Hello HealthUnlocked Community,
I've written about the idea of pulsed therapy -- aka, adaptive therapy, although I find more acceptance (though not by much) if I refer to it as "modified watch and wait" -- here before, and wanted to give an update.
First a disclosure. as I've been warned by this site, I'm not an oncologist, this is a completely novel idea, at least as it applies to CLL, and may in fact be very dangerous, and certainly no one should take this as any more as something to discuss with their oncologists. All opinions here are solely my own.
The overview from 30,000 feet.
1) I don't like the idea of watch and wait, where treatment is delayed until you have symptoms.
2) I don't like that CLL therapies have very serious adverse events and potentially seriously diminish quality of life. Neutropenia is extremely common, it diminishes the ability of the immune system, and increases the chances of secondary issues including secondary cancers. [edit---as AussieNeil pointed out, while neutropenia can very well cause numerous health issues, neutropenia itself is not linked to secondary cancers. However, treatments, like BTK, are: cllsociety.org/2019/12/asco... ]
3) I don't like that extended treatment can often lead to resistance to drugs and diminished overall survival
4) I think the idea of trying to achieve uMRD sets up exactly the environment that will bring resistance, as the only cells left are necessarily those that are resistant, and as they are then operating in an environment without competition, they have the opportunity to rebound unchecked, in a process termed "competitive release," which has been applied in the field of pesticide use since the 1970s.
5) Because early stage CLL is rather indolent and it's eradication is virtually impossible, I speculated that rather than watch and wait, then going to a full blown attempt at uMRD, why not treat early, and only enough to keep the disease in the indolent phase. Effectively, just control the disease enough so you're asymptomatic and live with it as a chronic disease.
6) I can't say this is my idea. Gatenby has been doing pioneering work on this methodology for almost 2 decades and has been having stunning results with solid tumors, but not CLL. I spoke to him, and he believes the strategy is reasonable in CLL because the highest replication happens in the protected niches of the lymph nodes and BM.
7) Aside from Gatenby, who doesn't work in CLL, I found the community (4 oncoologists so far) are absolutely against this strategy, and I understand why. "We are having great results with current therapies" and "we have no idea what are the consequences of this novel approach." But with uIGHV and mTP53, the results don't look that great to me.
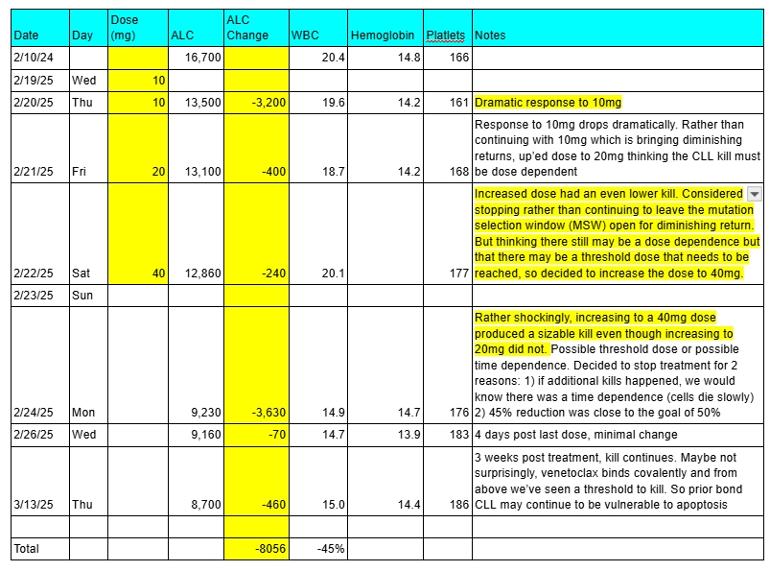
8) Fortunately I was able to find an oncologist, after considerable cajoling, to go along with the approach. I post the results below. I found it amazing that with 4 days of very low dose venetoclax, my ALC was reset back a year. At this point we don't know what the new doubling rate will be, what the other consequences will be, but the resistance window is so short and dose so small, it is very unlikely, though not impossible, that resistance could have been selected for. But biology is complicated and you just never know.
8a) By the way if you watch and wait until your ALC is very high, the chance of TLS increases significantly. I was worried about that even at an ALC of 17 and hydrated like a fiend.
9) if you look at the results so far you might find them stunning, I did. Just a 10mg dose brought a kill of 3000. A second 10mg does brought a minimal kill. A third 20mg dose brought a minimal kill, but a fourth 40mg does brought a kill bigger than the first, 3600. And even more stunning, 3 weeks post venetoclax, the kill is still happening. Which may not be too surprising because as we can see from just these results, there are threshold kills as evidenced by the 40mg kill, and we know venetoclax binds covalently. So there may be more CLL cells that have been compromised by the drug, but are slower to die.
10) Of course, all of this, and everything I am writing is open to interpretation and criticism. But no one is trying the idea of treating CLL as a chronic disease and instead are only in two camps, watch and wait, if you're lucky enough, and treat to uMRD. If miraculously, somehow Gatenby has come up with an idea that translates to CLL, it could potentially be a watershed approach to CLL that cuts costs to next to nothing and dramatically reduces adverse events.
11) So I'm a clinical trial n=1. I will share my results as they continue, and welcome your thoughts, even if highly critical, it's OK, I know I am out on a limb here.
All my best and thanks to everyone in this great community.

")
