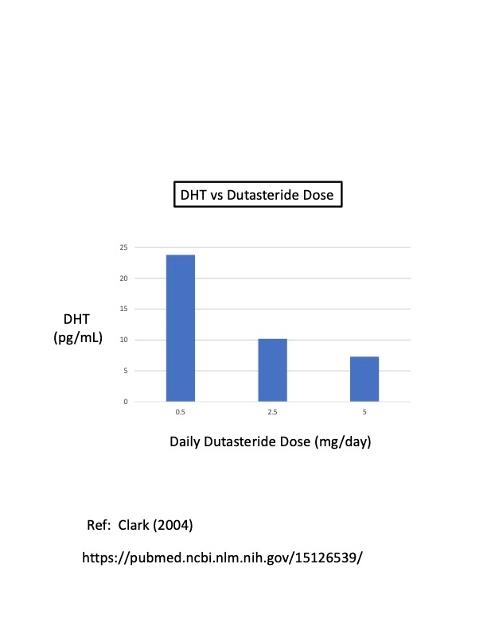
The plot above shows the residual (nadir) level of DHT in men as a function of the daily Dutasteride dose (mg/day). The DHT nadir numbers shown in this plot are:
23.8 pg/mL for 0.5 mg daily dose;
10.2 pg/mL for 2.5 mg daily dose; and
7.3 pg/mL for 5 mg daily dose.
Ref: Clark (2004) [see Table 1 from Clark 2004]
pubmed.ncbi.nlm.nih.gov/151...
The normal concentration of DHT in a healthy man without prostate cancer is about 400 pg/mL. Taking 0.5 mg/day of Dutasteride reduces the normal DHT level by 94.7 % to about 24 pg/mL (reduction factor = 19X). Increasing the Dutasteride dose to 2.5 mg/day reduces the normal DHT level by 97.7% to about 10 pg/mL (reduction factor = 40X). Finally, increasing the Dutasteride dose to 5 mg/day reduces the normal DHT level by 98.4% to about 7 pg/mL (reduction factor = 57X).
Since DHT is the actual molecule that "feeds" prostate cancer growth (not testosterone), it follows that reducing DHT as low as possible is as important as reducing testosterone as low as possible when doing chemical castration (ADT).
Note: the normal ratio of DHT to Testosterone (DHT:T) in a man ranges from about 1:7 to 1:15, with an average of about 1:10. So, on average, about 10% of testosterone is normally converted to DHT in a healthy man who is not taking Dutasteride.
For example, assuming that the DHT:T ratio stays constant in a man not taking Dutasteride, a 50% drop in testosterone level would cause a 50% drop in DHT level. More relevant to ADT, a 95% drop in testosterone (e.g., from 600 to 30 ng/dL) would naturally cause a corresponding 95% drop in DHT (e.g., from 400 to 20 pg/mL).
DHT is made by converting testosterone to DHT with a “5-alpha reductase” enzyme. Dutasteride effectively blocks the activity of 5-alpha reductase. That’s why it’s called a 5-alpha reductase inhibitor. Finesteride also does the same thing, but not as efficiently as Dutasteride. Both drugs also help to decrease hair loss (since hair growth is controlled by DHT levels).
Taking 0.5 mg daily of Dutasteride does two things at the same time:
(1) it increases T levels by about 20%, and
(2) it decreases DHT levels by about 94%.
That means the DHT:T ratio is drastically changed, from the normal ratio of about 1:10 to about 1:250 when taking 0.5 mg/day of Dutasteride. The ratio of DHT:T increases to about 1:600 when taking 2.5 mg/day, and to about 1:800 when taking 5 mg/day of Dutasteride.
The standard daily dose of Dutasteride is 0.5 mg, which gives a DHT nadir = 23.8 pg/mL. However, the plot above shows that increasing this daily dose to 2.5 mg/day decreases the nadir DHT level by about 57% (from 23.8 to 10.2 pg/mL). Furthermore, increasing the Dutasteride dose to the maximum daily dose of 5 mg/day decreases the nadir DHT level by about 70% (from 23.8 to 7.3 pg/mL). Those are significant reductions. Interestingly, Dr. Clark reported that the side effects are not significantly changed when increasing the daily dose from 0.5 to 5 mg/day. (See Table 2 from Clark 2004)
An important question is:
Does increasing the Dutasteride dose from 0.5 mg/day to 2.5-5 mg/day cause any improved PCa survival outcomes?
I think the answer is "YES", based on what we already know about how much survival outcomes improve when the (sub-castrate) levels of testosterone are decreased from 50 to 20 to 10 ng/dL (or even lower). (See previous posts)
We know that very small, incremental reduction in testosterone (in absolute terms from 50 to 10 ng/dL), greatly improves survival outcomes. In other words, going from 50 ng/dL to 10 ng/dL is equivalent to reducing a normal level of testosterone (say, 600 ng/dL) by 92% for a nadir = 50 ng/dL, compared to a reduction of 98% for a nadir = 10 ng/dL. That’s not a big difference between the two levels in absolute terms (92% vs 98%).
The reason this is important, for example, is that a 50% decrease in testosterone (in the linear regime below 250 ng/dL) causes a 50% decrease in prostate cancer growth rate (according to traditional ADT theory). Assuming the DHT:T ratio stays constant, then a corresponding 50% decrease in DHT will also cause the same 50% decrease in prostate cancer growth rate.
In a simple linear model, a 50% decrease in a prostate cancer growth rate translates to a doubling of the time to PSA failure. This is true whether you are decreasing a testosterone level by 50% (from 20 to 10 ng/dL), or whether you are decreasing DHT by 50 % (from 20 to 10 pg/mL) by increasing the daily dose from 0.5 mg/day to 2.5 mg/day (according to the plot above).
The first takeaway is that increasing the Dutasteride (monotherapy) dose from 0.5 to 2.5 mg/day could potentially double the survival time, and further increasing the daily dose to 5 mg/day could potential triple the survival time.
Perhaps some one will do a clinical trial to investigate this hypothesis.
COMBINATION THERAPY: Dutasteride + ADT
Another interesting question is what would happen if you combined traditional ADT with Dutasteride?
I think the combo would be fantastic!
The main goal should be to reduce DHT as low as possible. Here's a possible recipe:
STEP 1: Use Lupron (and/or Estrogen) to do ADT. This reduces the testosterone by about 95% (from about 600 to about 30 ng/dL), equal to a reduction factor of 20 X. When you do this, you will concurrently reduce the DHT by the same amount, 95% (from about 400 to 20 pg/mL), assuming the ratio of DHT:T remains constant (without taking Dutasteride at this point).
[Note: 10 pg/mL = 1 ng/dL].
STEP 2: Add Dutasteride to ADT. We know that using the standard dose of 0.5 mg/day of Dutasteride reduces DHT by 94% (reduction factor = 16.7 X). I believe that this 94% reduction will synergistically magnify the % reduction from doing Lupron ADT.
So, to estimate the potential total % reduction in DHT from the combined treatments you multiply (1-0.95) x (1-0.94) = (0.05) x (0.06) = 0.003. The total % reduction in DHT is predicted to equal (1-0.003) x 100 = 99.7%. Hence, a 99.7% reduction of the normal DHT level (400 pg/mL) equals 1.2 pg/mL, which is an extremely low value of DHT. Such a very low DHT of 1.2 pg/mL corresponds to a very low PCa growth rate, according to the linear model of Morgentaler.
A simpler calculation is to multiply the ADT reduction factor (20 X) by the Dutasteride reduction factor (16.7 X), to get a Combo reduction factor = 333 X. Then, you divide the normal DHT value of 400 pg/mL by 333 to get a reduced DHT value of 1.2 pg/mL (which is the exact same number as above).
The takeaway from doing Dutasteride + ADT COMBO therapy is the huge potential for increasing the time to PSA failure. Assuming that the prostate growth rate is linearly proportional to DHT, then the time to PSA failure is increased by the ratio of (1-0.95) / [(1-0.95) x (1-0.94)] = 0.05 / [(0.05) x (0.06)] = 0.05 / 0.003 = 16.7. This implies that the time to PSA failure could be increased by more than a factor of 16 X. That's a huge (theoretical) gain!!
Again, I wish we had real data to support this hypothesis...
A University could easily do a simple, randomized clinical trial that adds Dutasteride (or placebo) to Standard of Care Lupron ADT. It would be ethical, and it could have two options for a Dutasteride daily dose: standard 0.5 mg/day and high-dose 5 mg/day.
