Hello my condition is hypothyroidism and was diagnosed about a year ago
So would like to ask currently on Levothyroxine but would like to change to Thyroid s as I'm really not getting on with my present medication and currently still got symptoms of fatgue hairless and brittle nails I've been on Levothyroxine at 100mg since diagnosed i have informed my doctor of my continued symptoms but she has advised me that i do not need to increase
I have managed to get a source of Thyroid s but unsure how to begin taking it my current Levothyroxine is 100mg
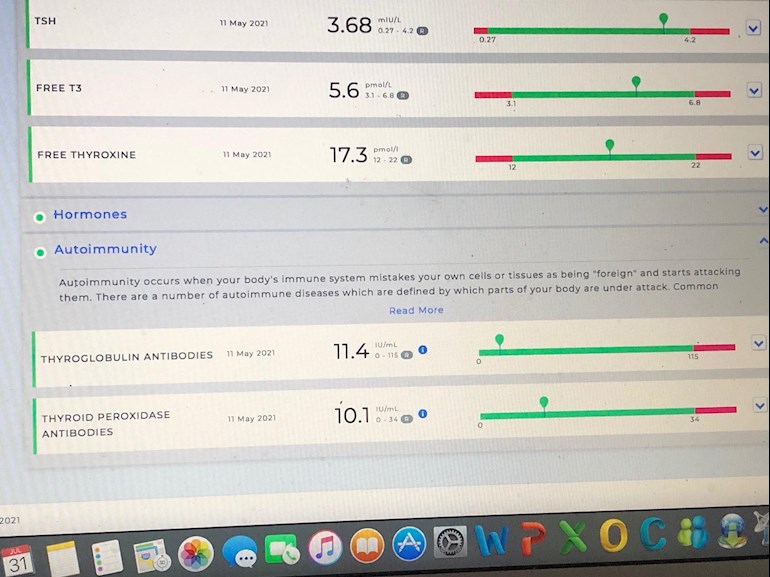
So do i stop this all together and start on thyroid s and if so how do i calculate how much to take my T3 and T4 are ok but my TSH is on a higher end antibodies are fine
It would be helpful for those members who would like to reply if you gave the actual results and reference ranges for your TSH, FT4 and FT3, just saying OK and higher end doesn't allow us to give meaningful comments.
I think you'd be better off sourcing levo and increasing your dose.
Or better still, going to a different GP to get them to prescribe a higher does.
Your conversion looks good so in theory levo should work for you once you get your TSH around 1.
There are guidelines you can show your GP to argue the case for a TSH around 1. Some of them are NHS guidelines too.
• in reply to
Thank you Plant_lady so i will try increasing by 25 and hopefully that will improve should i take it all at once or split the dose haven't had much help with this apart from this sight which is great
The reason you are still symptomatic is because you are undermedicated. The aim of a treated Hypo patient on Levo only, generally, is for TSH to be 1 or below with FT4 and FT3 in the upper part of their reference ranges.
What you need at this stage is an increase in your Levo. Your TSH is far too high and your FT4 is only 53% through it's range, you would probably do better with your FT4 around 75% through range or even higher with a much, much lower TSH.
It was only in April that you were started on Levo after a visit to A&E after you posted your results showing a TSH of >100 and well below range FT4 and FT3. You now need to give it time, it can take many months to improve and reach optimal medication to give you optimal hormone levels. You are still in the early stages of your journey although there is a vast improvement in your levels.
There is no indication that you need combination medication (the T4 and T3 that NDT contains), you have a good amount of FT3 from your mid-range FT4, increase your Levo, this will increase your FT4 and also increase your FT3.
If we can be optimally medicated on Levo then this is far, far easier than relying on having to continually source NDT which, in the last couple of years has been near impossible to obtain and has only just started to become available again, then there is the expense of the tablets themselves which has risen considerably recently, plus the fact that it has to come from overseas which means the risk of paying VAT and collection fees upon delivery.
i have informed my doctor of my continued symptoms but she has advised me that i do not need to increase
Is this is the same GP who said Levothyroxine was "happy pills" and refused you treatment. If so maybe remind her that she was very negligent originally and doesn't seem to follow guidance for treating hypothyroidism. It may be better to see another doctor in the practice. Did you ever make a formal complaint about the original doctor and her neglect?
Evidence to support you in your request for an increase in dose from respectable/reliable sources available to your GP:
How can blood tests be used to manage thyroid disorders?
.....
Occasionally patients only feel well if the TSH is below normal or suppressed. This is usually not harmful as long as it is not completely undetectable and/or the FT3 is clearly normal.
There are also certain patients who only feel better if the TSH is just above the reference range. Within the limits described above, it is recommended that patients and their supervising doctors set individual targets that are right for their particular circumstances.
.....
Also, Dr Toft, past president of the British Thyroid Association and leading endocrinologist, states in Pulse Magazine (the professional publication for doctors):
"The appropriate dose of levothyroxine is that which restores euthyroidism and serum TSH to the lower part of the reference range - 0.2-0.5mU/l. In this case, free thyroxine is likely to be in the upper part of its reference range or even slightly elevated – 18-22pmol/l. Most patients will feel well in that circumstance. But some need a higher dose of levothyroxine to suppress serum TSH and then the serum-free T4 concentration will be elevated at around 24-28pmol/l. This 'exogenous subclinical hyperthyroidism' is not dangerous as long as serum T3 is unequivocally normal – that is, serum total around T3 1.7nmol/l (reference range 1.0-2.2nmol/l).*"
*He recently confirmed, during a public meeting, that this applies to Free T3 as well as Total T3.
You can obtain a copy of this article from Dionne at ThyroidUK:
tukadmin@thyroiduk.org
print it and highlight Question 6 to show your GP.
Also essential for thyroid hormone to work (and before we consider adding T3) is to ensure we have optimal nutrient levels. Have you had the following tested, if not you should make this a priority and if GP wont test you can do them with one of the recommended private labs.:
Hello i was so bad back then cannot Thank this site so much its taken some time to actually feel normal actually think again I ended up twice in hospital since then because i cannot get much help I did eventually changed practice but the GP there is not very knowlegdable either so been doing lots of book reading
So if i increase Levo by 25 and see how that goes
Can you tell me being under medicated would that explain why my hair has fallen out even on my body including eyebrows half way along and total itchy head like a prickling feeling i can't understand it driving me mad and confidence
Had my ferritin checked 135 Magnesium 1.02 vitamin D 85 B12 high 256 I'm not really sure
Yes, 25mcg increase now, retest in 6-8 weeks, further increase if necessary, always testing 6-8 weeks after any dose change.
Remember to do test no later than 9am, before eating or drinking anything except water, and take last dose of Levo 24 hours before the test. If you take Biotin or a B Complex supplement this should be left off for 7 days before the test.
Hairloss is a symptom of hypothyroidism, loss of outer third of eyebrows is also a very typical symptom. List of symptoms here:
Thank you so much i asked my doctor to increase but she would not sent me away saying that hair loss comes with age and a diet sheet on cholestrol but i knew i still was not right and my cholesterol is so high total cholesterol 7mmoi/L <5r and ldl cholesterol 4.3mmol?l<3r and read online it can effect cholesterol i cannot thank you all for your support will let you know progress
They are ignorant Seaside Sue The times I've just cried and they look at me like " oh not another one " as if your looking just for attention or some thing I've change practise 3 times and each one i see first one said it was menopause then after 6 months no improvement changed GP again and its like they do not like it if you tell them what is my problem is they don't like you to have knowledge on thingsThere must be some really nice ones out there but haven't found one yet.
Stupid idiot hair falling out is not simply due to age! It might be with men. You need to see someone else for the good of your health. That woman is a fool.
Several months ago I had my annual thyroid blood tests and also a cholesterol test by my GP. I felt my levothyroxine was too low. They said my levo was fine but that I needed statins because my cholesterol was high.Following advice on here I argued with the doctor that my cholesterol was high because my thyroid was undermedicated. She agreed that I could try a 25mg increase in Levothyroxine. After 6 weeks on this dose my cholesterol was retested - the nurse said she had never seen such a dramatic decrease in cholesterol. Good luck with getting it sorted out.
Thank you for your message I've been to my Doctor she will not increase dosage so fed up fighting with them so going to see if i can get it privatley online its total rubbish I've got to do the but try anything to get better x
Hello SeasideSusie,Thank you for your interesting and helpful post.
I have had a look at the linked site, but cannot find where it says this:
“Occasionally patients only feel well if the TSH is below normal or suppressed. This is usually not harmful as long as it is not completely undetectable and/or the FT3 is clearly normal.”
I was delighted to read it because I am on 20mcg T3, 75mcg T4, TSH is suppressed (only just detectable), FT3 and FT4 both within range. No hyper symptoms (I take all the dose at once at bedtime). Consultant not happy about TSH because I have Osteopenia, possibly osteoporosis according to DXA scan. (But I think it’s post menopausal and coeliac disease - only relatively recently diagnosed).
Anyway, I’d love to know where to find that quote on the BMA site 🙂
I have had a look at the linked site, but cannot find where it says this:
“Occasionally patients only feel well if the TSH is below normal or suppressed. This is usually not harmful as long as it is not completely undetectable and/or the FT3 is clearly normal.”
Anyway, I’d love to know where to find that quote on the BMA site
It isn't the BMA's site, it's the British Thyroid Foundation that I have linked to. However, they appear to have done an update (most recent is recorded as 2021) and have now changed the wording under that heading and removed that quote so I will now have to remove that from my replies which is a crying shame because that was a very useful piece of evidence for our members and probably carried more weight that Dr Toft's article.
However, it wouldn't apply in your case as you're taking T3 and that tends to cause low/suppressed TSH anyway. It only applies to patients taking Levo.
**
Hidden For your information. The quote from the British Thyroid Foundation is no longer relevant as they have changed the wording so you wont be able to use that in support of your request for an increase in Levo. However, the GP Online and Dr Toft quotes should be useful.
You can stop Levo straight away and start on a small amount of thyroid s gradually building up the dose as advised in the guide.
I reduced Levo by 25mcg increments as I increased ThyroidS by 1/4 grain increments but it is not necessary to keep taking Levothyroxine I did it just in case the NDT didn’t work and I had could go back to Levothyroxine.
I would not start on a full replacement dose of NDT because the T3 in it can take time to adjust to. I had to split my dose of NDT but I no longer need to do this (been on ThyoidS for 7 years).
I feel a lot better on NDT than I ever did on Levothyroxine.
My endo aimed for TSH between 0.2 and 0.5 on Levothyroxine. Your TSH is way too high it should be under 1 at the very least so your doctor is wrong, you would benefit from a dose increase. But if the GP is refusing to listen to you what can you do? Telling you are well when you are not is a disgrace and with those numbers, that’s incompetence. Admin have a list of sympathetic medics you could try if you could afford. You just need to email admin to get a copy. I see you have had terrible luck with GP’s.
I never felt well on Levothyroxine even with the low TSH my T3 was always very low. Yours is not bad perhaps more Levothyroxine might work. I tend to think NDT is better than Levothyroxine no matter what.
Hi I used to take ndt until it became unstable I’m currently on Levothyroxine and hate it ! Can you please let me know where you are getting your thyroid S from as I would love to get back off levo as it doesn’t work for me
Even if we frequently don’t start on full replacement dose, most people need to increase levothyroxine dose slowly upwards in 25mcg steps (retesting 6-8 weeks after each increase) until eventually on, or near full replacement dose
Consider starting levothyroxine at a dosage of 1.6 micrograms per kilogram of body weight per day (rounded to the nearest 25 micrograms) for adults under 65 with primary hypothyroidism and no history of cardiovascular disease.
Traditionally we have tended to start patients on a low dose of levothyroxine and titrate it up over a period of months. RCT evidence suggests that for the majority of patients this is not necessary and may waste resources.
For patients aged >60y or with ischaemic heart disease, start levothyroxine at 25–50μg daily and titrate up every 3 to 6 weeks as tolerated.
For ALL other patients start at full replacement dose. For most this will equate to 1.6 μg/kg/day (approximately 100μg for a 60kg woman and 125μg for a 75kg man).
If you are starting treatment for subclinical hypothyroidism, this article advises starting at a dose close to the full treatment dose on the basis that it is difficult to assess symptom response unless a therapeutic dose has been trialled.
Content on HealthUnlocked does not replace the relationship between you and doctors or other healthcare professionals nor the advice you receive from them.
Never delay seeking advice or dialling emergency services because of something that you have read on HealthUnlocked.