From early on in my cancer journey, I have been interested in the role of cholesterol in cancer(s), of which I have two, PCa and CLL. Cholesterol seems to be a major player in both of them. It is also one of my 4 Horsemen of the PCa Apocalypse (so named by Don Pescado) of Glycolysis, Inflammation, Cholesterol, and Hormone Balance.
This summary research article is the best explanation I have come across that describes cholesterol's role in cancer. It is quite technical for those of us who are not trained bio-chemists and is not completely specific to PCa, but even for those who do not care to delve into the complete metabolic actions that take place, it is still packed with insights that we can each use to make decisions about treatment options, scrip drugs, supplement choices, and aspirational diet and lifestyle goals.
This passage from the report highlights the need for all cancer patients to be knowledgeable about cholesterol:
"As evident from numerous studies including pre-clinical, clinical, meta-analysis, and population-based studies, cholesterol plays a vital role in cancer risk, progression, survival, prognosis, and therapy [[21], [22], [23],37,45]. Alteration in blood cholesterol level is a very common phenomenon in majorities of cancers [22,37,45]; however, it is still not clear for most of the cancers whether decreased blood cholesterol level in the cancer patient is a cause or consequence of the disease."
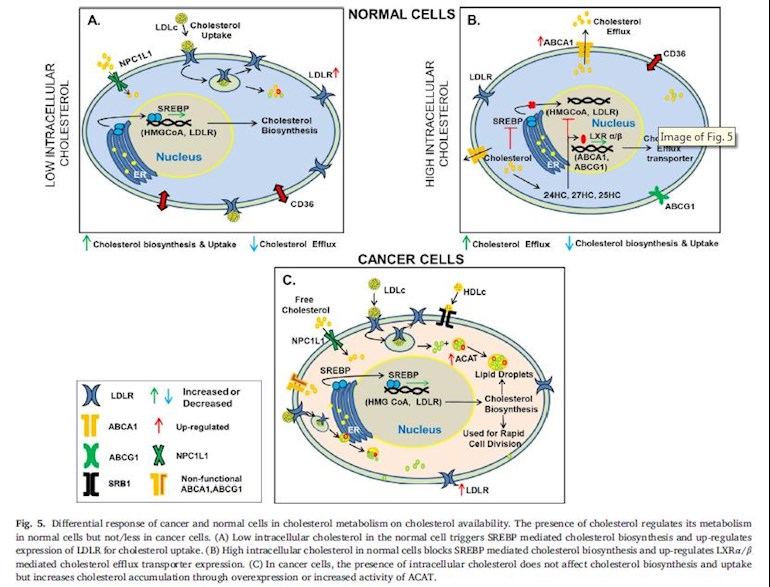
The illustrations in the report are first-rate and extremely useful in explaining in graphic form the roles of cholesterol in both normal and cancer cells. There is also a section that summarizes some treatment options for specific cancers. The research is mixed on the role of cholesterol in PCa. That section is reproduced in it's entirety below:
***
Prostate cancer
The relation between serum cholesterol and prostate cancer is complex. Few clinical studies indicate a link between high blood cholesterol towards increased risk of high-grade prostate cancer and the status of prostate specific antigen (PSA) [45,82]. The majority of epidemiological studies show weak evidence or no relation between blood cholesterol level and the risk of prostate cancer [83,84,85]. Even though the reports on the correlation of cholesterol with prostate cancer are conflicting, various studies suggest that non-identical races (black and white people) show a differential correlation between serum cholesterol and PSA levels. Increased blood cholesterol is highly correlated with increased PSA levels in the white population [86]. A population-based study from Stopsack KH, et al., demonstrate that lethal prostate cancer relies more on de-novo cholesterol biosynthesis instead of extracellular cholesterol uptake [87], whereas Singh G, et al., have shown up-regulated expression of LDLR in patient's tumor tissue samples. The increase in intracellular cholesterol inside the nucleus along with cyclin E overexpression in prostate tumor tissue indicates a potential role of cholesterol in regulating the cell cycle [88]. Also, metastasis of prostate cancer in bone causes an increase in cholesterol content as compared to the normal bone and these phenomena can be attributed to de novo cholesterol biosynthesis, supported by the influx of cholesterol through LDLR and SRB1 [89].
Studies in the xenograft model indicate the role of cholesterol in promoting tumor growth. Mice fed on a hypercholesterolemic diet with increased blood cholesterol level shows enhanced tumor progression along with induction of angiogenesis [90,91]. Moreover, in vitro conditions, upon treatment of prostate cancer cells with LDLc or cholesterol increased proliferation, migration, and invasion were observed [92,93,94]. Interestingly, prostate cancer cells lack a feedback mechanism for LDLR expression, even in the presence of excess LDLc, suggestive of the involvement of both pathways. In normal prostate cells, the expression of LDLR is tightly regulated and it decreases with an increase in LDLc availability [26]. Increased expression of LDLR is advantageous to prostate cancer cells as it facilitates enhanced uptake of fatty acids and cholesterol, which supports prostaglandin synthesis in cells [26]. Other than LDLR, Scavenger receptor class B type 1 (SRB1, HDLc receptor) was also found to increase in some prostate cancer patient samples [95]. Apart from these, androgen is required for normal epithelial prostate cell proliferation and differentiation. However, in advanced prostate cancer, cells can synthesize androgen by themselves in the presence of cholesterol, thereby making them self-sufficient for rapid cell division, independent of testicular and/or adrenal androgens [91,96].
Above mentioned studies illustrate both positive and negative correlation of cholesterol with prostate cancer. Clinical and preclinical studies highlight the role of cholesterol metabolism and LDLR in enhancing prostate cancer cell proliferation. The differential findings in clinical studies might be contributed in part by variability in the race and hormonal status, which needs further exploration.
***
The full report is here:
Influence of cholesterol on cancer progression and therapy
Translational Oncology - Volume 14, Issue 6, June 2021, 101043
sciencedirect.com/science/a...
Of special note to all prostate cancer patients is the following research on statins and PCa that is footnoted in the paper. It provides a caution to those who are taking satins as part of a treatment plan (self-directed or otherwise). It might cause you to take pause and reconsider whether that is a zero-risk strategy. Granted, the initial research was done in-vitro and in mice, but the follow-up patient profile study seems to suggest that there is, at a minimum, a sub-set of patients whose PCa could be made more aggressive by the use of statins. I suggest that anyone using them should read the entire report and come to their own conclusions.
That research (full report) is here:
Low-dose statin treatment increases prostate cancer aggressiveness
Oncotarget. 2018; 9:1494-1504
oncotarget.com/article/2221...
Be Informed and Stay Well, K9
