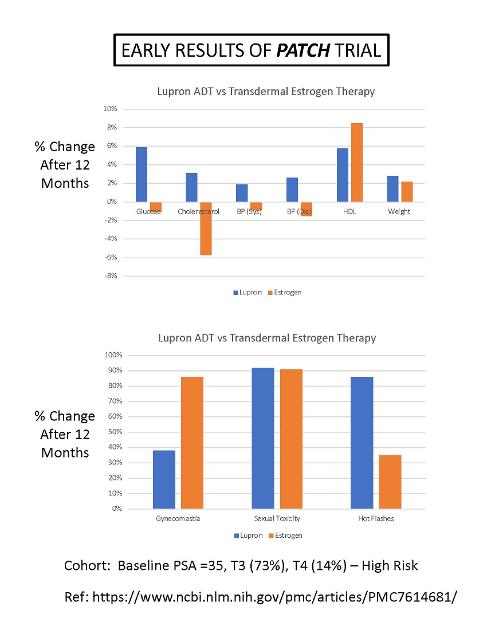
Here are some Early Results from the first year of the Transdermal Estrogen PATCH trial. References are available on their website at: patch.mrcctu.ucl.ac.uk.
The cohort was men with High or Very High Risk prostate cancer. Stage T3 (73%) and Stage T4 (14%), baseline PSA = 35 ng/mL.
The upper chart shows the % change in a given measurement after 12 months of treatment, comparing Lupron ADT to high-dose transdermal estrogen (TDE) patch. The biggest improvements with using TDE are reductions in: blood glucose, cholesterol, and blood pressure, and increases in HDL. No increases in adverse Cardio Vascular Events (CVE) were observed in the TDE arm, supporting the safety of doing Transdermal Estrogen versus the older Oral Estrogen treatment (from 1950 to 1980), which had problems with blood clots.
The lower chart shows significantly reduced Hot Flashes with TDE therapy. Unfortunately, the incidence of gynecomastia (enlarged breasts) was significantly higher with TDE therapy.
Bob
Written by
janebob99
To view profiles and participate in discussions please or .
I got a message today from the Lead on the PATCH study team in the UK that they have a target date of this coming fall to publish the long-awaited survival dta for the study.
Thank you for the information. Then we will have to wait until the patches get approved for prostate cancer. I hope the manufacturers show some interest in this.
The UK PATCH study is sponsored by a number of pharmaceutical companies in the UK. There is a US supplier of estrogen gel for women (Estrogel) that provides a doctor who writes prescriptions for Estrogel.
In response to the comment, "I hope the manufacturers show some interest in this [i reference to transdermal E2]," what comes to mine is that Pharma will change the packaging of the current prducts to blue, labelling it as "E2 for men" and raise the price...much like the elevated price of "just for men" shampoo.
I think the patches are FDA approved for women, not for men. Therefore the approval for the existing patches would need to be modified based on the PATCH trial. Currently, most doctors will not prescribe them for men and the insurance will not pay for them too.
The patches have advantages regarding side effects over Lupron, but I think they will be mainly used against PCa in low-income countries.
It is a bit more complicated than that. I would be happy to discuss the depth and breadth of the issues as I see them. However I am a slow typist and thus prefer to talk than to type. Let me know via regular email if you want to talk about E2 (and possibly also T). If so, give me some alternative times and numbers to reach you.
Sorry, the response was going to be quick and turned into a long rant.
Currently I am using Estradiol gel from Trigen Laboratories. Trigen manufactures generics, it was $55 out of pocket (no insurance) at Costco. At this price for a generic, there does not seem to be significant margins for big pharma to get their claws into the market. Even if estradiol is repackaged and marketed for men, can the additional margin offset the costs of entering a generic market.
Next issue would be once PATCH results are published, how many doctors will actually read the study and give is a chance on their patients? What would the incentive be to prescribe a generic estradiol as compared to LHRH or Relugolix What I found in my meet & greets and discussions with various doctors, if older would be against due to CV issues (even though this has been proven not to be true) and was discontinued as a SOC once LHRH was approved. They would say the use of LHRH for years, yes there are some SE but the use has been proven to be effective over the years. When challenged on the SE, they would gloss over and reiterate it is current SOC. As far as costs, this was not a factor in their consideration. Relugolix is the new hot button, its SE are less than LHRH, but it is extremely high. Follow the money and the picture becomes clearer.
The FDA is important in what can and can't be prescribed. Not to be too much into conspiracy but, almost half of the FDA's annual budget comes from big pharma. Many of the FDA lobbyists are from big pharma and big pharma has some former lobbyist on their Boards. Check out @Cancelcloco on X. FDA has also experienced politicalization over the years.
That is not to say every PC patient would be a candidate for estradiol as an ADT. This comes back to my previous rant, it is too easy to put the patient in a box citing SOC and what is easiest and quick for them. Luckily there are healthcare professionals/doctors that will listen to the patient, think outside the box and are disgusted with big pharma.
Digging into the history of Trigen, manufacturer of the estradiol gel I use, it was purchased by Osmotica Pharmaceutical in 2016. Osmotica Pharmaceutical was acquired by Alora Pharmaceuticals, LLC in 2021. Since Alora is an LLC, trying to find out the owners of it is difficult. Looking into several of the generic manufacturers, this is not unusual to be an LLC and ownership is closely guarded or they are foreign owned companies.
I predict there will be a giant sucking sound when the PATCH results are published this Fall. It will have a huge impact on thoughtful, informed doctors. That's why I'm trying hard to raise awareness of the benefits.
I had a poster write that he was suicidal on Lupron ADT. That's enough incentive for me to continue talking about this. One patient at a time...
Joining the rant club... Estrogen is one of the few areas I've not read a lot about but coincidentally I ran across this thread when researching how to reduce hot flashes when receiving ADT. There appears to be several people here attesting to the Estradiol Patch greatly improving things. I realize this study is more about using it as an alternative to "traditional" ADT. This seems rather odd to me as this isn't a new drug and I would have thought it would have been studied to great extent years ago in this treatment context?
I did see some study with the word "resurgence" in the title regarding Estrogen and Prostate Cancer, I suspect this study may have something to do with it (I've got info overload right now.)
It seems the big painful boobs side effects is the main one and then less frequently mentioned is problems with veins in your legs which is a lesser frequency. So did Oncologists sort of abandon the whole Estrogen ADT route years ago because patients were too put off about growing boobs despite the benefits in a better side effect profile in multiple areas compared to ADT? I'm kind of baffled here.
I just read a study that only a 0.05 mg patch reduces the severity of hot flashes, but not frequency. 0.1 mg does both. There's a 0.075 mg patch which may do both to significant extent but with less chance or less severe side effects than 0.1. If I read it right they were using 0.4mg in this PATCH study which makes sense if you are doing for ADT versus for reducing traditional ADT side effects.
I'm still baffled that on a substance that's been around so long that there really aren't any decent clinical studies on long-term outcome regarding effect on disease progression compared to traditional ADT? Weird. If you were to assume they have similar outcomes long-term I guess it boils down to most patients choose hot flashes over boobs with sore nipples? Or can doctors not "legally" prescribe these patches? Seems like off-label use on many things is pretty common. Were doctors scared of getting sued by prescribing the patch off-label and then their patient dies of a heart attack? So the finding so far is that there isn't an increase in cardiovascular risks so this would be a green light I would think for a lot of Oncologists. Especially from the low-dose use to mitigate hot flashes of traditional ADT.
Estrogen has been used for 84 years to treat PCa, but the oral estrogen (DES) that they used caused blood clots and other CV problems. It was replaced with Lupron in the 80's. In the 90's, researchers started using transdermal estrogen (TDE) gel, patches, IM shots, and subcutaneous pellets. The transdermal delivery route eliminated the pass through the liver, which eliminated the problems with blood clots and CV events.
Here is a plot showing the Serum E2 concentration vs applied E2 dose with patches. People can do low-dose "add-back "TDE, or they can do high-dose to replace Lupron ADT.
THe 10-yr phase-III PATCH trial comparing Lupron to Estrogen ADT will be published this Fall. The PATCH study used four, 100 microgram patches, applied twice weekly.
Side effects of TDE include gynecomastia, muscle loss/weakness, and increased risk of breast cancer (which is a very low risk, but can be a high risk if you have BRCA 1/2 gene mutations). If you think you're going to use TDE, you should get your gene status tested for free at (promiseforcancer.org).
I'm oligometastatic CS, on lupron and abiraterone, have had good response but am interested in estradiol to reduce side effects. I see in Patch trial and stampede they compare ADT to estradiol, one or the other. Can one use estradiol as an adjunct to ADT, seems like it should work?
Yes, there are studies that looked at adding-back Estrogen (E2) to Lupron ADT to ameliorate side effects. The higher the E2 dose, the greater the improvement in most (but not all) ADT symptoms. If you send me an email to janebob99@lobo.net, then I will send you papers and plots, if you're interested in researching this.
Content on HealthUnlocked does not replace the relationship between you and doctors or other healthcare professionals nor the advice you receive from them.
Never delay seeking advice or dialling emergency services because of something that you have read on HealthUnlocked.

")