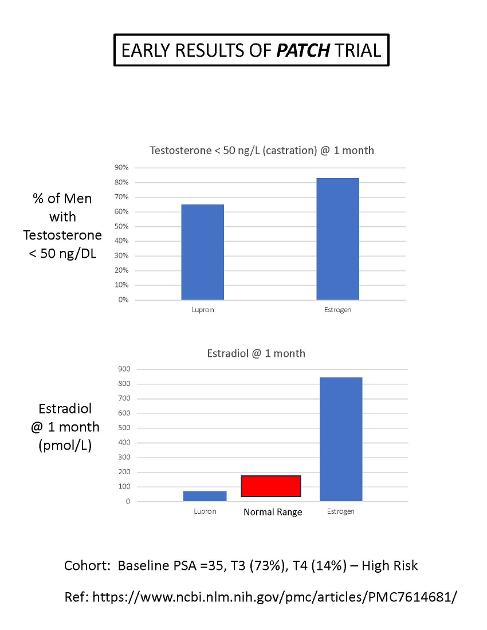
Here's some charts comparing Lupron ADT to transdermal estrogen (TDE) patch therapy for High Risk and Very High Risk men with prostate cancer.
The upper chart shows the percentage of men that have been castrated to a testosterone level < 50 ng/dL after 1 month of treatment. For Lupron, 65% of HR/VHR men are effectively castrated, compared to 83% for men treated with TDE. So, TDE is more effective at castration than Lupron in this study.
The lower chart shows the level of estradiol (picomol/L) after 1 month of treatment. The Lupron level is about 60, while the high-dose level is much higher, about 840 (pico mol/L) (i.e., supra-physiologic).
The normal range for men is from 35 to 175 (pico mol/L). Lupron reduces testosterone, which, in turn, reduces estradiol in the Lupron arm
Bob
Written by
janebob99
To view profiles and participate in discussions please or .
A question I would have is what happens to LH and FSH levels (they should increase) and their potential negative impact on the prostate cancer as both of them have been shown to promote iatrogenesis in the laboratory.
Good question. I guess LH and FSH increase as the level of testosterone goes down (feedback loop). Hopefully, it's a second order effect.
Pituitary tumors are often hormone-secreting adenomas. Extra secretion of prolactin is common, but extra secretion of LH and FSH could also happen. That would be great question for an Endocrinologist.
Have you looked for papers that study levels of FSH and LH on prostate cancer?
Elevated levels of follicle-stimulating hormone (FSH) and luteinizing hormone (LH) can potentially have direct effects on prostate cancer progression, including promoting angiogenesis, which is the formation of new blood vessels to support tumor growth. Here are some ways in which FSH and LH may contribute to angiogenesis in prostate cancer:
1. Hormonal Stimulation: FSH and LH can stimulate the production of testosterone in the testes. Testosterone, in turn, can promote the expression of growth factors and cytokines that stimulate angiogenesis in the tumor microenvironment.
2. Indirect Effects: Elevated levels of FSH and LH may indirectly influence the production of other hormones and growth factors that play a role in angiogenesis. For example, increased androgen signaling due to elevated testosterone levels can promote the expression of vascular endothelial growth factor (VEGF), a key regulator of angiogenesis.
3. Interaction with Tumor Cells: FSH and LH receptors may be present on prostate cancer cells, allowing direct stimulation of these cells by FSH and LH. This direct interaction can lead to the activation of signaling pathways that promote angiogenesis and tumor growth.
4. Inflammatory Response: FSH and LH may also contribute to the inflammatory response in the tumor microenvironment, leading to the release of pro-angiogenic factors and the recruitment of immune cells that support angiogenesis.
5. Therapeutic Implications: Targeting FSH and LH signaling pathways, either through hormonal therapies or other targeted approaches, may help inhibit angiogenesis and limit tumor growth in hormone-dependent prostate cancer.
Overall, the relationship between FSH, LH, angiogenesis, and prostate cancer progression is an area of active research, and further studies are needed to fully understand the mechanisms involved. Consulting with a healthcare provider or oncologist for personalized information and treatment options is recommended for individuals with prostate cancer.
Fascinating! You have good reason to be concerned.
Did you use ChatGPT 3 or 4?
Have you considered a brain MRI? I've had two, both looking for adenomas in the pituitary...which they found on the second MRI. It might show the presence of an hormone-secreting adenoma...
I believe I read a figure like 20% incidence of micro adenomas. Most of no consequence discovered incidentally at autopsy.
I just asked AI. At least I haven’t lost all my memory!
“ Pituitary microadenomas are small tumors in the pituitary gland that are less than 10 millimeters in diameter. They are quite common and are often discovered incidentally during brain imaging studies for unrelated conditions.
The incidence of pituitary microadenomas varies widely in different studies, but it is estimated that they may be present in up to 10-20% of the general population. However, many of these tumors do not cause any symptoms and do not require treatment.
Symptomatic pituitary microadenomas, which produce symptoms either due to hormone overproduction or due to pressure on surrounding structures, are much less common. The incidence of clinically significant pituitary adenomas (both microadenomas and macroadenomas) is estimated to be about 77.6 per 100,000 individuals, according to a study published in the Journal of Clinical Endocrinology and Metabolism.
As with any medical condition, the incidence can vary based on factors such as age, sex, and population studied. It's always best to consult with a healthcare provider for information tailored to your specific situation.“
From AI it appears LH and FSH should fall as well, which would appear to be beneficial in this scenario. The negative feed back involves not only estradiol but also levels of free T, total T, DHT and probably free DHT. So probably results may vary!! Lots of competing possibilities
Personalized medicine?
“the use of transdermal estradiol cream in men could potentially lead to decreased levels of LH and FSH. However, the actual impact on an individual's hormone levels can vary depending on various factors, including the dose of estradiol used, the duration of treatment, and the individual's overall health status. As such, it's always best to consult with a healthcare provider for personalized advice.”
THe decrease in FSH and LH is the primary reason high-dose estrogen castrates men. But, if there is an adenoma secreting FSH and LH, then it might be different.
You may want to AI "primary hypogonadism and FSH and LH"...
I believe the feedback is more complex than estradiol alone. May involve fT, TT, DHT, fDHT, etc. levels as well and may not be the same from person to person. Also age.
Gosh...I don't remember. When you say "dynamic", I assume you are referring to the use of a contrast agent (e.g., gadolinium, Gd)) and then they look at the time dependence of the Gd flow/perfusion. They usually always do Gd contrast now.
Dynamic contrast-enhanced MRI: This is a specific type of contrast-enhanced MRI where images are taken in rapid succession before, during, and after the injection of the contrast material. This allows for the visualization of how the contrast material flows through the blood vessels and tissues over time. Dynamic contrast-enhanced MRI can provide valuable information about the blood supply and vascular characteristics of a pituitary tumor, which can be important in differentiating between different types of tumors and planning treatment strategies.
I understand. A prostate tumor has lots more blood vessels, and it will absorb Gd contrast agent much faster and a greater amount than the surrounding tissue. A plot of GD MRI Signal Intensity vs time will show this effect.
DCE-MRI however, provides the possibility for multiple and quantifiable parameters pertaining to tissue perfusion and microvascular status (9,10). Since its initial presentation the approach has mainly been applied in studies of the myocardium (11), the brain (12-15) and oncological research (11,16-21). Lately, DCE-MRI has also been adopted to examine the peripheral vascular and muscular system.
A typical targeted MRI examination of the pituitary region includes coronal and sagittal small field of view T1 and T1 post-contrast images, as well as dynamic contrast-enhanced coronal images, which are critical for the identification of small microadenomas. T2 weighted sequences are often also included.Jul 18, 2023
Ideally, you should use a 3T MRI machine, which has higher spatial resolution than the older 1.5 T machines. That's a measure of the magnetic field strength (T=Tesla).
Yes, but have found out I need to be cautious. It will outright lie. Wants to please the user. Provide non-existing references, apologize when corrected, later repeat the same error, etc.
I've corrected it many times and its response is typically that I am correct or absolutely correct, to apologize, etc.
Replies tend to be reflect bias. I suspect that is bias of developers, etc. In particular if there are issues that surround political narratives. Subtle but there.
Great tool though. I get more info from it than if I spent months in a medical library. I am cautious but grateful.
It may put many people out of that present work but like all new technologies it will create many other jobs we just can see right now. Just look at computers.
It is common to take standard ADT (e.g. lupron) and low dose estrogen to mitigate the side effects of the ADT. I know of no benefit of using the high-dose estrogen (as used when estrogen is used as a monotherapy) in addition to standard dosage standard ADT. And not EVER heard of the other (mathematical) combination of low-dose ADT with high dose estrogen. That last combination, while mathematically possible is probably a ridiculous protocol.
In a list:
1 Standard ADT alone
2 Estrogen/estradiol alone (not currently Standard of Care in the U.S.)
3 Standard ADT with estrogen as an add-on to mitigate adverse side effects of ADT
4 Estrogen as primary and standard ADT as an add-on (I think this is never used)
Oral estrogen monotherapy was the Standard of Care for 30 years (from 1950 to 1980). It effectively castrates men. Everyone agrees on that point. Oral estrogen was only dropped because it caused blood clots. The newer transdermal estrogen bypasses the Liver and doesn't cause blood clots.
Combining high-dose transdermal estrogen and Lupron ADT would probably reduce testosterone very close to zero (which maximizes survival outcomes), and there would be reduced side effects because of the high estrogen levels. It probably wouldn't hurt. And, at $55/month (estrogel), it's a cheap addition. The only downside is gynecomastia.
The only downside of transdermal estrogen therapy is increased gynecomastia, which can be prevented by radiation treatment (1 session) or tamoxifen. Adding estrogen will remove most of the bad side effects of the Lupron treatment.
It's very common, as high as 60-80% probability. Some breasts will enlarge a little, others a lot. I plan on getting a single dose radiation treatment as prophylaxis before I start Estrogen patch/gel therapy in a few months.
Lupron and Estrogen work the same way, by reducing LH and FSH. Both castrate men effectively. It's dose dependent, though. More estrogen or Lupron causes lower testosterone nadir levels. No one is studying combination therapy, but there could be some positive synergistic effects. Adding Lupron to estrogen will be the same as increasing the estrogen dose, I expect.
From a practical point, Doctors will be more likely to prescribe estrogen if there is also Lupron being prescribed.
My plan is to convince my MO to do the following. I will start initially on high dose estrogen and then monitor the testosterone every 2 weeks for 2 months. Then, if the testosterone does not drop to sub-castrate level (< 10 ng/dL), I will agree to add Relugolix to drop it further. That's my plan that I will present to her in a few weeks. Wish me luck !
That's an excellent idea, and the doctor should approve it, as long as you are on Lupron ADT. There will likely be a synergistic effect, where the additional estrogen will further drop the testosterone to lower sub-castrate levels (which improves survival probabilities a large amount). You should monitor your testosterone levels every 2 weeks for two months, and titrate your estrogen dose to reach < 10 ng/dL. Your doctor will appreciate the T data.
Plus, you will reduce or eliminate most of the bad side effects of ADT when taking supplemental Estrogen.
With complex biological systems you just never know without multiple peer reviewed trials.
BUT
You can avoid high risk low reward scenarios. and opt for low risk high reward scenarios that are off the beaten path.
I think this would be a low risk moderate reward.
The peer reviewed statistical research shows that if you have three bullets to use against an adaptive self replicating agent or organism, you are statistically best off hitting it with all three bullets right away instead of sequentially.
I think that is starting to show up in many modern protocols. Certainly in prostate cancer and I think also with Aids. And probably others. Everyone is using cocktails now adays.
It wasn't that long ago that the standard protocol for prostate cancer was to start off with a weak ADT and then gradually escalate to stronger ADT agents. Now they are mixing chemo plus a cocktail of ADT agents right at the start. At least some are.
Both work the same way regarding castration of men. I don't think there's any data on combining the two treatments. Probably the combo would castrate to close to zero testosterone and reduce bad side effects. It wouldn't hurt.
Is not current SoC, that's why doctors won't prescribe it.
Some men won't do it because of gynecomastia, which is a common side effect.
Breast cancer rates in men increase with estrogen use, but the absolute rate/risk is still very, very low compared to women. Estrogen won't prevent muscle loss and muscle weakness, which is driven by low testosterone.
Overall, the positive effects of high-dose Transdermal estrogen (TDE) greatly outweigh the negative side effects of Lupron. Attached is a chart comparing pros and cons of side effects of TDE.
I've been contacted by many men who use either estrogen patches or gel, and they aren't complaining about it. Professor Wassersug in Canada switched from Lupron to estrogen gel (Estrogel.com) over 20 years ago and he swears by it. His HealthUnlocked name is "Wassersug". He's a great, and well-informed, resource for all things ADT and estrogen.
I plan on using high-dose E-gel for my own treatment, and do a single course of radiation to prevent enlargement of my breasts.
When the PATCH study is published this Fall (I spoke with the lead researcher yesterday), I predict there will be a huge groundswell of support for switching from Lupron to transdermal estrogen. The UK is funding the phase-III clinical trial because they are looking for ways to reduce the cost of their National Health Care system.
I have collected 17 papers on E-therapy and lots of charts/graphs, that I'd be happy to send you. Send me your email in a private message, if you would like them.
I spend 1-2 hours every morning researching articles about prostate cancer. Have been doing that since Nov, 2023, when I was diagnosed with Stage III PCa (PSA 10, PIRADS 5, GS 7, with some ECE, clean PSMA-PET (no spread).
Im 69, still working, and have a Ph.D in Nuclear Engineering and my wife is a RN specializing in diabetes. So, I'm a "doctor', but not a MD. I have had a lot of hormone problems: hypogonadism, hypothyroidism, prolactinemia, and depression, which are all well-treated now.
I absolutely love doing research, and especially enjoy discovering trends from data sets. I hate tables of numbers. I love to make plots from Excel spreadsheets and Powerpoint. One can learn a lot more from graphs than tables.
Thank you for your support!
As to your question, since high-dose estrogen castrates men in the same way that Lupron does, the low testosterone will cause muscle loss and weakness in either cases The only solution is weight training, which many men report helps them a lot to counteract the side effects of Lupron ADT.
After stopping ADT, I recommend that men supplement their testosterone to get it back to normal levels as soon as possible. TRT is safe for Prostate Cancer, and effective at reversing symptoms of ADT.
My T has been consistently <3.0 using three .1mg patches changed weekly. The reason I’m using three is because that’s the number used in the PATCH trial. I’ve considered using fewer but why mess with success?
Btw when I was on Lupron back in 2015 my RO advised me to use one patch changed twice weekly to stop hot flashes. Worked great!
Thank you for sharing your experience. It's great that your testosterone reached < 10 mg/dL, which is associated with significantly improved survival metrics (many references).
I wish my father could use estrogen patch in place of Lupron. Like you, he's also on 1/2 dose of Xtandi due to side effect and it works well so far. I'm finding a way to get our hands on Estrogen patch. If not, I wonder if "Estradiol Vaginal Cream, USP, 0.01%" can be used and how. The patch is a lot more convenient with its form and concentration.
Maybe change doctors? Has he given a reason why he won’t prescribe it? Sounds like he’s working with old data about the oral version which did indeed cause blood clots. The patches are as safe as any other form of ADT with fewer side effects.
Content on HealthUnlocked does not replace the relationship between you and doctors or other healthcare professionals nor the advice you receive from them.
Never delay seeking advice or dialling emergency services because of something that you have read on HealthUnlocked.