Four strategies have been tested in recent years with combinations of ibrutinib with immunotherapy, chemoimmunotherapy, cell therapy, and other targeted therapy. Here, they review the scientific rationale for and clinical outcome of each strategy.
Among these strategies, ibrutinib with targeted agent venetoclax results in high complete response rates and, importantly, high rates of undetectable minimal residual disease. Although they concentrate on ibrutinib, similar combinations are expected or ongoing with acalabrutinib, tirabrutinib, and zanubrutinib, all second-generation BTK inhibitors.
While single-agent ibrutinib was a remarkable addition to the CLL pharmacopeia, results from combinations of ibrutinib and other agents have been even more promising. Particularly, early data from studies of the combination of ibrutinib with other targeted agents, such as venetoclax, show deep responses resulting in high CR rates and, importantly, high rates of undetectable MRD.
This progress is providing us an opportunity to test fixed-duration therapy and an MRD-guided approach to discontinuation of treatment for patients with CLL. Time-limited treatment would be more cost-effective than regimens that must be used continuously until the disease progresses. MRD status and the velocity of attaining remission allow identification of patients with a low risk of relapse who do not require continuation of treatment.
More selective BTK inhibitors, such as acalabrutinib, tirabrutinib, and zanubrutinib, are being tested in similar combinations. Further, the use of combination strategies to target different elements of the pathophysiology of CLL at an early stage may result in lower rates of emergence of drug-resistant clones. Long-term results will provide this long-needed information.
Future investigations will focus on the feasibility of discontinuing ibrutinib combinations after a defined time; the therapeutic benefit of adding a third agent to ibrutinib-containing combinations and the profiling of resistant clones that develop after combination treatment.
A new standard of care for CLL is expected to emerge from these investigations.
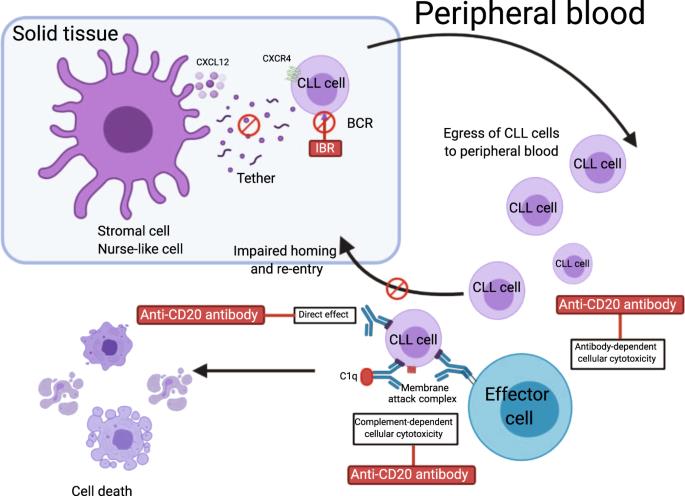
Lots more detail here and some excellent schematics illustrating the dynamics of each approach
Thanks Jackie! This is a great summary paper of where we are now with combination treatments. It should be a pinned post.
Maintenance treatment of CLL was the only practical approach when the new, slow acting, yet acceptable long term toxicity non-chemo targeted therapy treatments, commencing with Ibrutinib, came on the scene. Researchers didn't know how to assess treatment response on maintenance therapies, as only a few on Ibrutinib (10% after 4 years) achieved uMRD.
As the paper highlights, the big breakthrough is moving on from FCR, both in avoiding the associated long term secondary blood cancer risks and most importantly, extending treatment coverage to those older than 65. Given the median age of diagnosis with CLL is 71 and treatment is typically needed years later, this is a huge breakthrough.
So now we are now moving back to the standard CLL treatment paradigm, importantly using non chemo, limited term combination treatments, but I suspect that further research will identify a subset of CLL patients who will be better served by maintenance treatments. This will most likely be those with high risk markers, i.e. complex karyotype with unmutated IGHV, mutated TP-53, 17p-del, NOTCH-1, etc. Thankfully we also now have a growing list of better targeted BTKi therapies with a lower side effect/adverse event profile to better support that group of patients. See: healthunlocked.com/cllsuppo...
I agree, Neil. This is such an encouraging review of where the research has brought us and where we’re heading. Thanks for posting it, Jm954 .
I agree, too, with your feeling, Neil, that mono therapy with a targeted BTKi will still have a role for some people with higher risk CLL. It’s working for me, anyway 😀
Treatment should definitely be targeted based on the FISH, IGHV status and other markers in the future. All the trials should be doing these tests and then reporting results for each segment of the CLL population.
The down side to this is that the trials would need thousands of patients to power the results statistically and could take too long but it might be possible to get some signposting from just a few hundred patients in relatively short time or a huge meta-analysis of all relevant trials could be done.
Thanks for this Jackie.The authors have written the reference book with this one. A systematic review of where we are and how we got here. A good post to save!
I feel that alongside clinical trials, or maybe integrated into them, single cell analysis on small groups of patients could reveal a lot about which mono- and combo treatments are likely to work best on which driver mutations. This kind of detailed and sophisticated time-series analysis is made possible by developments in computational biology, aka bioinformatics. Christian Bock's team has used this approach in CLL, Ibrutinib treatment.
I know what you mean, a lot of data crunching for what. Well, they may not have come up with any specific recommendations but this was a kind of proof of concept. They have demonstrated a way to track CLL treatment dynamics at a new level of biological detail, and I suspect such an approach will be key to personalised therapy.
Although CeMM teams up with other medical researchers, perhaps they need someone like M Hallek to set them some concrete objectives feeding into current clinical trials?
Great post Jackie, bless you. I am on the UK Flair trial on Ibrutinib with amazing results for me. Little side effects all manageable and for the first time in 6 years all my blood measures are in the 'normal' ranges as reported last week at my latest 6 monthly review. Just have some minor surgery on Sunday for latest basal cell carcanoma removals from my head. Will not be long before my head looks more like Krytons from red Dwarf! Keep well and positive everyone.
Content on HealthUnlocked does not replace the relationship between you and doctors or other healthcare professionals nor the advice you receive from them.
Never delay seeking advice or dialling emergency services because of something that you have read on HealthUnlocked.

")