I had a nice breakthrough today. 😀
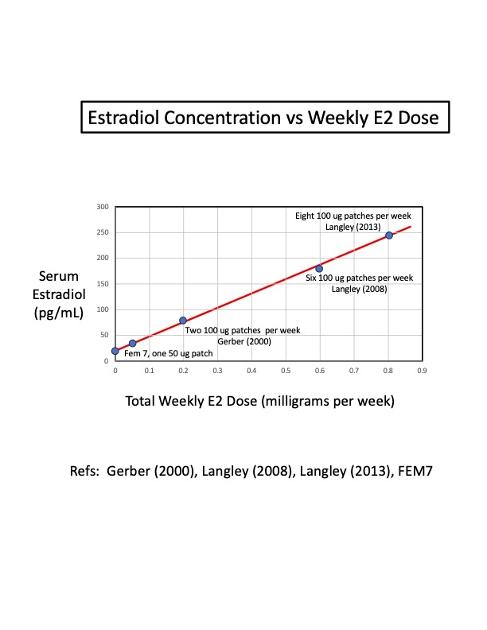
I collected all of the available data on the number of estrogen patches that the studies have used, and plotted the measured serum estradiol level versus total milligrams of estrogen used every week.
I was pleasantly surprised when all five of the data points fell almost perfectly on a straight line! That rarely happens in prostate cancer research.
It makes sense, though, that the concentration of serum estradiol should increase proportionately as the dose of estrogen increases...you're feeding the body with estrogen. There is no sign of leveling off or non-linear behavior at these high-doses.
This plot will help doctors and clinicians to easily pick the right estrogen dose ( # of patches) for their patients. Some men may need to titrate (adjust) the number of patches in order to reach a desired amount of castration (for example, T < 10 ng/dL). I hope to be able to generate a similar plot for men who use estrogen gel, although that is less standardized.
Low-dose estrogen (2 patches per week) can help manage hot flashes in men on ADT, while high-dose estrogen (4 patches, changed twice a week) can be used to chemically castrate men without having the bad side effects of Lupron ADT.
In this latter case, men should be able to simply replace Lupron ADT with high-dose transdermal estrogen (patches, gels, or IM shots).
Or, they can combine Lupron ADT + transdermal estrogen (either low-dose or high-dose). There would likely be a synergistic effect of combining the two, although this remains to be studied in the high-dose setting. This option may be more favorable to doctors who are concerned that estrogen therapy is not current Standard of Care.
The ultimate goal for castrate-sensitive men is to get their testosterone down to < 10 ng/dL, and preferably less than 5 ng/dL. Some men on estrogen have reported getting their T down to 3 ng/dL, which is a fantastic number!
