Introduction
Through the practice of mindfulness observation and discussions with many people I have come to various conclusions concerning fascia. I have discussed mindfulness as used by myself together with its problems in a previous post. I have found by inquiry that many medical students do not cover the intricacies of fascia in their medical courses. The reader needs to do their own investigations to determine the truth or error of what I have presented. These investigations need to use mindfulness.
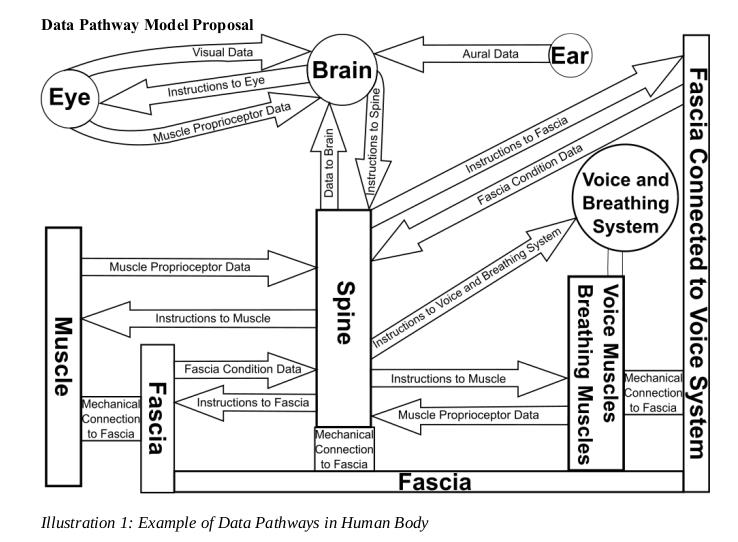
Fascia forms a continuous tensional network throughout the human body, covering and connecting every single organ, every muscle, and even every nerve or tiny muscle fibre. The first International Fascia Research Congress was held at Harvard Medical School in October 2007.
The fascia has thousands of nerve endings which feed into the brain. It has contractile components which can contract and relax. I have given a proposed diagram of the data pathways.
A helpful book on fascia is “Fascia what it is and why it matters” by David Lesondak ISBN 978-1-909141-55-1.
The arguments I present need to be investigated by the reader to see if they hold true for them. A principle mode of investigation is meditation and mindfulness. Meditation to develop the skills to enable quietness of the mind and mindfulness with a light touch to observe what takes place.
Emotions are felt in the body. I believe that fascia is what determines to a very large extent the emotions that are felt and the brain interprets and acts upon the felt emotions. The brain sets the tensions in the fascia by various means (physical and chemical) and then interprets these emotions by feedbacks from the fascia to the spine and then from the spine to the brain. If the feedbacks are very high (whatever this means) then the brain starts to get overloaded. A system’s stress breakdown point in the brain is reached with the resultant fall in ability to do things well. These overloads are what have caused people to seek help from psychiatrists. This may not have been as helpful as they would have liked. Psychiatrists listen to and observe what the patients say and do. Psychiatrists never consider or observe the patient’s fascial state. Psychiatrists could by their actions enable a more problematic state to develop in patients. Psychiatrists often ignore how patients use language when drawing conclusions. The deep fascial state cannot be observed.
I have come to the conclusion that particular fascial tensions determine what thinking processes the brain engages in. Fascial tensions are determined by environment (both social and physical), drug-taking regimes, muscular habits, human gut microbiome, and brain instructions.
The above is a matter of personal investigation to determine its truth. This investigation takes time because lots of observations (though mindfulness) need to take place before enough variability of events and response have been observed and assimilated. The data that has been observed and remembered can develop new conclusions or test the truth or error of my reasoning. The therapist the patient sees cannot determine this truth. No therapist or machine can determine what the actual internal state of the patient’s fascia is, nor how this state impacts on the patient’s thinking.
Drugs
When a person takes a drug what happens? The drug affects the body. Drugs diffuse all over the body. The amount that resides in different places depends on the drug and drug amount. The drug has an effect on the fascia due to the drug’s presence in the fascia. The drug has an effect on the brain which in turn sends some sort of message to the fascia. What effect the drug has can depend on the state the fascia is already in. This is why drug psychiatric side effects can be a very variable quantity. The fascia informs the brain of its state. The brain then responds with a thinking process regime that has dependence on the inputs it receives from the fascia.
The discomfort in the fascia can be become considerable. Drugs or alcohol can dull this pain or replace the discomfort with non discomfort and maybe the fascia sending pleasurable signals to the brain. Drugs and alcohol can be problematic because they interfere with the brain’s ability to think and respond well. By pleasurable I can mean signals that generate less discomfort.
Psychological and psychiatric Issues
As a result of the effects of long term physical health disabilities I have had the experience of having to see both psychologists and psychiatrists. I have engaged in talking therapy. I have engaged in physical therapies. These different therapies produce different results. My engagement with psychologists and psychiatrists has in the long term created a lot of potential problems with how the medical professionals interpret my medical notes. Psychologists and psychiatrists when they see a patient can have a doctor who states they cannot find anything wrong. This can lead to the assumption that nothing wrong is present hence the patient has a mental problem. The issue of the doctor or consultant not being competent to find a physical problem is often not on the considered agenda.
My experience is that what I tell psychologists and psychiatrists is recorded by them differently from what I have told them. Events that have never ever been discussed or have never taken place get entered into the medical records as having taken place. This lack of accurate recording happens often. There is a lack of reliable patient records. Thus, how can it be possible that a psychological or psychiatric diagnosis be researched for best treatments? If the fascia is playing a part in the way the brain responds and the psychiatrists and psychologists are ignoring the fascia response, how can the treatment options they offer be effective and efficient?
There are two genders and people with different sexual orientations. In the two genders there are sexual genetic characteristics and a wide range of psychological orientation characteristics. My experience is that the two genders male and female can and often do respond to the environment very differently. It seems logical to assume that the effect of an environmental stimulus on the fascia could be different for the two genders. On certain issues the two genders have a very different fascial response. It seems logical that an environmental stimulus input to the brain which then sends a response to the fascia is different for the two genders.
I have found that a number of members of the female gender are demanding that the male gender should have the same response that they have. If they do not there is something wrong with the male. This can develop into something very bad as the male gender’s fascia develops into a particular emotional tension which the brain can then release into violence against the person who is perceived to indicate that there is something wrong with them, or they can carry this tension which can be released against a bystander who caused a very minor irritation. How can this violence be prevented? A friend of mine was murdered 50 years ago. I came very close to killing someone 55 years ago and was very lucky there were others around to stop me. I am thinking of all the injuries that are being given to people by others. I am thinking of lifetime of pain these injuries can cause both to the victim and to the perpetrator. I am thinking of lifetime of pain that can be caused when messages from fascia in a particular state overload the brain or set particular responses in motion. Many in Painconcern suffer sleep problems which in turn because of brain response has an effect on the fascia. This effect may create dangerous emotional tensions. I will never forget a clinical neuropsychologist who worked in the NHS stating under oath in a court of law: “Losing an hour of sleep per night has no effect on one.”. The court case had a negative mental effect on me for years afterwards.
When I was growing up I was told to count to ten when angry. When experiencing the anger response I was often too emotionally upset for this to be effective.
I appear to have wandered off the topic for Painconcern. I hopefully can explain how this relates to many on Painconcern. We have a hidden disability which others cannot see. Many others who cannot see our very real pain (particular some of those who have some authority) can imply accidentally or deliberately that we are making the problem up or that we have some mental deficiency. This is an attack on our self worth and the anger and sometimes intense rage which we have to suppress does not do our pain or our relations with others much good.
The anger we have developed we try to suppress mentally. This is important for social reasons. I think we can engage another way that is far less exhausting. And more efficient and effective. We can decide to set ourselves the task of moving in a gentle manner. This changes the state of the fascia. This changes the feedback of anger from the fascia into the brain. This in turn reduces the input into the brain that demands action. When I was growing up I can remember the films showing the irate lady throwing things at the man who had upset her. (I know this is non PC). I can remember 40 years ago an aunt telling me that when she got really upset about something she would buy some very cheap second hand plates and then smash them. She told me that she felt wonderful afterwards. These women had by movement moved the state of their fascia from one state to that of another. A number of men I know when they have got upset went for a walk. They found that their emotional state changed during the walk. The walk has modified the state of their fascia.
There have been many cases of people who are ready to jump off a high building. A good citizen goes to talk to them and they decide not to jump off the high building. I was taught that this was because someone had talked them out of it. Was the real reason that someone had spoken to them and the person thinking of jumping had re-orientated their body to the person speaking to them? Their re-orientation had changed their fascia state and as a result the feedback into the brain from the fascia had changed. Following this as a result there was no longer the wanting to commit suicide thought process.
I have spoken to a number of people who had been admitted to a psychiatric hospital after a failed suicide attempt. In conversation with them there was a tacit acknowledgement of moving out of the suicidal state by moving the body. I.e. changing the state of the fascia.
A topic which causes grief, upset and pain to a lot of people is the accidental or deliberate injuring and killing of infants and children by adults who are supposed to be in a caring role. A local vicar told me a number of years ago about one of his parishioners. The parishioner was a well liked person. This person had shaken his child to death. The circumstances were that the parishioner, due to a range of circumstances, got very tired and exhausted because of work and night shift sleep issues. He was left on his own to care for his child. The child did something as children do to irritate him and he shook the young child to death. This was totally out of normal character. The person was over tired and exhausted and would have had a particular fascial state at the time of the incident. I believe that he reacted according to his fascial state at the time and coupled with tiredness had no means to inhibit his response of extreme anger. The parishioner lives with the pain that his actions caused to others and his own pain for killing his child. If he had understood the state his fascia was in he could have knowingly changed it. It is possible to change the fascial state to prevent further tragic events like his. I have met many people who have fascial states which are swift to anger and react. I am careful around those people. I have learnt that when my fascial state gets into certain states I need to avoid people.
The headlines talk of evil people. The psychiatrists talk of investigating (history taking) why these people did what they did. The history taking never considers the state of the person’s fascia present at the time of the problematic event. There is a lot of talk about mental health issues with the brain in isolation with the body having no part to play.
What has the above to do with Painconcern? Painconcern deals with issues of pain and how to reduce pain and discomfort. Emotional states can be painful or at least uncomfortable. Extreme emotional states can occur by taking the wrong approach to tackling minor emotional issues.
I believe that if my understanding about fascia is correct or is along the right sort of lines then there are methods with which we can engage that can reduce pain and discomfort. There are methods to change how we feel. These methods involve movement and observing movement. The development of these methods requires the use of citizen science, meditation and mindfulness. The methods cannot rely on the written or spoken word to develop. The methods rely on doing, experiencing and modifying.
I have been looking at methods for a long time without actually formulating anything. Different things work for different people because of various innate skills that people possess.
I have as a result of my road traffic accident and the events that followed it experienced many uncomfortable and potentially destructive emotions over the years. I have found from experience that handling the experienced emotions can be exhausting with long term after effects that interferes with my ability to do things.
I will begin to discuss these methods in Part 2.
