As I followed my Pca story, I have now changed focus from straight genomic mutations [AR mutations,etc] to what I see as a new focus on how Pca treatments induce senescence and how this senescence is a double edged sword. The following clinical article is a newer view:
file:///Users/podsart/Downloads/fimmu-15-1395047.pdf
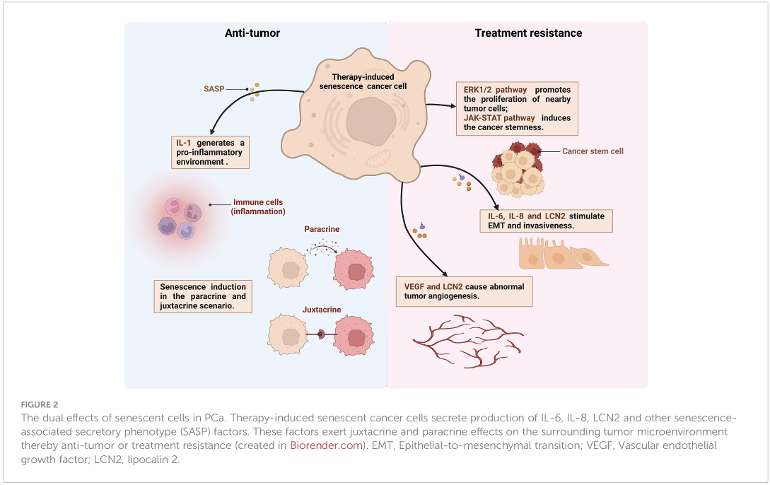
The above figure is from this article [couldnt get the second figure to be added, it keeps replacing the first??]
From a previous thread on this subject, I got the sense that our Pca treatments first can effect aptosis and actually kill the Pca cell and then the treatment tends to produce these senescense cells that have a good and bad side, as shown above and described in the article [hopefully the above link works.
In my case, I am trying to ascertain the optimal strategy, given I have already progressed on 2 sequential AR monotherapies [xtandi then erleada]. They have just started me on relugolix ADT. My PSA is now very low after just emerging from undetectable, I am sure it has acquired a more aggressive nature and can therefore progress rapidly from here, so in my view, the current low PSA is temporary. Also, I am sure I already have a lot of senescence cells.
Given the above, does it make sense for me to add another systemic therapy such as chemo [which I never had], perhaps inducing more scenescense, with the above associated good/bad duality? What about Provenge, which the article doesnt address? Does Provenge also induce senescence?
How do you chose and optimal strategy. Would appreciate your views.
