I have had blood tests back from Medichecks and will appreciate some input on next steps. About a week after my post a couple of months ago I had my levothyroxine dose increased to 125mg a day. Further to advice I received from members who read atheists post I dealt with folate and selenium shortages. I am now due to have a test at surgery next week to see result of increased levo dose In order to get a detailed set of results I used Medichecks again
I clearly need to deal with the Vit D issue. I am also wondering if I should now request a referral to an endocrinologist with thyroid experience. I found one on the list from Thyroid UK. I am sure I will feel better when Vit D is sorted.
My concern is that as I am diabetic and this can cause t4-t3 conversation plus my age, now 67 that the decline in ft3 in last two months suggests to me that the time has come after 55 years being underactive to get back to the healthy me I was on ndt.
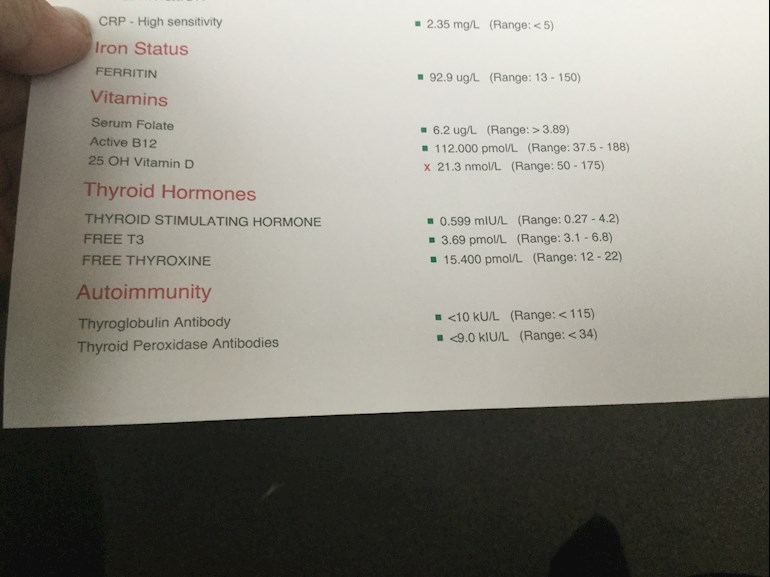
Test result in photograph, thanks for help.
Written by
Miffie
To view profiles and participate in discussions please or .
"Treat for Vitamin D deficiency if serum 25-hydroxyvitamin D (25[OH]D) levels are less than 30 nmol/L.
For the treatment of vitamin D deficiency, the recommended treatment is based on fixed loading doses of vitamin D (up to a total of about 300,000 international units [IU] given either as weekly or daily split doses, followed by lifelong maintenace treatment of about 800 IU a day. Higher doses of up to 2000IU a day, occasionally up to 4000 IU a day, may be used for certain groups of people, for example those with malabsorption disorders. Several treatment regims are available, including 50,000 IU once a week for 6 weeks (300,000 IU in total), 20,000 IU twice a week for 7 weeks (280,000 IU in total), or 4000 IU daily for 10 weeks (280,000 IU in total)."
Each Health Authority has their own guidelines but they will be very similar. Go and see your GP and ask that he treats you according to the local guidelines or this summary and prescribes the loading doses. Once these have been completed you will need a reduced amount (more than 800iu, which is the usual amount prescribed after loading doses, so post your new result at the time for members to suggest a dose) to bring your level up to what's recommended by the Vit D Council - which is 100-150nmol/L - and then you'll need a maintenance dose which may be 2000iu daily, maybe more or less, maybe less in summer than winter, it's trial and error so it's recommended to retest once or twice a year to keep within the recommended range. You can do this with a private fingerprick blood spot test with an NHS lab which offers this test to the general public:
Your doctor wont know, because they are not taught nutrition, but there are important cofactors needed when taking D3 as recommended by the Vit D Council -
D3 aids absorption of calcium from food and K2-MK7 directs the calcium to bones and teeth where it is needed and away from arteries and soft tissues where it can be deposited and cause problems such as hardening of the arteries, kidney stones, etc.
D3 and K2 are fat soluble so should be taken with the fattiest meal of the day, D3 four hours away from thyroid meds if taking tablets/capsules/softgels, no necessity if using an oral spray
Magnesium helps D3 to work. We need Magnesium so that the body utilises D3, it's required to convert Vit D into it's active form. So it's important we ensure we take magnesium when supplementing with D3.
Magnesium comes in different forms, check to see which would suit you best and as it's calming it's best taken in the evening, four hours away from thyroid meds if taking tablets/capsules, no necessity if using topical forms of magnesium.
Check out the other cofactors too (some of which can be obtained from food).
You are undermedicated to have such low in range hormone levels - FT4 and FT3. Dr Toft, past president of the British Thyroid Association and leading endocrinologist, states in Pulse Magazine (the magazine for doctors)
"The appropriate dose of levothyroxine is that which restores euthyroidism and serum TSH to the lower part of the reference range - 0.2-0.5mU/l.
In this case, free thyroxine is likely to be in the upper part of its reference range or even slightly elevated – 18-22pmol/l. Most patients will feel well in that circumstance.
But some need a higher dose of levothyroxine to suppress serum TSH and then the serum-free T4 concentration will be elevated at around 24-28pmol/l.
This 'exogenous subclinical hyperthyroidism' is not dangerous as long as serum T3 is unequivocally normal – that is, serum total around T3 1.7nmol/l (reference range 1.0-2.2nmol/l).*"
*He recently confirmed, during a public meeting, that this applies to Free T3 as well as Total T3.
You can obtain a copy of the article by emailing Dionne at
tukadmin@thyroiduk.org
print it and highlight question 6 to show your doctor.
If you were well on NDT, maybe you should consider going back on it. Thai NDT can be brought without prescription and many members do well with it.
Content on HealthUnlocked does not replace the relationship between you and doctors or other healthcare professionals nor the advice you receive from them.
Never delay seeking advice or dialling emergency services because of something that you have read on HealthUnlocked.