There are lots of us on long term Ibrutinib who have had a good response but still have a small amount of residual disease. I would welcome the chance to add venetoclax to my treatment as in this study which is an important piece of work by Michael J Keating et al.
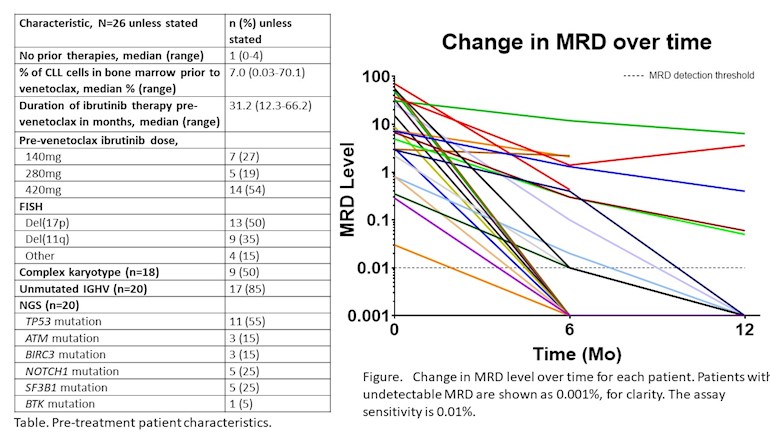
"Patients receiving the BTK inhibitor ibrutinib (ibr) for CLL rarely achieve CR with undetectable MRD (U-MRD) and require indefinite suppressive therapy. This results in a cumulative risk of relapse and also of adverse events leading to drug discontinuation. The risk of relapse is highest in patients with complex karyotype and/or del(17p); some series also suggest increased risk in patients with del(11q) or a persistently elevated β2-microglobulin.
Ven added to ibr in pts with high-risk CLL as consolidation is well tolerated and associated with a high likelihood of achieving U-MRD in BM and CR within 12 months of combination therapy, suggesting that time-limited therapy may be feasible in high-risk CLL. Further follow-up will determine the likelihood of achieving U-MRD at later time points and durability of responses."
Great article. I started ibrutinib over 3 months ago. Dr Wierda told me that he wanted to add Venetoclax in a year but I emailed Dr Thompson and he said that he’d be fully accrued by then. I guess we’ll see.
Thanks for posting, Jackie! This is one of my favorite images. Only one of the 26 lines appears to have a positive slope!
It reminds me of the other I+V abstract you posted where they show U-MRD over time, where it keeps getting better from 12 to 24 months, suggesting that some patients may need more than 12 months of the combo.
I'm hoping to stay on Ibrutinib long enough for this to become the standard of care of this group of patients - high risk with MRD after years of Ibrutinib.
I'm considering a similar approach. Starting on a BTK inhibitor for a year (or two), then delivering a knock-out punch (or icing on the cake) with V or O or V+O after fully taking advantage of the 'compartmental shift phenomenon' of the BTK inhibition.
I mean taking ibrutinib or acalabrutinib for a year or two, since they take a long time to flush out the nodes/spleen (aka compartmental shift phenomenon). The problem with those drugs is that you have to take them continuously to keep the CLL controlled. So I'd rather get CLL under control, then add venetoclax (and maybe obinutuzumab) in an attempt to get rid of any detectable CLL, then stop all drugs.
We don't know yet the optimal sequence or combination to achieve a cure, but we've seen lots of fresh data from the ASH 2019 abstracts. It appears responses on ibrutinib+venetoclax are very good after 12 months, but keep improving up to 24 months. (see the chart here: healthunlocked.com/cllsuppo... )
V+O combo looks great, but would it be even better if it was preceded by a year of ibrutinib? Last year we saw that adding O after a year of ibrutinib seemed better than starting with I+O. healthunlocked.com/cllsuppo...
Thank you for your explanation. I have been on Ibrutinib for a year and half. I just have all the tests done yet again . Blood test, as well as PET scan, looks very well with no enlaged nodes etc. My bone marrow study though shows 30 % of infiltration of small lymphocytes. My Doc, talked briefly with me on the phone and stands behind his previous option for me , which is a stem cell transplant. I am really scared of this procedure and will make an appointment with him after Xmas to discuss my results and other options if any. I want to have nice Holidays and I am posponing the visit until after.I feel great , went back to work on a per diem basis ,but my Onco thinks ,it will not last for a long time. He said"no rush , but we have to talk". My diagnosis is somewhat inconclusive betwen Marginal Zone Lymphoma and CLL . Ibrutinib is my 4 line of treatment .To add to my misery I am TP 53 as well.
That's a tough situation. Have a look at this encouraging ASH 2019 abstract about stem cell transplant for CLL in the era of novel agents:
Allogeneic Stem Cell Transplantation (alloHSCT) for Chronic Lymphocytic Leukemia (CLL) in the Era of Novel Agents
Conclusions: In the largest series of alloHSCT following NAs, data demonstrate that alloHSCT remains a viable curative strategy that can overcome adverse CLL characteristics including TP53 disruption and CK. As many pts treated with ibr and/or ven will progress or be intolerant, alloHSCT should be included in treatment algorithms for appropriate candidates. These data suggest that exposure to 1 vs. ≥2 prior NAs did not impact outcomes, though disease status at time of alloHSCT and HCT-CI are important predictors of PFS. Therefore, decision about proceeding to alloHSCT should consider comorbidities and current depth of response, as well as anticipated depth of response with the therapeutic options remaining. These data may significantly add to development of evidence-based guidelines for alloHSCT in the era of NAs.
Thank you for taking time and find this papaer that you quoted here and gave me the link.I don't think I will go throught that though. The whole thing with its concequences ,side effects is too scary for me. I will see what the Doctors have to say in January when I go to my appointment.
I still have diarrhoea, cramps, joint pain and mouth ulcers. Not all the time but it’s unpredictable and bad enough for me to be reluctant to make plans too far ahead.
It’s different for everyone so don’t let anyone else’s experience put you off Ibrutinib 😊
Jackie, great post. I am sorry to hear that you are still experiencing side effects after 50 months. I hope that pattern changes and that you get breaks from them. And when you do, I hope you can be present to enjoy those pain free moments.
I am unclear as to the difference between U-MRD and CR. Isn’t achieving undetectable minimum residue disease the same as complete remission? What additional information are they looking at that says you are in complete remission other than U-MRD?
You'll see that the marrow assessment is visual with no CLL cells seen for CR.
However, MRD analysis looks at many thousands of cells, much more than by microscopy, to detect CLL cells. If they cannot find any then, depending on the level of sensitivity of the way they are being measured you might be U-MRD4 (<1/10,000) or U-MRD6 (<1/100,000).
Same boat as you Jackie been on ibrutinib 2.5 years doing well and have long wondered if adding v would be beneficial asto preventing relasp and drug resistance in theory by reaching umd and stopping treatment we should be able to go back on I+v as and when cll comes back most consultants mine included seem to still favour mono treatment and I understand that with costs etc but if in the long term we get treatment breaks then this should off set the combination treatments cost
Medics are very cautious (they don't like killing their patients or being sued!) and so we need more studies like this to get the evidence to change it from a trial to standard practice.
We just need to be able to hang on for a few more years
I asked my oncologist about adding Venetoclax to Ibr (3+years) several months ago. He said insurance would not cover both, but that was before Ven was FDA accepted. I plan to ask again.
It’s interesting to me that the insurance companies aren’t all over this. Coz actually a year or two of venetoclax in combo would probably mean you get to stop ibrutinib so be cheaper. But I think the reason they aren’t pushing is coz the data isn’t there. Of course the other question is whether you’d need to continue the ibrutinib or could perhaps cross taper to venetoclax mono or in combo with a CD20 antibody.
At the moment I guess the thought is that if ibrutinib is working why upset the Apple cart? But as data continues to acrue for venetoclax combos MRDU and what will most likely be associated long remissions, I suppose the drive will becomes stronger to do this.
It does seem clear tho that by driving CLL cells out of the lymph nodes and reducing the tumor load and lymphocyte count Ibrutinib therapy is certainly going to be good preparation for venetoclax by making tumor lysis less likely (a similar role the CD20 antibody plays)
I wondered that myself. Look at all the money the companies would save not having to provide unending Ibrutinib!
I saw my doctor today for another bmb. its been a year. and also almost a year of Imbruvica She says she is going to check it for mutations and will add venetoclax within 3 weeks unless the bmb yields something unforeseen. I will add info when available. also although most of you know i have b-pll but am treated as high risk cll
I am a participant in this study at MD Anderson. My bone marrow has gone from 90% to .20% in 10 months. I’m feeling great. I have the 17p deletion. The study is wrapping up and I’m one of the last participants.
Thanks for keeping this great info posts coming Jackie. I am 11q deleted so read this with great interest. After a relatively side effect free year on Ibrutinib i Have gone from 95% infiltration in the bone marrow to undetected which is rare and cynic in me says lets see. (however do not want to rush the next bone marrow biopsy!
That’s a fantastic result with ibrutinib. I presume they want to keep you on it for now yes? There is a mathematical theory that says if you get to MRDU on any treatment you should probably remain on that treatment for the same amount of time longer that it took to get to MRDU if that makes sense. Tho not everyone holds to this idea, it does make some logical sense since as you say just because you are MRDU doesn’t mean every cell has been killed yet.
You deserve a good break. So glad things are going so well for you.
True Adrian, the blood results did not quite endorse the biopsy so my consultant suspects they may be a residue but admits to be astonished with the improvement. I am happy to remain on medication. The test will be if at some point they suggest coming off it....
Very good news, indeed, if this means that Venetoclax can get a great outcome if it is added to a BTK inhibitor some time down the track and not just as quickly as it is in the ACE-CL-311 trial, for instance.
Great article but data is lacking for PFS , going MRD negative doesn’t necessarily increase your PFS, the date isn’t out there yet as these trials haven’t been around along enough
Basically why these trials aren’t front line therapy yet.
I think that there is reasonably good evidence that MRDU does increase your chances of a long remission and PFS. Not a guarantee but certainly the field seems to believe that (hence the idea that MRDU patients can be managed without treatment). For sure the evidence is strongest for ex-FCR patients where MRDU predicts not just PFS but Overall Survival too. It seems likely that at least some patients who get to MRDU by means other than FCR will also see such similarly super long remissions. Just the maths of it makes sense.
I have seen a couple of people on here mention that their doctor had recently added venetoclax to long term ibrutinib therapy. This seems to be a USA only thing right now though since whilst this add on data is interesting it’s not randomised and indeed there is still not enough V plus I clinical trial data to satisfy regulators anywhere. Payers in the USA are sometimes more willing to allow what doctors call “off label” use than in other countries.
What does seem to be becoming more popular is V plus O or V plus R as a treatment option in its own right. But the data for that is really about relapse refractory patients rather than adding this to patients stable on Ibrutinib. USA and some EU countries will fund VO/VR first line, more countries including the UK will fund it second line.
There has also been a very interesting clinical study ongoing examining combining Acalabrutinib venetoclax and obinituzimab (AVO) for first line treatment. And other new drugs are being looked at in combo with V too.
I am sure that some doctors and patients have also looked more closely on an i individual case by case basis at ongoing ibrutinib treatment when it has gone on for years and there are persistent side effects but no evidence of mutations yet. Probably in some cases they may have decided in individual circumstances to switch to Venetoclax (perhaps most often in combo with O or R). One approach to this would be to simply decide that the Ibrutinib was no longer tolerated and needed to be stopped. It might sometimes with some payers be possible to justify an overlap to allow this switch even if true ongoing combination is not justified by the payer. Or it may be thought in some situations that since V plus O or R are quite toxic to CLL cells it might sometimes be OK to just stop the ibrutinib and move to V plus R/O in the same way you would if I or A absolutely had to be stopped due to major tolerability issues.
There are a couple of points, however. I rather suspect that some doctors are going to still be reluctant to make a change if I or A appears to still be working well. Do we really know for sure that moving to VR or VO is always going to be better? Is there clear enough data yet? Or is it better to keep taking I or indeed A for as long as it still works and then make the jump?
Of course if you do decide to continue I or A monotherapy some might feel that it might make sense to be ready to make the jump at the first hint it is not working rather than wait for a fully fledged relapse. Logic might suggest that if you move to a V combination whilst the lymphocyte count is still low and whilst the nodes are still nice and small thanks to I or A you might hope that you could have a better chance of getting to MRDU than you might if you wait and do that from a higher level. But clearly we don’t know that for certain either.
Everyone is different and this is why it is best for us all to be treated by CLL specialists who can weigh things up with us and help us make the best individual choices for our own situation.
One other major complication at the moment is that V, O and R are all believed to be more likely to cause more immune suppression than A or I early on in treatment initiation. They also tend to require more trips to the hospital and more regular blood tests (especially compared to simply staying on a drug you’ve been on for ages). And clearly the infusions of R and O have to be given over many hours in a clinic.
Therefore in the current COVID19 environment where we need to try and avoid hospitals as much as possible there is a clear sense from many of the CLL specialists that right now is not the time to be making radical changes to treatment unless you absolutely have to.
Indeed many specialists are currently trying to delay starting new treatment in patients if at all possible to help ensure people are in the best possible shape to fight off COVID19 if they do catch it.
And if a new treatment must be started A or I is tending to be reached for. Even In the UK right now we have managed to get a special scheme to allow A to be used first line if treatment can’t be delayed (and this was discussed in the first of the Leukaemia Cares CLL webinars). Patients may find their local centre not able to access that scheme but should still be able to request a second opinion from a site that has access to it for consideration of whether that is appropriate for them. And the longer the current situation continues the more some patients will end up having to start treatment. It is all about risk benefit analysis, and care can be taken to minimise the risk of visiting hospital clinics that are typically much quieter than normal at the moment.
So in summary all this has promise for the future but perhaps less so right now at this precise moment. So for sure bursts of time limited combination treatment are likely to become the best option moving forward to obtain long lasting treatment free remissions, MRDU, and in some cases this might even amount to a complete cure (we don’t have long enough data to know this for sure yet though).
But for now it’s very much don’t rock the boat unless you have to. And determining whether you as an individual should be making any treatment changes now more than ever needs to be the role of a CLL specialist. In the UK you can ask for a second opinion (which could be given over the phone if necessary) In the USA if your insurance won’t allow a second opinion there is a free web consultation service offered by the CLL society.
Content on HealthUnlocked does not replace the relationship between you and doctors or other healthcare professionals nor the advice you receive from them.
Never delay seeking advice or dialling emergency services because of something that you have read on HealthUnlocked.

")