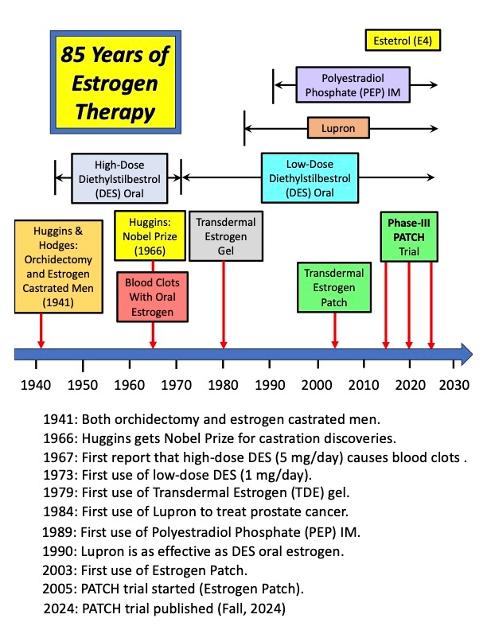
I made this chart which shows the historical timeline of Estrogen use for treating prostate cancer.
Estrogen has been used for about 85 years, with various forms of delivery.
With the exception of high-dose oral estrogen (DES) causing blood clots from 1945 to 1970, the other forms of estrogen (e.g., transdermal) have had a very successful history.
Most doctors have forgotten, or never learned, about the long history of estrogen use.
Bob
