I had a total thyroidectomy 11 years ago and I’m on 175 levothyroxine and 60 liothyronine but I feel bad and looked at my bloods and they look low on T3 considering how much I take….. what do you think?
is this ok: I had a total thyroidectomy 11 years... - Thyroid UK
is this ok
Written by

Justmayb
To view profiles and participate in discussions please or .
Read more about...
26 Replies
•
Hi Justmayb, welcome to the forum. ")
Your latest FT3 does look low, yes. How long have you been on your present dose? Since Feb 2020?
What time of day were all these tests done? Were they all done at the same time of day? And, how long was the gap between your last doses of T3 and the blood draw?
Do you also have FT4 and TSH results for these tests? It's not a good idea to just look at one result in isolation. The three need to be looked at in conjunction with each other to get the full picture.
How do you take your thyroid hormone? Do you split your dose? Do you always take it well away from food/supplements/other medication?
SlowDragonAdministrator
ALWAYS test thyroid levels early morning, around 9am latest , last dose levothyroxine 24 hours before test
Day before test split T3 as 3 smaller doses spread through the day with last dose approx 8-12 hours before test
Is this how you do your tests
Do you always get same brand levothyroxine and T3 at each prescription
Which brands
Essential to also test vitamin D, folate, B12 and ferritin
What vitamin supplements are you currently taking
What were last vitamin results and ranges
Always take levothyroxine and T3 on empty stomach
Have you thought about stopping your T4 dose for a few days to see if you feel better? I was taking a similar dose of T4 and T3 and felt awful, in fact I was close to a myxoedema coma. I took the decision to stop T4 as I was just getting worse but after just a couple of days of stopping the T4 I was beginning to feel better. I now know that my pituitary has failed and I dont have a TSH at all which I think was affecting the coversion of T4 and making it work against the T3. It took about a month for the T4 to disappear from my system, now its zero and I rely on just the T3 medication that I take. I must say that this is right for me but might be worth trying to see if it helps you.
Heather
How would the T4 'work against' the T3?
I can only suggest that the non existence of TSH causes the conversion of T4 to make Reverse T3 rather than T3. I just know that when I stopped the T4 I began to feel better and I have never touched T4 since then.
I agree with you that T4 doesn't suit everyone, it didn't suit me and I didn't even have a conversion problem.
There's always some T4 that is converted to rT3, even in thyroid-healthy people. That is perfectly normal. But, rT3 is inert and doesn't cause symptoms, and it doesn't cause poor converstion. It is the result of a problem, not the cause. So, I really don't think T4 can 'work against' T3 in any way.
Deiodinases?
thyroidpatients.ca/2021/02/...
It’s complicated but this is one thing mentioned could be of relevance
As T4 rises beyond one’s setpoint, it can also elevate D3 enzyme activity, which has a net effect of intracellular T3 loss.
Agreed. But, the solution is simple: reduce the levo. Saying that T4 is 'working against the T3' makes it sound as if the T4 is having an effect on the existing T3, not that excess T4 is affecting conversion to T3. Vocabulary is very important. That's why I questioned it. It's confusing enough as it is! lol
I totally agree. I think people simplify to try and understand what is hard to get one’s head around and although it seems to explain it, it isn’t really correct.
Well, I really don't think it does explain it. I think anyone new to all this would get a false idea and increased confusion, and surely that's what we're here to avoid.
but they are important and it may be relevant. I don’t think knowledge of these things (deioadinases) is in any way bad or unhelpful they are hugely important in fact imperative as to how much t3 reaches our cells
I didn't say any knowledge was bad or unhelpful. And we seem to have strayed a long, long way from the original question. The OP was questioning whether her FT3 was low considering the amount of T3 she was taking. That has nothing to do with deiodinases.
gg,
That T3 med has to go somewhere, and if O/P isn’t taking with foods or other meds/hormones with binding (inducing) properties, then it will be deiodinase actions that are reducing thyroid hormone levels.
You know all the reasons for excess RT3 (driven by deiodinase type 3) and which congruently converts T3 to inactive metabolites. The body doesn’t choose but converts both T4 & T3 reducing the ‘frees’, and impairs future usage (by lowering D1 & D2).
You are right in that it is not the RT3 per se that is damaging but it is the deiodinases not working to be advantageous for wellbeing. The link TSH110 has provided offers great deiodinase explanation all backed up with credible sources.
greygoose
The OP was questioning whether her FT3 was low considering the amount of T3 she was taking. That has nothing to do with deiodinases.
I wholly disagree as it has everything to do with the deiodinases that control thyroid hormones. Other factors influence the three deiodinases and the links from Thyroid Patients Canada clearly explain the role of each. TSH110 has the right idea.
Deiodinases are to do with conversion. De - iodination, meaning the removal of one atom of iodine from one molecule of thyroid hormone.
If the OP were taking T4 mono-therapy, then I would agree with TSH110. But, as she is taking T3 mono-therapy and the amount in her blood does not correspond to the amount she is taking then that would appear to be an absorption problem, not a conversion problem, given that FT2 is never tested. Thank you for the aggression.
greygoose,
Deiodinases are to do with conversion. De - iodination, meaning the removal of one atom of iodine from one molecule of thyroid hormone.
Exactly, so why do you fail to see that by this happening it risks lowering T3 levels? radd above has indicated by mention of RT3, de - iodination occurs in BOTH hormones congruently and so lowers T3 levels also when F4 levels are reduced.
You would do well to read the links kindly supplied by a fellow members that will educate you deiodination influences far more than just conversion, and can reduce T3 levels by multiple influences.
I don’t thank you for the aggression, as there really is no need. This is a wonderful forum and most are willing to discuss/debate instead of taking umbrage 😊.
Well, actually, I did read the article. And nowhere did it address the problem of someone taking a high-ish dose of T3 but having a low level in the blood. Of course T3 is converted into T2 - three types, she said - but that should not affect the levels in the blood 12 to 8 hours after taking T3 in one person and not it others (and I didn't see the use of the word 'congruently' anywhere). If it did, there would be little point doing a T3 blood test. So that argument is spurious.
However, if you are suggesting that T3 can be converted into rT3... Well, that is just wrong. Nor did it say that in the article. Only T4 can be converted into T3.
As for taking umbridge, it's difficult not to when one is aggressed. And, now you're lecturing me. I really don't think it's your place to do that. I have had lots and lots of discussions and debates on this forum in the 21 years I've been on here, with nice people who didn't find it necessary to be aggressive or take the moral high-ground. I just react badly to being attacked. 😁
Oh dear, I don’t read it as anyone attacking anyone else, just friendly & helpful advice gg.
This is the link that explains how T3 is congruently reduced with T4. Hope it helps 😊 …. thyroidpatients.ca/2019/11/...
But, the whole point is, the OP is on T3 mono-therapy. Did anybody actually read the question?
gg,
O/P is medicating 175 levothyroxine and 60 liothyronine,
Oh! (Embarrassed face lol) I must be mixing her up with somebody else, then. My most humble apologies. I was convinced she was taking just T3. Perhaps because she only gave FT3 results.
However, the fact remains that the OP is taking quite a high dose of T3 but her levels IN THE BLOOD are low. Nothing in that article you linked me to says that T4 has any effect on T3 taken exoginously. Unless I missed it - if I did please point it out to me. Therefore, her low levels have nothing to do with conversion/rT3/deiodinases. And, all these posts telling me how ignorant I am - I am not - leave me feeling aggressed, whether you perceived any agression or not. Most of it was totally unnecessary, given that nobody can explain the connection, just give links that don't explain it either, and the fact that we have had no further information, or replies, from the OP herself.
I would have your B12, folate and ferritin checked. Your result is within normal limits but as I was told what is "normal"? Blood results are a guide not definitive to each person. Prior to my total thyroidectomy 10 years ago I had a couple of episodes of low B12. I checked my immunoglobulin too as there was a history of pernicious anaemia in the family. However I found a research paper that stated people with thyroid issues can also have B12 issues. Since thyroidectomy I have stabilised on Levothyroxine 100mcg daily. I also take a vitamin supplement that contains B12 and have felt much better than the 20 odd years I suffered with my thyroid as my T3 was "within normal limits". Hope this helps
A lot of people come to the same conclusion as Heather. I too was among those that just could not take Levo / T4. T3 came to be came to be my go to, and the over the counter bovine glandular at that! It’s weaker and as I learned from others here on HealthUnlocked you have to start out low and go slow, gradually increasing until you find the right dose, it’s like night and day difference. (From Levo) The good news is, if you go over slightly, on the dose, it dissipates quickly like in hours. It has been said when going up or down with Levo / T4 (and looking for any kind of changes) think days. With T3 think hours. It was very true in my experience. Bovine glandular actually has more than just T3, (which makes it all the better in my experience!). I have a thyroid gland so I don’t know how / if that makes a difference. I also learned to stay away from iodine supplement of any source - even that in foods higher in iodine, like seafood, dairy, (especially cheese!), eggs. It’s been a long hard slog, because in my case, the Drs were clueless and it took so long to figure that out and educate myself - but I am finally SO MUCH better! Recently, I have lost 50 lbs, energy has returned and my brain is working like it did when I was young - I can recall and remember things again! It has been a little over 3 years since my last Levo. Again, I have a thyroid and I do believe it has healed, so I don’t know how / if it will work for you. I am down to minuscule amounts of bovine glandular ever 5 to 10 days if you can imagine that…after more than 30 years on the pharmaceutical T4 / T3 miserable (by comparison) roller coaster. Two key factors in feeling great again (for me) were lower iodine intake and bovine gladular thyroid hormone replacement. I also take a thymus glandular supplement, bovine sourced, two to three times a week - a much lower dose than recommended on the bottle, but I learned that the thymus somehow is a part of the whole thyroid / body metabolism. HealtUnlocked is a great educational source! Another! Dr. Christianson - an online endocrinologist who himself used to have thyroid problems. He sells supplements it is true, but he offers a ton of free information - even free Zoom events. Another great source of thyroid education.
I can’t see the entire results only the ranges.
Hello Justmayb and welcome to the forum ;
The other option you haven't tried yet, that you may like to consider, is that of Natural Desiccated Thyroid which contains all the same known hormones as that of the human gland, namely trace elements of T1. T2 and calcitonin plus a measure of T3 and a measure of T4 in each dose and derived from pig thyroids dried and ground into tablets referred to as grains.
NDT is the original treatment for hypothyroidism and has been used successfully for over 100 years and on the back of which Big Pharma launched their own T3 and T4 synthetic options and then went about claiming their market share by fair means or foul.
The two leading brands Armour and Efra are prescribed to some on the NHS - but many of us are forced to self medicate and Do It Ourselves.
No thyroid hormone replacement works well until you core strength vitamins and mineral are up and maintained at optimal levels - these are ferritin, folate, B12 and vitamin D.
Your results are ok, but obviously not restoring your health and well being as otherwise you wouldn't be on here asking questions, and this just another option you may like to consider.
I agree with others that it is good to see the whole thyroid panel, of TSH, freeT4 and freeT3 together, and to hear a bit more about the context. Were you taking the same dose for all these tests and was the blood sample taken correctly under the same conditions? And possibly the most important question, did you feel any better on any dose in the past or have you always felt just as bad?
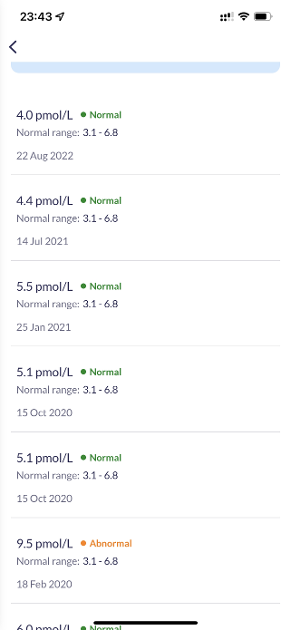
Still, freeT3 is generally the most important of the three in a thyroid panel, particularly when you are taking some T3. This is because T3 is the active form of thyroid hormone needed by every cell and organ in our body, so is the result most closely linked to symptoms. For both freeT3 and freeT4, a person with a healthy thyroid would have these numbers about halfway through the range. But once we are on thyroid hormone replacement we need it higher than that. Most people will feel well with freeT3 fairly high in range, at least in the top third, if not all the way to the top. Your most recent result from August 2022 shows freeT3 just over 25% up the range, so this is low. It would be common to feel rubbish with results like these.
You've had one result over the range in Feb 2020 that I can see. It's possible to feel well with a result like this, but carries some health risks. If a doctor sees it they would immediately push for a dose decrease. You don't say whether you did have a dose reduction or anything else at this time, but by the October your freeT3 had dropped to around halfway through the range. Again, symptoms are the most important thing. Some people could feel well on a freeT3 halfway through the range, but it is still a fairly low level and many people will need it higher, so from October 2020 to August 2022 your freeT3 was fairly low, and dropping the whole time.
I would say you need an increase in T3. T3 is very potent, so an increase of 5-10mcg is a good increment. Often we have to round up or down from constraints in tablet sizes. A good pill cutter should be able to get the tablets into quarters. Some are better at cutting than others. You may need more than one increase to feel better.
I agree with others that it's likely you don't need all that Levothyroxine alongside your T3. I've also had a thyroidectomy. It is great to see so many of us on the forum as it used to be very rare to find anyone else who had had one After many years of self medicating I've become more and more suspicious of excess Levothyroxine /T4. You are taking quite a large quantity of both Levo/T4 and T3, each could be considered a full replacement dose in itself, so this is double the dose some people could feel well on. Now that doesn't necessarily mean it is too high for you, we are all different and some people need high doses to feel well. But I think the more unusual something is, the more you need a good reason to be doing it that way, so you need to be sure that all that T4 is right for you.
What another poster mentions is correct, too much T4 can trigger a feedback mechanism in the body that reduces conversion of T4 into T3, and blocks T3 getting into cells, so you may not be getting the full benefit of the T3 you are taking if you've got excess T4 sloshing around.
I'd want to know what doses you've previously taken, how you felt on them, and to see the freeT4 results that went with each of these test results to fully advise. But I would conservatively suggest that when you add some extra T3 you reduce your Levo/T4 dose by a corresponding amount. Because T3 is more potent than T4, this would be around 3-5x as much T4 as T3, so if you add 5mcg of T3, drop by 20-25mcg of T4 (you may have to round up or down due to constraints of tablet sizes). Using these amounts would mean your total dose remains about the same. As you continue to add T3 if you need two or three increases you could continue to drop the T4. Pay attention to how your symptoms feel, and monitor everything when you make any adjustments. Stay on any dose change for at least six weeks for things to settle and get a feel for how it suits you. If you feel any worse you can always return to a previous dose.
If this hormone is prescribed and you won't have the immediate freedom to increase your T3 as you need to, another short term option could be to reduce your Levo/ T4 by a small amount and see if it improves your symptoms at all. 25mcg is the usual amount to change in an adjustment, but if you feel nervous you could adjust by half that if you like. When I tried this a few years ago I was surprised to find that reducing my T4 improved my symptoms as much as increasing T3 had. If you decide to try this, move slowly and monitor your symptoms closely, and see how you feel. If you are lucky and feel an improvement after trying a reduction you could try another six weeks later. And of course if you feel any worse reverse any change.
Not what you're looking for?
You may also like...
Are these ok?
possibly a goitre but wasn't sure. GP ordered bloods to check my thyroid as other symptoms pointed...
Are these ok?
they actually look alright
My TSH is 0.51 - the range given is 0.35-5.0 mU/L, so I'm quite low in...
Are these results ok?
75 mcg and 50 mcg until my next blood test in 2 months' time. I feel fine on 75 mcg daily but I am...
Are these results ok?
as normal. The only thing that was a bit low was my total white cell count. Here are my results:...
Do these results look ok?
here and would be grateful if you lovely people here could take a look for me?.
The Dr I saw about...