Ugh...I made a BIG mistake on the previous posting!
I just realized that Dr. Morgentaler had listed the Testosterone level in unusual units (ng/mL), not the usual units of (ng/dL). So, my X-axis was off by a factor of 10.
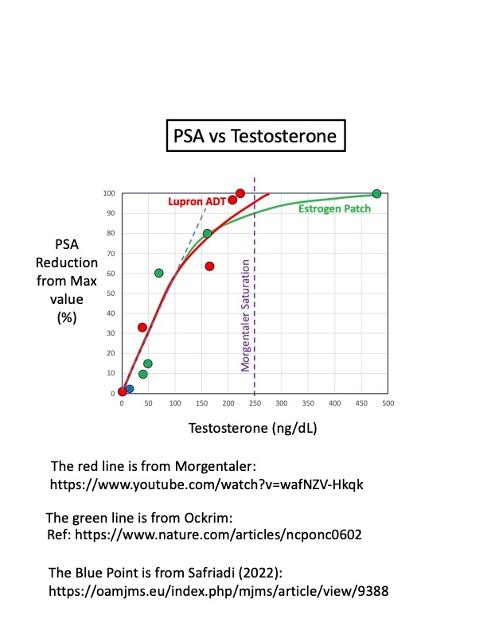
Here is the revised plot. The exciting discovery is that the two different (and wildly different) datasets converge to essentially the same curve !!
The Lupron points (red) and the Estrogen Patch points (Green) seem to have the same behavior. This makes sense, because they have the same mechanism of action (suppression of LH and FSH causing suppression of testosterone).
I also added the published Morgan Saturation Model rollover point (T = 250 ng/dL). It appears that the roll-over in this dataset occurs earlier, i.e. at about 150 ng/dL...not 250 ng/dL. More data is needed to more accurately confirm this rollover point. The linear regime ranges from T = 0 to 150 ng/dL. This linear regime is the basis for why ADT works so well for castrate-sensitive Prostate Cancer patients.
Written by
janebob99
To view profiles and participate in discussions please or .
I'll have to research the time to PSA failure, comparing estrogen to Lupron ADT. In principle, they should be the same because both have the same mechanism of action (LH, FSH suppression).
Here's a comparison chart showing the pros vs cons of transdermal estrogen (TDE) therapy.
i’m glad you made that correction I was just about to jump in when I saw that linear plot. Check out my postings on this issue. What Dr Morgentaler has always tried to State is that it’s not necessary to drive testosterone to zero in treating prostate cancer. This was the fundamental point he is trying to make. And driving testosterone to zero has dramatic negative lifelong impacts on men’s quality of life and sexual function. If you could keep testosterone at around 200 to 250 heck that’s what men in their 60s and 70s have naturally anyway. It would make a huge difference to quality life.
I’m gonna go on memory here but read much of my postings. The other shocking thing that the doctor points out is that the whole canard testosterone is like, adding gasoline to a fire is based on two or three men. in the end, if memory serves correct, it’s based on the observations of one man for two weeks. Men in the United States, and all over the world have had their testosterone wiped out because of research that is based on one person.
Point that more data is needed is a interesting point. But we will never get this data. The research will never be done, and nothing will ever happen to the current standard of care and protocol. I can’t remember the doctor that said it, but it goes something like this; it takes 50 years to get a bad idea out of medicine and 100 years to get a good one introduced. so don’t hold your breath. Testosterone will be continued to be driven to zero when there’s probably no need to do it
I’m going on memory but check out my postings on this. I researched this issue ad nausea. Sorry for the long post.
Thanks for your interesting post, and for your research on this topic. I will try to find your previous posts.
I'm a big fan of Morgentaler's work. But, I may disagree on the fine points of his saturation model. He says the roll-over point occurs at about 240-250 ng/dL, but my data analysis shows that the curve rolls over at about 150 ng/dL. I'd like to get his email address to send him this plot and get his feedback. Overall, we agree very well.
My understanding of T at this point is that there are three regimes of behavior. For the Pre-Diagnosis regime, it appears that high testosterone is generally protective. Also, for the castrate-resistant PCa regime...higher T (above the saturation point) appears to also be protective there.
But, in the hormone-sensitive regime (non-CRPC), ADT works extremely well at improving survival outcomes. This is the linear regime of the Saturation Model, which predicts increasing rates of PCa growth for increasing levels of T (below the saturation/roll-over level of 250 ng/dL). Getting the T < 10 ng/dL (sub-castrate level) significantly improves survival outcomes. See attached plot.
So, high T is not protective in the middle regime (hormone-sensitive PCa). I'm curious if you have any data that refutes this statement?
Bob
PSA recurrence free survival probability vs time for different T-nadir levels
No, I don’t have data that addresses the saturation model PSA theory but I guess that was my overall conclusion of my research, that no one else does either. This research simply is not done. I may be wrong, but the graphs you are presenting are the result of ‘zero PSA is best’ data collection. And in this condition, while attempting to keep and drive PSA to zero those men who don’t respond to ADT have negative outcomes correlated to higher PSA levels. Again, I may be wrong, but I think that’s what these graph show.
…what has never been done and will never be done is to prove or disprove the saturation model itself. What if men’s TET was kept to even 150? 150 is a heck of a lot better than zero. I went through 21 months of ADT, where my testosterone was three (3)! That really does a number on a man’s body. I am now one year and three months into a vacation and so far so good. My testosterone returned (thankfully ) to the level I had before surgery which was in the low 300s. I can only imagine how much better I would’ve felt during my ADT treatment if I could’ve kept my testosterone in the 150 to 200 range and had the same results. That research has not been done as far as I know.
Again I could be wrong about your chart. But right now the standard of care is to drive testosterone to zero. The lower the better. And the saturation model begs to differ, but has never seen the light of day as far as research is concerned; it never will. Correct me if I’m wrong. TNX Rick
I think it's important to receive feedback with different points of view.
I appreciate how awful it is being on ADT. That's why I've been promoting Estrogen patch/gel therapy as a better alternative to Lupron ADT.
You raise a good point that there are men who don't respond to ADT. It could be that those men have progressed to being castrate-resistant, which is a common occurrence in men with advanced PCa. In that regime, it appears that higher-T is protective.
Have you seen the very recent survival curves from Artera.ai (artera.ai) that show 66% of men don't respond to ADT, while only 34% of men do respond to ADT. That could explain why there is so much scatter in the data. I should get my Artera test results back in a few weeks.
My PCP wants me to have a T>1000 ng/dL. Have you considered doing TRT to bring it up to that level?
You say there is no data supporting the Saturation Model.
I respectfully disagree. I presented results yesterday that show the linear regime and a saturation effect. The plot shows PSA versus testosterone, with a rollover (saturation) point of about T = 150 ng/dL. That is lower than Morgentaler's saturation point of T= 250 ng/dL, but that could be just statistical variations. The two different data sets (Lupron ADT and Estrogen patch) overlay each other very nicely in the linear regime, which gives high confidence in the linear portion of Morgentaler's model. Plus, the curves start to rollover and saturate at T > 150-200 ng/dL. This rollover is consistent with Morgentaler's model. The linear portion supports the statement that lower testosterone is associated with lower PSA values when on ADT (only for hormone-sensitive men).
Hello. Will you please do many of us here a favor please and write this which state in layman's terms. I find this difficult to follow and understand. Will you please take time to do this. I hope you understand what I am asking. I find your postings and ideas fascinating and get some form of idea as to what is being stated but need to understand them. Thank you.
I will try to explain these things better in layman's terms. I hope to post a 1-page "Lessons Learned" about Estrogen therapy soon, with 7 short bullet points.
I'll do the same for the other topics I've posted about.
This is wonderful Bob. I really thank you for your postings and look forward to the new postings you are going to create for us. I hope that the sun shines on you.
…well I’m glad and surprised that there is any data that shows the validity of the saturation model. I did not think that this was common or even desired by the vast majority of urologist and MO’s. But who knows things change. I hope that men going forward can have some testosterone while also suppressing PSA. Even a TET of 150 or 200 is far healthier than testosterone at near zero. You really pay a heavy price.
…no I’m not aware of the Artera or other data that you talked about. If you want to post that we can look at it.
…your primary care physician wants your testosterone at 1000. That’s interesting but do you know what your baseline testosterone was before you had surgery or radiation. That is the question and 80% of men are never tested; doctors don’t care what your testosterone is going into treatment which is baffling. When you are trying to recover how are you supposed to know if you’re back to normal w TET if you don’t know where you started from? Luckily I had a test result for TET that was some two years before it was operated on that showed I was in the low 300s, which is not uncommon for a man in his 60’s, Again there may be some men out there in their 60s and even 70s that have a testosterone of 1000 but I think they are outliers. I don’t know if that’s normal for you if it is great. If I had prostate cancer, I would be leery of pushing my testosterone to those levels. Again, even if the saturation model is accurate, that level of 1000 is well beyond the plateau that we’re talking about after which you do reenergize the growth of prostate cancer.
…the other thing I researched is that for those men that are given the decipher test there is a matrix which decipher publishes along with the test results. That matrix can be used by doctors to identify men who will respond to ADT. This could also save men from affecting their bodies unnecessarily. Look, I took ADT for 21 months and I know it helped me. But in no way was I prepared or informed of what would happen to me. If I had been, I would’ve taken some steps before hand. But ADT does work for some men. But it also does a hell of a job on your body and for men’s sexual health it’s Destructive. But if you need it, you should take it. But you should take it only if you benefit from it. The decipher matrix helps men determine that. I’ve published some of this in my blog site. Rick
Here's the key plot from Artera.ai that shows that 66% of men don't benefit from ADT, versus 34% of men who do benefit from ADT. It could be a game changer. The test is FDA approved, and Medicare pays for it (starting 1/1/2024). So, very recent stuff.
I agree that doctors do a lousy job of telling men about the bad side effects of ADT. That's why I'm pushing so hard on using Transdermal Estrogen (TDE) as an excellent alternative to Lupron ADT.
I haven't gotten the Decipher test yet. Hope to soon.
I'm only recently diagnosed with PCa. Haven't had RT yet, but plan on doing SBRT in a few months. The only treatment I've had is taking Dutasteride and my PSA has dropped a lot: from 10.0 to 3.3 over 3 months. I expect it will continue dropping. What I don't know is if the PSA is dropping because the prostate volume is decreasing (it's supposed to shrink by 20-50%), or because the tumor has stopped growing or is shrinking. Perhaps both are happening at the same time.
I have hypogonadism and have been taking TRT for over 10 years. That's why my T is so high now...I'm supplementing it.
My treatment plan is to continue taking Dutasteride, and then stop doing TRT. I should naturally chemically castrate myself after stopping TRT, since I don't make testosterone anymore. I want to get to T < 10 ng/dL, for maximizing survival outcomes.
I also plan on starting estrogen patch or gel therapy to counteract the bad side effects of the very low testosterone. We're all awaiting the final results of the phase-III PATCH trial comparing estrogen patches to Lupron ADT. It should be published this Fall.
How do these methods compare to the idea of hitting the patient with very high levels of testosterone periodically? I have heard of this recently and think a relative’s doctor is going to have him do this.
You're talking about Bi-Polar Androgen (BAT) treatment. It's being used for men with advanced PCa who are castrate-resistant (meaning that ADT doesn't work anymore and their PSA is rising). The BAT protocol is apparently quite successful, and very inexpensive. You may want to contact Dr. Sam Denmeade at Johns Hopkins, who invented the technique, for more information. hopkinsmedicine.org/profile...
This is one of the better (useful) threads I've read here, thanks for your effort to post and clarify. My personal experience is that total ADT was counter-productive, it immediately raised my PSA, many years ago. I'm finding success at QOL, physical, mental and sexual health with BAT. Mine is a personalized cycle of 6 weeks, supra T 1400+ for one week (t-cyp), maintenance at 250-300 T for 4 weeks (androgel), low T 50 +- for 1 week, 240 mg xtandi at the 35th day. Rinse and repeat. PSA < .006 for over year, after surgical interventions for 4 lymph nodes. 4 weeks is not enough to wash out T-Cyp, so androgel in the middle. If someone can comment on Xtandi 8 day half-life, it reaches into the supra week, in the context of this threat, that would be great. Maybe this should be a different thread, but since there were comments on very low T be problematic in some patients, I thought I would chime in.
Something I couldn't understand from your plot were the Lupron and Estrogen patch data points. Don't these two treatments reduce Testosterone to zero? Why are they plotted against positive values for T?
Great question. You're really thinking about what the plot means.
Take, for example, the green points. That's for a man that started estrogen patches at time = 0, which corresponds to the point at the upper right hand of the graph. So, time = 0 equals the baseline. Since the Y-axis is normalized to the peak (maximum) PSA value, the value of that point is 100% (at time = 0, baseline). Then, as time progresses, from 2 weeks, to 1 month, to 2 months and finally to 3 months, the green points start to march down the green curve towards the original at (0,0) where testosterone and PSA are zero. In other words, each of the green points is at a different time from start of applying the estrogen patch.
I've attached the source data plot showing the drop in testosterone and PSA versus time for the Estrogen man. Note the different time scales (the upper one is in weeks, the lower one is in months).
Eventually, the estrogen man is chemically castrated at a testosterone nadir of 40 ng/dL and a PSA nadir that's only 10% of the original peak value (we don't have the absolute values for this data set). That is the green point at the bottom left hand corner of the plot.
I appreciate that this is a challenging plot to understand.
Bob
T, PSA versus time after starting estrogen patch therapy
Here's the plot of PSA versus testosterone for just the Estrogen patch man. I've labelled the points with the time at which they were measured. The points march from the upper right hand of the plot at time=0 down to the lower left hand of the plot at time = 3 months (with continuous estrogen patch therapy).
Note that I've forced the green curve to go through the origin. But, in this man, the lowest value of testosterone that he achieved was 40 ng/dL. He probably could have applied more patches to get his T-nadir down to a better level of T < 10 ng/dL.
1. If you want to reduce your cancer growth rate and, hence, PSA, to a very low value, then you have to reduce your testosterone levels to very low (sub-castration levels). That's the basis for doing ADT. Ideally, testosterone level should be < 10 ng/dL.
2. Increasing testosterone above 250 ng/dL has no additional impact on increasing cancer growth rates beyond the maximum "saturation" value. This result helps men who want to increase their testosterone after stopping ADT for QoL, namely, by taking supplemental testosterone to get T back to normal levels of 400-700 ng/dL . Doing so will not cause any increase in cancer growth rates above its maximum saturation value. This means that having a high testosterone after ADT treatment is finished is not going to increase your cancer growth rate, compared to a low value 250 ng/dL.
The actionable take away is to have a goal of reducing your testosterone to less than 10 ng/dL to maximize the survival probability, by doing Lupron ADT or high-dose estrogen therapy. This will also reduce your PSA to very low values, between about 0.1 - 0.5 ng/ml.
I do not mean to deem your efforts in doing this research and trying to understand the impact of your analysis but for the most part most of us live in a different world.
Let me explain what I mean in simple terms. Aeronautical engineers are amazing at discussing the scientific data on why airplanes fly, the impact of changes to aircraft modifications and future trends.
However that is useless to a pilot in a close in dog fight. They have sometimes split seconds to plan an attack, gain an advantage and kill the other guy. Assuming we are not allowed to launch missiles beyond visual range which is a political decision. Do not even want to go there.
Most of us cancer pilots in this fight receive 15 minutes to receive the results of a test or procedure and plan the next phase. Most of us are searching for concrete steps that our doctors are willing to support based on current standards of care.
I agree that the better informed we are on the standards of care available the better off that 15 minutes goes and the more comfortable we are with our future therapy. Not all of our doctors are on the cutting edge of cancer research and theory.
Sometimes I am reminded of my Philosophy class discussions on how many angels can fit on the head of a pin. Yes I was educated by the Jesuits but am a true pragmatist. I live in the world of what works.
We need forward looking thinkers and researchers but sometimes we simply like that fighter pilot do not have the time for potential what ifs. Nor do our doctors.
Sorry if this seems harsh but for many it is our reality. We do the best we can with the brain power available to us and education.
Sorry for this long post and any hurt feelings it has caused.
I've gotten similar feedback recently, including from Prof. Wassersug.
I'm just about done making plots that are difficult to understand. I show all the plots to my RN wife to see how well she understands them. Most are easy to understand, but some are quite difficult. So, that's useful feedback to me.
I do have ideas of posting series of simple, 1-page "Lessons Learned" docs, that will cover a wide range of topics. Stay Tuned!
Content on HealthUnlocked does not replace the relationship between you and doctors or other healthcare professionals nor the advice you receive from them.
Never delay seeking advice or dialling emergency services because of something that you have read on HealthUnlocked.