monovalent vaccines alone.
What are the implications for public health practice?
COVID-19 vaccines helped provide protection against COVID-19–related thromboembolic events. Persons aged ≥65 years and adults with ESRD should receive all recommended COVID-19 vaccine doses to prevent COVID-19–associated complications, including thromboembolic events.
Addendum: The role of COVID-19 vaccines in preventing post-COVID-19 thromboembolic and cardiovascular complications
Results The study included 10.17 million vaccinated and 10.39 million unvaccinated people. Vaccination was associated with reduced risks of acute (30-day) and post-acute COVID-19 VTE, ATE and HF: for example, meta-analytic sHR of 0.22 (95% CI 0.17 to 0.29), 0.53 (0.44 to 0.63) and 0.45 (0.38 to 0.53), respectively, for 0–30 days after SARS-CoV-2 infection, while in the 91–180 days sHR were 0.53 (0.40 to 0.70), 0.72 (0.58 to 0.88) and 0.61 (0.51 to 0.73), respectively.
Conclusions COVID-19 vaccination reduced the risk of post-COVID-19 cardiac and thromboembolic outcomes. These effects were more pronounced for acute COVID-19 outcomes, consistent with known reductions in disease severity following breakthrough versus unvaccinated SARS-CoV-2 infection.
As covered by The Guardian
Covid vaccines cut risk of virus-related heart failure and blood clots, study finds
Researchers say jabs substantially reduce for up to a year the chances of serious cardiovascular complications
Astra Zeneca has published a press release about the SUPERNOVA Phase III COVID-19 pre-exposure prophylaxis (prevention) trial saying that it showed that "sipavibart (formerly AZD3152), an investigational long-acting antibody (LAAB), demonstrated a statistically significant reduction in the incidence of symptomatic COVID‑19 compared to control (tixagevimab/cilgavimab or placebo) in an immunocompromised patient population." astrazeneca.com/media-centr...
"COVID-19 still represents a significant and disproportionate risk for immunocompromised patients, with infection often leading to serious and protracted illness. By delivering infection-fighting antibodies directly to patients who often don’t respond adequately to vaccines, the data support that sipavibart has the potential to provide much-needed protection against COVID-19 in this highly vulnerable population.”
"Sipavibart was designed to provide broad and potent coverage across Omicron and ancestral viral variants by neutralising spike protein interaction with the host receptor ACE2."
There's little detail in the press release in terms of data which "will be presented at a forthcoming medical meeting. AstraZeneca is in dialogue with regulatory authorities on potential authorisation or approval pathways."
Note there's no forward projection of sipavibart's likely efficacy against the so called "FLiRT" variants that are now circulating or still emerging. Whether that will be provided when the data is released is hard to tell.
Talking of the protection one can expect from a previous infection against newer variants, a resource recently released by Johns Hopkins, answers the question "Do people who recently had COVID have any protection against infection from FLiRT variants?" It says:
"A JN.1 infection should provide pretty strong protection against all the FLiRT variants. The difference between JN.1 and these variants is only one or two amino acid changes, so there are still a lot of other places antibodies can bind to. Infection from a variant older than JN.1 is less likely to offer as much protection." publichealth.jhu.edu/2024/w...
In the past two weeks, there have been a couple of promising news items about the development of universal COVID-19 antibodies and a vaccine candidate which may provide longer immunity.
The first news comes from a press release about research efforts to develop universal COVID-19 antibodies.
'A consortium of scientists at Texas Biomedical Research Institute (Texas Biomed), the University of Alabama at Birmingham (UAB) and Columbia University have developed a promising new human monoclonal antibody that appears a step closer to a universal antibody cocktail that works against all strains of SARS-CoV-2.'
'"This antibody worked against the original SARS-CoV-2 strain, omicron and SARS-CoV, providing strong evidence that this antibody will continue to work against future strains, especially if paired with other antibodies," says Luis Martinez-Sobrido, Ph.D., a Professor at Texas Biomed and co-lead author of the research, which is published as a preprint on bioRxiv.'
'The newly designed antibody, called 1301B7, is a receptor binding domain antibody, meaning it targets a region of the spike protein responsible for enabling the virus to bind and enter a cell. By targeting this region, these antibodies are essentially stopping the virus before they can infect a cell.'
1301B7 has been tested against several variants including the original SARS-CoV-2 and omicron JN.1 variants.
In a Texas Biomedical Research Institute press release, Dr Martinez-Sobrido said that a multi antibody approach may be required, as it is for Ebola and HIV, that targets different regions of the virus.
The team is also interested in vaccines that would be able to induce these types of antibodies meaning that they wouldn't need to be updated as often.
Here's a link to the full press release and to the research article titled 'Potent neutralization by a receptor binding domain monoclonal antibody with broad specificity for SARS-CoV-2 JN.1 and other variants' that appeared in bioRxiv: medicalxpress.com/news/2024... and doi.org/10.1101/2024.04.27....
That brings us to the second piece of news which is about a COVID-19 vaccine that promises longer immunity than current mRNA vaccines.
'Scientists from Monash University and the National University of Singapore have engineered a COVID-19 vaccine that, in pre-clinical models, has shown very long-lasting, protective immunity with a single-shot.'
'“The results that we see in this study are very promising, and we are confident that the work performed in pre-clinical models is highly translatable to humans,” said Associate Professor Sylvie Alonso, Principal Investigator of this study.'
' . . . they monitored the immune responses in pre-clinical models over 21 months, and found no signs of declined immunity. In contrast, it was observed that the quality of the immune response (the neutralising antibody response, in particular), was associated with increased protection over time.'
'We are now evaluating our vaccine candidate as a booster vaccine in mRNA-vaccinated pre-clinical models. We hope to demonstrate that this booster approach will induce long-term protective immunity, and avoid the need of multiple (annual) booster shots.'
'Beyond COVID19, this versatile, rapidly-deployable vaccine platform shows promising potential to be part of the pandemic response against diseases caused by unknown pathogens in the future.'
A research article that appeared in the scientific journal Molecular Therapy explains the use of this "Clec9A-receptor binding domain (RBD) antibody construct that delivers the SARS-CoV-2 RBD to conventional type 1 dendritic cells":
Cheang et al., Single-shot dendritic cell targeting SARS-CoV-2 vaccine candidate induces broad, durable and protective systemic and mucosal immunity in mice, Molecular Therapy (2024), doi.org/10.1016/j.ymthe.202...
For now, it's worth remembering that a "vaccination plus" approach is important to minimise the risk of COVID-19. That includes using the following strategies:
- stay up to date with your vaccinations,
- wear a well fitted respirator in public indoor spaces and crowded outdoor ones
-aim for good ventilation in indoor areas
- monitor indoor CO2 levels where possible and use ventilation to keep the levels low,
- test for infection
- isolate if unwell and,
- if infected and eligible, get antiviral treatment as soon as possible
This cohort study found that both current and former smoking were associated with an increased risk among patients with COVID-19 for hospitalization, ICU admission, and all-cause mortality. These associations remained after adjusting for demographic and comorbidity factors. Specifically, older patients who reported current or former smoking showed a faster progression to all-cause mortality than those who reported never smoking. In addition, cannabis use was associated with an increased risk of hospitalization and ICU admission among patients with COVID-19.
The MedPage Today article summarised the report as follows;
Cannabis use was significantly associated with a greater risk of severe outcomes following a COVID-19 infection, according to a retrospective study that spanned the first 2 years of the pandemic.
Among more than 70,000 patients with a documented case of COVID at a large medical center in the Midwest, use of cannabis was linked with an 80% greater risk of hospitalization and a 27% higher risk for intensive care unit (ICU) admission after an infection, but no difference in all-cause mortality:
Hospitalization: OR 1.80 (95% CI 1.68-1.93)
ICU admission: OR 1.27 (95% CI 1.14-1.41)
Mortality: OR 0.97 (95% CI 0.82-1.14)
The elevated risks for hospitalization and ICU admission were about on par with that of smoking, reported Li-Shiun Chen, MD, MPH, ScD, of the Washington University School of Medicine in St. Louis, and coauthors.
The electronic health record (EHR)-based study, published in JAMA Network Openopens in a new tab or window, also confirmed the established link between tobacco smoking and increased risks for serious outcomes from COVID. That association was observed both in current and former smokers and included a higher risk for mortality.
"There's this sense among the public that cannabis is safe to use, that it's not as bad for your health as smoking or drinking, that it may even be good for you," Chen said in a press releaseopens in a new tab or window. "I think that's because there hasn't been as much research on the health effects of cannabis as compared to tobacco or alcohol."
"What we found is that cannabis use is not harmless in the context of COVID-19," Chen continued. "People who reported yes to current cannabis use, at any frequency, were more likely to require hospitalization and intensive care than those who did not use cannabis."
Content on HealthUnlocked does not replace the relationship between you and doctors or other healthcare professionals nor the advice you receive from them.
Never delay seeking advice or dialling emergency services because of something that you have read on HealthUnlocked.
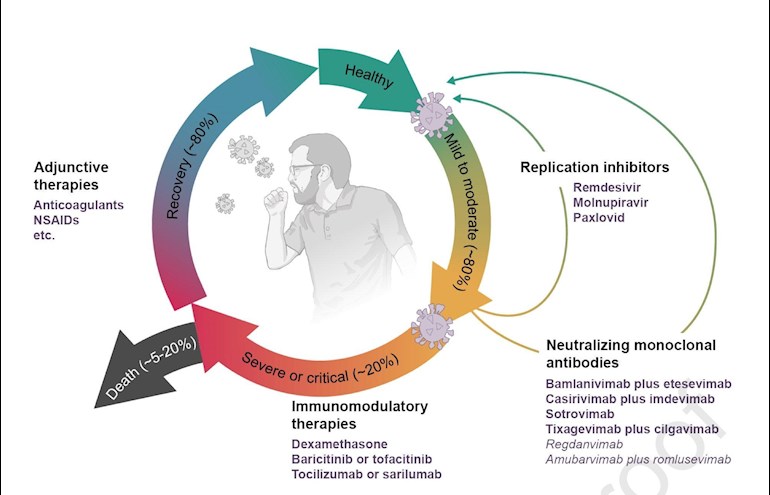

")