I'm curious if anyone has had any discussion with their MO or Radiation Oncologist about having to take a longer course of Orgovyx compared to Lupron or other longer acting ADT drugs because Testosterone comes back so much quicker on Orgovyx? It would seem to me, 6 months of Orgovyx is like the equivalent of maybe as little as one Lupron shot.
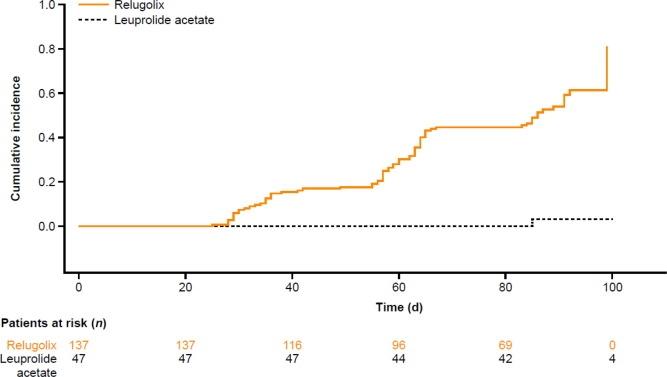
Here's what the comparative T recovery looks like which to me seems like Lupron keeps working for months after your last shot (which is pretty common knowledge here but the graph really illustrates it.) Extrapolating out I'd say it's plausible to get the equivalent effective time of castration you'd have to take Orgovyx an additional 4-6 months! So 10-12 months Orgovyx = 6 months (2 shots) Lupron.
Written by
jazj
To view profiles and participate in discussions please or .
Orgovyx starts suppressing T faster than Lupron. If one is taking it adjuvantly with salvage radiation, there is no trial data for comparable periods of taking the drug or time since T recovery. For men with distant metastases, it doesn't matter because they are suppressing T permanently.
The time to castration and time to testosterone recovery for Lupron are nowhere near equal so the longer time to castration with Lupron of about 4 weeks/1 month longer isn't going to offset the fact the T recovery of Lupron is about 1/6th the level of Orgovyx at 3 months post-treatment.
Yes in the context of advanced metastatic stage treatment it makes no difference except in the case of Intermittent ADT because the patient will be on it constantly until the cancer becomes castration resistant. But in the context of concurrent treatment with initial or salvage radiotherapy or intermittent ADT I do think the math here is significant.
At minimum the study is showing that the total time of castration is AT LEAST 2 months more for Lupron vs Orgovyx for the same treatment duration. However realistically the equivalent difference is probably significantly higher than two months since the Lupron patient post-treatment after 3 months may have just exceeded castration level, but due to having a much lower T than the Orgovyx patient is still getting significantly more therapeutic effect more than 3 months post-treatment. If one were to assume the rate of cancer progression is roughly linear to the level of Testosterone up to maybe say half the normal T level, the actual equivalent effective treatment period would probably closer to 4 months. For sake of argument, let's be conservative and say there's a 3-month effective T reduction difference.
In the context of initial or salvage RT, there are many studies evaluating all different lengths of ADT treatment including 3 months, 4 months, 6 months, 12 months, 18 months and 24 months. Granted the 2-3 month difference is not that significant probably starting at 12-month ADT or greater but can be significant for 3/4/6 month intervals and VERY significant in the context of IADT.
My question basically boils down to in those three scenarios (initial & salvage RT or IADT) are MOs prescribing Orgovyx recognizing these major differences in pharmacodynamics and "doing the math" or just oversimplifying that x months ADT is equivalent despite which drug is used?
I'd question the intelligence (or maybe better termed independent thinking) of any MO that hasn't discussed this with patients in these three circumstances.
This also would make a difference on ADT timing of initiation when used during RT. I believe there is good evidence neoadjuvant ADT combined with subsequent RT had no benefit. So if the goal was to have castration at the beginning of RT, you could start Orgovyx 5 days before, where with Lupron you'd want to get your shot a month before starting RT.
I still postulate that if for example a past study only showed benefit of adjuvant ADT therapy with RT for at least 6 months (two Lupron shots) the actual duration of castration was 9 months. Which given the slower time to castration of 1 month means the effective duration of ADT on Orgovyx would be 8 months not 6. But since it's not an on/off switch, realistically I'd say based on median T levels, the equivalent of 2 lupron shots over 6 months would be a 10-month course of Orgovyx pills.
If the measurement in most studies of duration of ADT treatment is based on length of time blood T was at castration level and not on duration the patient took the ADT treatment drug, then my hypothesis goes out the window.
Not in all cases. I believe there are other patients (some on here) that did ADT for < 12 months in conjunction with initial or salvage RT and other patients doing intermittent ADT or BAT. The large difference in the pharmacodynamics I believe is a consideration in those cases. But not in patients that are High Risk or Metastatic Hormone Sensitive where indefinite constant ADT is the SOC. This forum is not only useful in informing patients who are already at an advanced stage of PCa but patients in earlier stages that want to learn about earlier experiences of those patients and the treatment decisions they made along the way.
I wouldn't doubt that as you're on top of the studies. It appears to date it's only been studied as an adjuvant to RT as far as safety and effectiveness (for testosterone ablation.)
"2 randomized clinical trials of 260 men with prostate cancer who were receiving treatment with radiotherapy"
It hasn't been around long enough I suppose to do studies in the RT setting with endpoints like PCSM or MFS with various durations compared to the other ADT drugs.
It's been more widely used now in various settings. I was just curious if anyone taking it as an adjuvant to RT if their Radiologist or Oncologist told them they would need to take it longer than Lupron because their T level would not remain suppressed as long when they ceased treatment.
I added 'As Adjuvant to RT' to the title to better describe what I was asking about. As you point out, my question doesn't really make sense in the context of metastatic PCa or post initial/salvage RT (except in the case of IADT which I assume you're not a fan of because it's not as effective as continuous ADT?)
Indefinite ADT is not the SOC for high risk...unless you mean men who do only ADT and neither surgery nor RT? Also, you said something about linear relationship between T level and PCa progression? Really? In what setting? Good discussion. I'm sure almost all ROs are bright enuf to understand the different recovery times for Lupron and Orgovyx!!
The linear relationship between T and PCa progression is the linear portion of the Morgentaler Saturation Curve, which occurs for T < 250 ng/dl. In this linear regime, the PCa growth rate is proportional to the T-level. This is the fundamental basis for doing ADT.
This is for men who have been treated with RT or surgery and have recurrence? It is a model.....based on studies I suppose? Obviously, if a man is "cured" this wouldn't apply. Seems too simple to me.....but no expertise !!!!
Interesting.....using Google scholar, found nothing re Morgental Saturation Model???
I think I misspelled his name. It's Abraham Morgentaler. He's published over 170 papers on testosterone and written a patient's guide to testosterone called "Testosterone for Life". It's a good, easy read with two chapters on prostate cancer.
The supporting data is based on PSA vs T.
PSA is proportional to the integral of the cancer growth rate over time. So, they are related.
Here is the supporting data that shows a rollover and saturation in the average PSA curve fit for T > 200-250 ng/dl. For T < 200 ng/dl, the PSA is proportional to T, especially in the linear range (T < 100 ng/dl). There is a lot of scatter in PSA because other factors influence PSA, including, but not limited to: infection, inflammation, age, prostate volume, and BPH. Lower T (below 200 ng/dl) predicts lower PSA, which is the fundamental basis for doing ADT in castrate-sensitive men. This curve doesn't apply to castrate-resistant men (by definition, ADT stops working).
This PSA vs T data is for any castrate-sensitive man diagnosed with prostate cancer, not just after RT or surgery or recurrence.
I have additional data that supports the linear portion and saturation portion, but I can only post one plot at a time...
Anyone who is castrate-sensitive can track their PSA versus T and can make this plot for themselves. It applies primarily for short periods of time, for example, after decreasing T due to Lupron ADT, or increasing T with supplementation.
This confirms what my common sense hunch was. So any MO during the initial/salvage RT or IADT setting that is basing recommended ADT on studies to date, yet offering the more convenient pill form of Orgovyx (with less potential for cardiovascular side effects) needs to factor in if it takes 90 days for T to get to a measly 50 on Lupron, so it could be close to a year before you reach the rollover point, whereas with Orgovyx based on the graph you reach the rollover point in around 45 days!
This is probably only really going to be a major consideration for patients receiving RT who are High-Risk as Intermediate Low-Risk patients don't appear to have the same long-term benefit of adding ADT to RT. But this is especially significant for Advanced Stage patients doing Intermittent ADT. I'm unfamiliar if there is a prominent drug choice used in this type of treatment but if it were Lupron and you were doing IADT, you would effectively be on partial ADT during the off-treatment period whereas if you used Orgovyx for IADT, your median T levels during the off-treatment period would be multiples higher than Lupron! I would assume MOs are using shorter acting drugs with IADT than Lupron? This would also be very significant for those doing BAT. In that scenario Orgovyx may be far superior than something like Lupron so you can much more quickly switch from low T to high T.
Sidenote: I don't think either of those treatments are SOC therapies? I believe I read one study where patients doing IADT general had a little over a year shorter survival. But that is the trade off, go through less total duration of ADT side effects along the way when you are younger in exchange for moderately less-effective long-term survival. That would be a tough decision for many I think if for example your MO said you could go through 4 years of ADT side effects and live 10 more years versus a cumulative of 2 years off/on ADT side effects and live 9 more years. But this is really a subject for an IADT thread.
" I'm sure almost all ROs are bright enuf to understand the different recovery times for Lupron and Orgovyx!!"
Honestly, I'm not so sure about that. Hence why I posed this topic in the first place. I think the problem is most people on here did their RT or SRT before Orgovyx was commonly prescribed for ADT. Currently, I can't think of a reason why anyone would be doing Lupron shots instead of taking Orgovyx unless their particular insurance didn't cover it. The other problem is you'd have to be careful to pose the question of treatment regimen differences between the two without the question being too leading to truly see if the RO recognized the significant difference in pharmacodynamics that would potentially indicate different treatment timing and duration.
I'm not going to assume one way or the other but it would not surprise me to hear reports especially from smaller clinics that the RO recommended "X months of ADT" or x months on and y months off for IADT, regardless of the drug prescribed. Just a hunch at this point though based on many conversations with about different doctors over the years. There is a varied level of knowledge between providers.
To answer your question directly: I've been treated in the situation you describe by the most experienced proton MD in the world at California Protons and my MO at the City of Hope is considered one of the best. None of my 3 times treated has either mentioned the need for a different length of ADT based on the choice of drug.
You bring up an interesting thought for sure, thanks!
I am in the situation of having done salvage radiation and adjuvant ADT. I still have hope for "cure" and I am grateful for everyone in here, further in their journeys, charing their stories, thoughts and knowledge. When my RO suggested ADT with the RT he said 24 months of bicalutamide or 6 months of Lupron. When I read about Lupron and realised about T recovery time I told him that 6 months was false marketing. He answered that I was absolutely right and that 6 months means more 9 to 12 months. On your question I wonder why it isn’t mandatory to describe the obvious to the patient (and then also the obvious difference between drugs).
it seems like the data says the longer the antitestosterone the better the chances. In many cases they shorten the course to 6 months because they are balancing side effects with the relatively small benefit of lengthening the course. You would need head to head data to see how much shortening it to 6 months on Orgovyx versus 6 months on Lupron effected the outcome.
This retrospective study of 10,000 men showed a maximuum overall survival benefit with 19 months of ADT......but for distant metastasis-free survival and prostate cancer specific survival for high risk men, the longer the better.....but the benefit curves included in this study indicate added benefit past 10-12 months is modest compared to 1st 10-12 months. So, as an RT patient, a man can shoot for the longer duration,
I've ran across the HERO study several times comparing Orgovyx and Lupron. They are very similar as far as most side effects with less chance of cardiovascular events and a little less effect on blood pressure with Orgovyx but with a moderately higher chance of diarrhea. Anecdotal reports of patients that took both and said Orgovyx has less side effects might be attributing it to the side effects going away quicker after the last treatment, or, there may be a small subset of patients that their personal biology lends itself to be less prone to the side effects of Orgovyx compared to Lupron. But in studies involving many patients there wasn't a significant difference in the common side effects like hot flashes and fatigue.
622 patients.
The most common adverse event observed was hot flashes (54.3% vs. 51.6%), followed by mild-to-moderate diarrhea (12.2% vs. 6.8%) and hepatic dysfunction (1.4% vs. 1.3%) in the relugolix and leuprolide groups, respectively. The major cardiovascular events (6.2% vs. 2.9%) and fatality (2.9% vs. 1.1%) were higher in the leuprolide group.
As mentioned above I am one of those on this forum who has PC but at least for now has not spread by measurable scan data. That does not rule out microscopic spread for now. I come here because if it does spread I have learned some valuable lessons based this forum versus a generic PC forum.
I had the exact same thoughts as the original post and planned my treatment based on that. My original thought was 6 months of Lupron preceded by one month of Casodex to stop the flare of T would because of the residual impact of Lupron would actually get me about 9 to 10 months of effective treatment. Once again this was my thinking based on what I had read about T recovery time.
Not very scientific but based on blood work after my radiation I actually got that extended to between 2 to 3 months effective dose rather just 6 months advertised by taking Lupron.
It just seems to be the short response of T coming back on Orgovyx versus the extended length of T on Lupron would give you this added boost of time.
Once again no real studies to back up my logical reasoning but it proved correct in my case.
Great question! Related to that question is the question about ADT duration when an ARPI is added along with radiation (and also whether it’s hypofractionated or ultrahypofractionated -SBRT).
My experience is as follows and will continue. Before having salvage radiation I was started on ADT using Orgovyx. After 5 weeks blood tests showed it didn't work for me, my T levels did not drop below 250, let alone to the level desired. I was then given a 1 month shot of Firmagon which pulled the T down in 2 days. After that month I was put on 6 month shots of Lupron. I also started abiraterone at this time. In May I will be coming off the Abiraterone/Prednisone. My last Lupron shot was in November. I have met other men with similar results. We're all a little different and react differently to treatment/medication. At the point in May I begin periodic blood tests checking on T level recovery and PSA. Not sure what you are looking for, but my oncologist and I are very happy with my progress and interaction with treatment. I look forward to a return to some normalcy, 1 or 2 month difference doesn't matter.
Very interesting that apparently, your GI system didn't absorb the drug as I believe someone mentioned Firmagon acts in the same was as Orgovyx? That is most likely very rare or else the studies would show a significant portion of the patients being non responders and I haven't seen that.
Very possible. One note to that, I have AB+ blood - AB blood types have less gastric acid than other people and can have difficulty with absorption of vitamins/minerals & medications. Injections usually work better for particular things. I closely watch particular levels in my blood as this also causes me to "bounce along the line" of anemia. As I often mention, we are all different and treatments need to be monitored and adjusted.
jazj, I’ve just finished my first month on Orgovyx as an ADT. My RO included it as an option to Lupron specifically because it offers more rapid on/off hormone deprivation effects. I selected it for both that reason and because the SEs are reportedly less severe. My RO never discussed the details you’ve elaborated on in your post. What she did say about ADT, as an adjuvant treatment to RO, is that ADT tends to shrink and weaken the cancer cells and make them more susceptible to injury from radiation. She said it takes a couple of months on ADT for the cancer cells to be affected. Hence, the 2 or 3 month regimen prior to EBRT.
That is interesting. Studies I've read seem to conclude that neoadjuvant ADT is of little value for most men. Concurrent/adjuvant ADT provides more benefit. When I mentioned need to take ADT 1-2 months prior to ADT, Harvard-trained RO suggested not necessary..take concurrently/adjuvant. Intelligent people can disagree .
Finishing my previous post, I intend to embark on my own version of IHT. It will probably be some version of six months on, six months off—without the objective of achieving zero PSA readings. My RO is not enthusiastic and is pushing for 9 months minimum post RT. Here’s where I really don’t get it—how do you know if the RT has been successful if you don’t clear yourself of ADT and then monitor your PSA? My understanding is a male should achieve a nadir in PSA levels post RT, assuming it’s had some success.
Finally, re SEs, so far I would categorize them as mild. Granted, it’s only been one month. Here’s what I’ve noticed: I don’t sleep as well as I did, I have hot flashes at night mostly, I’m trading muscle mass for fat, I’m fatigued more often, I have random aches and pains in my muscles and joints that I don’t remember having and, finally, my mind thinks differently. In that last item, I no longer think about sex, I’m slightly more absentminded than I was (I drop things). But, all in all, I’m not overwhelmed.
One thing that is interesting is due to the results of the EMBARK trial, patients appear to be better off in the long run (at least higher risk ones) taking Xtandi during RT instead of "standard" ADT drugs we've been discussing here. It had better long-term outcomes. But combining Xtandi with ADT drugs was even better. That's what led the FAA to recently approve Xtandi for use with high-risk patients with non-metastatic hormone sensitive PCa. But that's really a whole other subject.
Content on HealthUnlocked does not replace the relationship between you and doctors or other healthcare professionals nor the advice you receive from them.
Never delay seeking advice or dialling emergency services because of something that you have read on HealthUnlocked.