I'm trying to work out what my next steps are and would really value any advice... Brief history below:
- Diagnosed hypothyroid in Nov 2024 and put on 50mcg Levo
- Went back in Jan 2025 for blood tests and increased to 75mcg Levo + 40,000iu Vit D once a week for 8 weeks
- A bit up and down but overall I've been feeling worse week by week, went in for new blood tests last week.
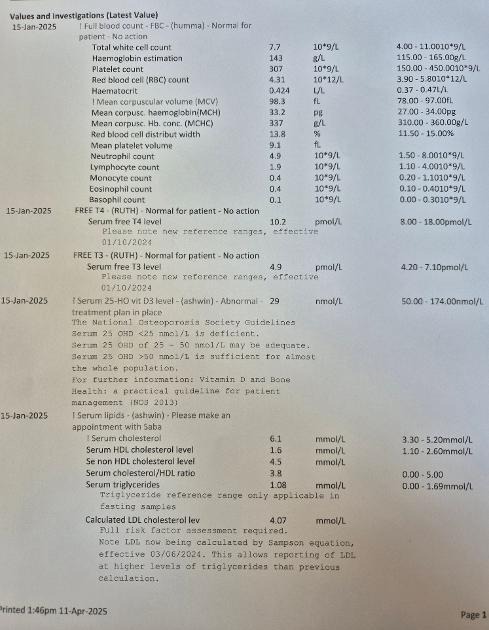
Where I'm not sure how to progress is that they've made me the first available appointment to discuss those results but it's not for five weeks, and the surgery won't share the results until I've had that appointment. I've put my January results here in case that's helpful/anyone has any advice based on those at least... FT3 and FT4 were both within lab range, although I'm not really sure what to look for other than that. I thought they were going to test iron levels but that doesn't look like it's on here.
It feels like my options are to either slightly increase my Levo dose on my own pending an appointment and see what happens, or I'll have to consider going private which isn't ideal given I think I'm going to have to cut hours at work because I feel so tired. If the latter any recommendations on who to talk to very welcome.
Thank you
Written by
momo81
To view profiles and participate in discussions please or .
IMPORTANT......If you are taking vitamin B complex, or any supplements containing biotin, remember to stop these 3-5 days before ALL BLOOD TESTS , as biotin can falsely affect test results
In days before blood test, when you stop vitamin B complex, you might want to consider taking a separate folate supplement (eg Jarrow methyl folate 400mcg) and continue separate B12 if last test result serum B12 was below 500 or active B12 (private test) under 70
Thank you, I'll definitely take a look at those - it sounds well worth it. It's less the cost of the tests than having to do private consultations about results/private prescriptions. Presumably with the test results I can go back to the GP, it's just a long time to wait even just for a phone appointment. A friend with hypo told me to check I'm not one of the minority who don't convert well, what would I need to look for to establish that?
"IMPORTANT......If you are taking vitamin B complex, or any supplements containing biotin, remember to stop these 3-5 days before ALL BLOOD TESTS , as biotin can falsely affect test results"
Thyroid hormone therapy can influence the metabolism and status of several vitamins and minerals. T3 has a stimulatory effect on many physiological processes, which can result in faster turnover or increased demand for certain nutrients. Here's a summary of key nutrients that may be depleted or become functionally insufficient in people taking levothyroxine (T4) or T4/T3 combinations:
I've been on T4/T3 combo therapy and my potassium level had dropped to 3.7 mmol/L (range: 3.5 - 5.3). I was experiencing skipped heart beats and muscle weakness. I began taking KCl powder.
While you'll probably need a few more increases in thyroid hormone dosage, you'll want to rule out the possibility of an insufficiency in a vitamin or mineral, focusing on those that have a direct effect on T4 → T3 conversion. Iodine deficiency is rare, but you might want to evaluate your dietary intake for that. Levothyroxine 75mcg has around 49 mcg of iodine.
Key Vitamins and Minerals Involved:
1. Selenium
Role: Selenium is essential for deiodinase enzymes, which directly convert T4 into the active hormone T3.
Form: Selenomethionine or selenium yeast.
Recommended dose: Usually around 100–200 mcg/day.
2. Zinc
Role: Zinc is involved in the activity of deiodinase enzymes. It supports proper thyroid receptor function and helps regulate T3 synthesis.
Recommended dose: Typically 15–30 mg/day, though doses vary based on individual needs.
3. Iron
Role: Iron is critical for proper thyroid metabolism, influencing the activity of thyroid peroxidase and contributing to healthy thyroid hormone synthesis and conversion. Iron deficiency can impair T4-to-T3 conversion.
Recommended dose: Dose varies widely (around 18 mg/day, higher for those deficient or anemic).
4. Vitamin D
Role: Vitamin D enhances thyroid receptor sensitivity and supports thyroid hormone utilization, indirectly supporting T4-to-T3 conversion and cellular action.
Recommended dose: Usually 1,000–5,000 IU/day, adjusted based on individual levels.
5. Magnesium
Role: Magnesium assists in converting T4 to T3 by supporting thyroid cell metabolism, enzymatic reactions, and hormone receptor sensitivity.
Recommended dose: Generally between 200–400 mg/day, depending on individual tolerance.
6. Vitamin B12
Role: Essential for cellular metabolism, proper mitochondrial function, and the energy-producing processes required for thyroid hormone conversion.
Recommended dose: Approximately 500–1,000 mcg/day sublingually or orally, especially if levels are deficient.
7. Vitamin A
Role: Facilitates thyroid receptor function and hormone signaling; indirectly supports optimal thyroid hormone activity.
Recommended dose: Recommended dietary allowance (RDA) is about 700–900 mcg/day.
Summary table of nutrients that can become depleted by T4 or T4/T3 combination therapy.
If you can’t access your results via the NHS app, you still have the right to your test results. I know it’s hard as you don’t want to undermine your relationship with your GP, but I don’t think they can refuse.
I requested scan reports from my hospital with a ‘subject access’ application - the first one was provided within a few days but I’m still waiting for the second - I think they have upto 30days to supply it but they can’t refuse me.
Content on HealthUnlocked does not replace the relationship between you and doctors or other healthcare professionals nor the advice you receive from them.
Never delay seeking advice or dialling emergency services because of something that you have read on HealthUnlocked.