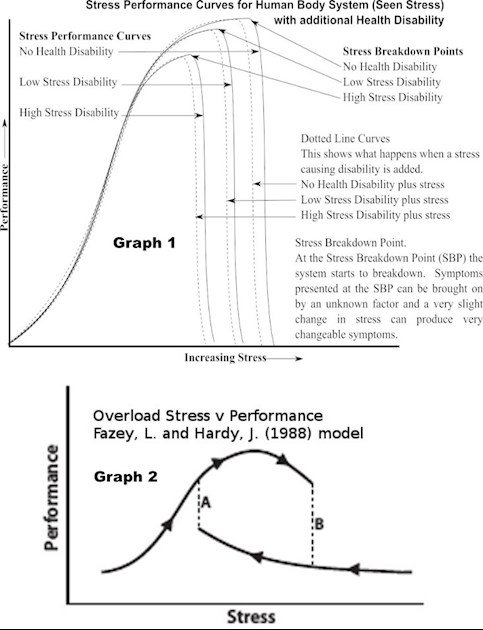
In this post I will discuss present my attempt to describe my thinking on the concept of Stress Breakdown Point. The stress – performance curves are models to work with and will vary from person to person depending on environment and health disability. In the graph we have Stress versus Performance for three conditions: A person with no Health Disability; a person with a Low stress disability; a person with a high stress disability.
In the graph 1 we can see that at low stress we have low performance. As the stress increases the performance increases until we reach a point where a slight increase in stress causes a collapse of performance. This point is called the Stress Breakdown Point. The graph indicates that when the stress falls just below the Stress Breakdown Point the performance increases again. In reality this may not be what always happens. Graph 2 below the top graph shows increasing performance with stress. At point ‘B’ there is a sudden drop in performance. The stress has to drop considerably to ‘A’ before the drop in performance can recover to what it was.
Which graph is an accurate portrayal of events in the management of a chronic health disability. My experience is that both graphs have a semblance of truth. Which graph I must consider when managing my disability I have to rely on experience built up over the years. In some types of stress graph 1 is the stress – performance behaviour I experience. In other types of stress graph 2 is the stress – performance behaviour that I experience.
For example: there are the DWP forms. They are stressful. When I first look at the form I am in Graph 2 mode. My stress has got too high. I have to put it down and leave it for another time. This another time is often a few hours away. Looking at it got me to ‘B’ and I have to get the stress down to ‘A’ before I can handle the form again. I have to look at the form more than once before I can begin sensibly manage it. At this point my stress – performance behaviour becomes like that of graph 1. I have to work to have the stress high enough for reasonable intellectual performance in tackling the form, but not so high that I go over the Stress Breakdown Point. It entails doing a little bit. Leaving it for while and then coming back to it. As well as monitoring myself to ensuring that muscle stress does not increase my pain levels.
My DWP form is complex because I have to explain so many factors as to why I cannot do things. Why I am capable of getting past a job interview and yet I will be sacked within two weeks. The effect of pain and the effect of pain causing sleep problems. The exhaustion of constant monitoring of my condition and the sudden collapse of my ability to do things because the brain says I have to rest I am not doing any more until I get a rest/sleep.
My experience is that my condition is sometimes “Low Stress Disability” and sometimes “High Stress Disability”. For example on a nice sunny day I have “Low Stress Disability”. On a damp day that is not quite raining I have High Stress Disability”. This is where it gets interesting. I am on a different stress- performance curve. I have to remember that the internal stress that gives me maximum performance on my “Low Stress Disability” will put me in the total system collapse and incompetent zone of the stress -performance curve. I had to learn these things by trial and error. With much social embarrassment on occasion.
Graph 1 shows the stress – performance curve of no health disability and the internal stress where maximum performance is. Graph 1 also shows the stress – performance curve of health disability. It shows something interesting the lower maximum performance and the lower stress capability. When we first experience the chronic health disability we are going to have to live with we have a remembrance of how much internal stress we needed for maximum performance when we had no health disability. We have a task to do which we want to do effectively. We ramp up the internal stress. We ramp up too much internal stress and we go over the “Stress Breakdown Point” for our new condition of having a health disability. We have to take time to learn at what internal stress we have are maximum stress. Again this is a situation of much trial and error. Because we must also take account: of the sleep disturbance stress caused by the health disability; the stress of failure to meet social oblations that we once could meet without difficulty; the stress of actually navigating the health disability. We must take account of these stresses when we ramp up our internal stress to get effective performance.
I have attempted to explain the stress- performance curves of graphs 1 and 2. The curves are working models with which to approach the handling of the short comings that we experience with a health disability. I have not explained all the researches I have done in this area. I limited by my ability to describe things in writing. I can only signpost things for investigation into the better management of a health disability.
In summary. I find that I can change the Stress Disability because of known or unknown environmental factors. Sometimes I have a low stress health disability. Sometimes I have a high stress disability. Sometimes I find that my capability recovers easily if I have gone over my Stress Breakdown Point and drop the stress. Sometimes I find my capability takes some time to recover if I have gone over my Stress Breakdown Point and I need to drop the stress quite a lot before I recover.
Lastly. We need to investigate to determine our stress – performance characteristics. We need to recognise that the stress – performance characteristics can change and we need to investigate so that we know when the stress – performance characteristics have changed. All this takes time. We need to give ourselves time. We need to allow ourselves to make performance mistakes due to internal stress miss judgements. And to be able to spot we the performance mistakes are occurring because of internal stress miss judgements.
My method for handling a internal stress miss judgement that effects performance is to stop what I am doing at that time. Do nothing for a short while and start again at hopefully a lower internal stress. This I admit took me a little while to learn (years). I had to re-invent the wheel for myself. Hopefully those reading this can design a better wheel than what I have.
