Hi everyone, this is referring to my mum not me. I’m absolutely fuming. I paid for my mum to do private blood test through medichecks as her doctors only ever check TSH and her annual bloods were just to check that and hb1ac and it turns out she has type 2 diabetes. Her TSH was in range but I felt she needed to get her T4 and T3 checked as she always complains she’s cold and struggles to lose weight. However the doctor didn’t say anything about increasing levothyroxine because her TSH is in range. Her vitamin d and folate are low as well. I’m finding GP’s are really rushing through patients and not listening to what they have to say. It’s really frustrating. Her results are as follows.
GP, results and not increasing levothyroxine - Thyroid UK
GP, results and not increasing levothyroxine
Written by

Cade83
To view profiles and participate in discussions please or .
Read more about...
7 Replies
•
SeasideSusieRemembering
Cade83
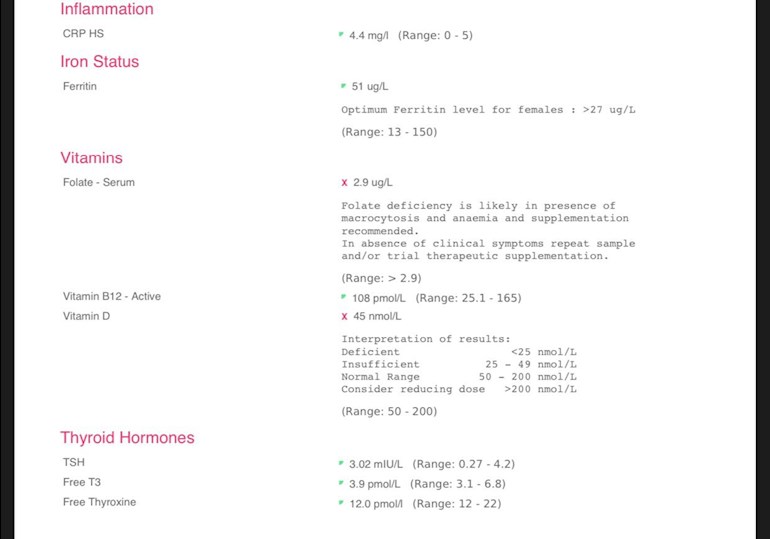
CRP is an inflammation marker so is best as low as possible, this is within range but quite close to the top.
Ferritin: 51 (13-150)
This is rather low. Ferritin is recommended to be half way through range, so around 82 with that range. Eating liver regularly, or liver pate, black pudding, etc, will help raise her level. She shouldn't take iron tablets without having an iron panel to see if she is iron deficient as if she already has a good serum iron level taking iron tablets could take it too high and too much iron is as bad as too little.
Folate: 2.9
This is Folate deficiency and her GP should address this - see cks.nice.org.uk/anaemia-b12...
◦Serum folate of less than 7 nanomol/L (3 micrograms/L) is used as a guide to indicate folate deficiency.
Active B12: 108
This is a good result.
Vit D: 45nmol/L
This is too low, her GP may prescribe a low dose supplement but probably not enough so she may be better addressing this herself.
The Vit D Society and Grassroots Health recommend a level of 100-150nmol/L.
To reach the recommended level from your current level, you could supplement with 5,000iu D3 daily.
Retest after 3 months.
Once she has reached the recommended level then a maintenance dose will be needed to keep it there, which may be 2000iu daily, maybe more or less, maybe less in summer than winter, it's trial and error so it's recommended to retest once or twice a year to keep within the recommended range. This can be done with a private fingerprick blood spot test with an NHS lab which offers this test to the general public:
Doctors don't know, because they're not taught much about nutrients, but there are important cofactors needed when taking D3.
D3 aids absorption of calcium from food and Vit K2-MK7 directs the calcium to bones and teeth where it is needed and away from arteries and soft tissues where it can be deposited and cause problems such as hardening of the arteries, kidney stones, etc.
D3 and K2 are fat soluble so should be taken with the fattiest meal of the day, D3 four hours away from thyroid meds if taking D3 as tablets/capsules/softgels, no necessity if using an oral spray.
For D3 I like Doctor's Best D3 softgels, they are an oil based very small softgel which contains just two ingredients - D3 and extra virgin olive oil, a good quality, nice clean supplement which is budget friendly. Some people like BetterYou oral spray but this contains a lot of excipients and works out more expensive.
For Vit K2-MK7 I like Vitabay or Vegavero brands which contain the correct form of K2-MK7 - the "All Trans" form rather than the "Cis" form. The All Trans form is the bioactive form, a bit like methylfolate is the bioactive form of folic acid.
Magnesium helps D3 to work. We need Magnesium so that the body utilises D3, it's required to convert Vit D into it's active form. So it's important we ensure we take magnesium when supplementing with D3.
Magnesium comes in different forms, check to see which would suit you best and as it's calming it's best taken in the evening, four hours away from thyroid meds if taking magnesium as tablets/capsules, no necessity if using topical forms of magnesium.
naturalnews.com/046401_magn...
drjockers.com/best-magnesiu...
Don't start all supplements at once. Start with one, give it a week or two and if no adverse reaction then add the next one. Again, wait a week or two and if no adverse reaction add the next one. Continue like this. If you do have any adverse reaction then you will know what caused it.
TSH: 3.02 (0.27-4.20)
FT4: 12 (12-22)
FT3: 3.9 (3.1-6.8)
Her TSH is too high for a patient on Levo, the aim generally is for TSH to be 1 or below with FT4 and FT3 in the upper part of their reference ranges. If her GP can't see that her FT4 at the very bottom of the range means that she is not taking enough Levo then he should retrain or find another job. It is ridiculous to leave her on that dose which doesn't produce enough thyroid hormone.
As she's been left on a starter dose of 25mcg Levo for years, this doctor seems to be very ignorant of how to treat hypothyroidism and should be ashamed of himself. She needs an immediate increase of 25mcg, retest in 6-8 weeks, repeat if necessary until her levels are where they need to be for her to feel well.
Unfortunately, as most doctors only look at TSH then she will have to persuade him that hers is too high. The following should hopefully help her get an increase:
From GP Notebook
gpnotebook.com/simplepage.c...
Target level for TSH during thyroxine therapy
Fine tuning of the dose could be necessary in some patients
* aim of levothyroxine treatment is to make the patient feel better, and the dose should be adjusted to maintain the level of thyroid stimulating hormone within the lower half of the reference range, around 0.4 to 2.5 mU/l. If the patient feels perfectly well with a level in the upper half of the reference range, then adjustment is unnecessary
From GP online
gponline.com/endocrinology-...
Under the section
Cardiovascular changes in hypothyroidism
Replacement therapy with levothyroxine should be initiated in all patients to achieve a TSH level of 0.5-2.0pmol/L.
From the British Thyroid Foundation:
btf-thyroid.org/thyroid-fun...
How can blood tests be used to manage thyroid disorders?
.....
Occasionally patients only feel well if the TSH is below normal or suppressed. This is usually not harmful as long as it is not completely undetectable and/or the FT3 is clearly normal.
There are also certain patients who only feel better if the TSH is just above the reference range. Within the limits described above, it is recommended that patients and their supervising doctors set individual targets that are right for their particular circumstances.
.....
Also, Dr Toft, past president of the British Thyroid Association and leading endocrinologist, states in Pulse Magazine (the professional publication for doctors):
"The appropriate dose of levothyroxine is that which restores euthyroidism and serum TSH to the lower part of the reference range - 0.2-0.5mU/l. In this case, free thyroxine is likely to be in the upper part of its reference range or even slightly elevated – 18-22pmol/l. Most patients will feel well in that circumstance. But some need a higher dose of levothyroxine to suppress serum TSH and then the serum-free T4 concentration will be elevated at around 24-28pmol/l. This 'exogenous subclinical hyperthyroidism' is not dangerous as long as serum T3 is unequivocally normal – that is, serum total around T3 1.7nmol/l (reference range 1.0-2.2nmol/l).*"
You can obtain a copy of this article from Dionne at ThyroidUK:
tukadmin@thyroiduk.org
print it and highlight Question 6 to show the GP.
Thyroid peroxidase antibodies 175 Range 0-34
You haven't shown them on the print out above so I've taken them from your other post. Her raised TPO antibodies confirm autoimmune thyroid disease, known to patients as Hashimoto's. Does she already know this? Some members find a strict gluten free diet helps but there is no guarantee.
Gluten contains gliadin (a protein) which is thought to trigger autoimmune attacks so eliminating gluten can help reduce these attacks.
You don't need to be gluten sensitive or have Coeliac disease for a gluten free diet to help.
Gluten/thyroid connection: chriskresser.com/the-gluten...
stopthethyroidmadness.com/h...
stopthethyroidmadness.com/h...
hypothyroidmom.com/hashimot...
thyroiduk.org.uk/tuk/about_...
Supplementing with selenium l-selenomethionine 200mcg daily is said to help reduce the antibodies, as can keeping TSH suppressed.
Hashi's can cause gut/absorption problems which can lead to low nutrient levels or deficiencies, this may very well be the cause of her poor levels.
SeasideSusie is so accurate in her comments.
SlowDragonAmbassador
See different GP and insist on 25mcg dose increase in levothyroxine
Bloods should be retested 6-8 weeks after each dose increase
Always test as early as possible in morning before eating or drinking anything other than water and last dose levothyroxine 24 hours before test
She’s likely to need further increases in levothyroxine over coming months
The aim of levothyroxine is to increase dose upwards in 25mcg steps until TSH is ALWAYS under 2
When adequately treated, TSH will often be well below one.
Most important results are ALWAYS Ft3 followed by Ft4.
When adequately treated Ft4 is usually in top third of range and Ft3 at least 60% through range (regardless of how low TSH is)
Extremely important to have optimal vitamin levels too as this helps reduce symptoms and improve how levothyroxine works
Email Thyroid UK for list of recommend thyroid specialist endocrinologists...NHS and Private
tukadmin@thyroiduk.org
TSH should be under 2 as an absolute maximum when on levothyroxine
gponline.com/endocrinology-...
Replacement therapy with levothyroxine should be initiated in all patients to achieve a TSH level of 0.5-2.0pmol/L.
New NHS England Liothyronine guidelines July 2019 clearly state on page 13 that TSH should be between 0.4-1.5 when OPTIMALLY treated with just Levothyroxine
Note that it says test should be in morning BEFORE taking levothyroxine
Also to test vitamin D, folate, B12 and ferritin
sps.nhs.uk/wp-content/uploa...
Aim is to bring a TSH under 2.5
UK guidance suggests aiming for a TSH of 0.5–2.5
gp-update.co.uk/SM4/Mutable...
Dr Toft, past president of the British Thyroid Association and leading endocrinologist, states in Pulse Magazine,
"The appropriate dose of levothyroxine is that which restores euthyroidism and serum TSH to the lower part of the reference range - 0.2-0.5mU/l.
In this case, free thyroxine is likely to be in the upper part of its reference range or even slightly elevated – 18-22pmol/l.
Most patients will feel well in that circumstance.
But some need a higher dose of levothyroxine to suppress serum TSH and then the serum-free T4 concentration will be elevated at around 24-28pmol/l.
This 'exogenous subclinical hyperthyroidism' is not dangerous as long as serum T3 is unequivocally normal – that is, serum total around T3 1.7nmol/l (reference range 1.0-2.2nmol/l)."
(That’s Ft3 at 58% minimum through range)
You can obtain a copy of the articles from Thyroid UK email print it and highlight question 6 to show your doctor
please email Dionne at
tukadmin@thyroiduk.org
Hi Cade83,I have had vit d deficiency and best to check the sign and symptons on google scholar reseach hypothyroidism with vit d deficiency.
As this help my case when my levels reached over 100.
Plus medichecks advise to be without meds for 14days to get best results, so that is difficult to do.
Hoping this helps.
She does not require thyroxine tablets as her TSH is fine. Would have been better to have done a T4, not T3.
Needs iron and folate tablets for a while.
Orchidman99
Did you actually read the opening post and look at the picture of the results? FT4 was tested. She is already diagnosed hypothyroid and on Levothyroxine. Her TSH is too high for a treated Hypo patient on Levo and her FT4 is at the very bottom of it's range - 12 (12-22).
Read through the replies, even the medical profession says her TSH is too high and recommends it be lower.
Not what you're looking for?
You may also like...
GP, results and not increasing levothyroxine
Hi everyone, this is referring to my mum not me. I’m absolutely fuming. I paid for my mum to do...
My friends results
My friend who has no thyroid condition had her bloods checked recently. She has cold hands, feet...
Results Interpretation
Hi everyone, you’ve been extremely helpful before so I’d like to ask re my mums historical results...
Levothyroxine and Atorvastatin
Can anyone tell me if there is any interaction between Levothyroxine & atorvastatin.
My 76 year...
Mums thyroid results
Hi everyone,
I recently got my mum a thyroid plus check from Medichecks after reading all the info...