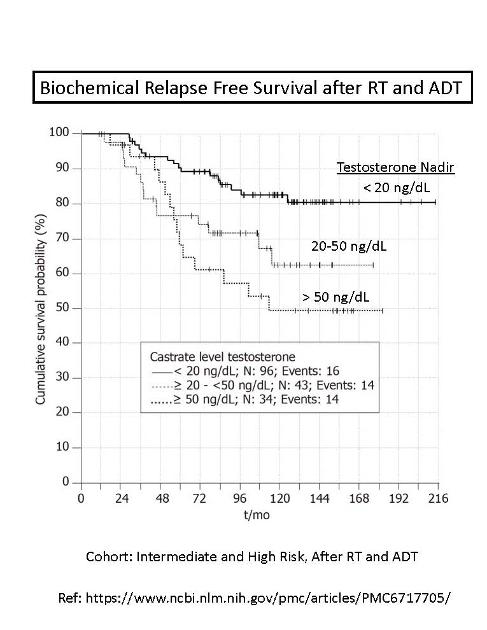
This plot shows the Biochemical Relapse Free Survival after RT and ADT, versus time for up to 18 years, for Intermediate and High Risk men, comparing different levels of testosterone nadir ( 50 nd/dL). (ref: 2019)
The bestoutcomes are significantly associated with a lower testosterone nadir ( < 20 ng/dL).
This may be well-known to many of you, but it was new to me.
The prior definition of castration being < 50 ng/dL probably needs to redefined to < 20 ng/dL. (I read that the level of 50 ng/dL may be an artifact representing the lowest limit that testosterone could be acurately measured many years ago. That makes sense to me).
Since it is well known of course that testosterone feeds PC, and ADT is designed to reduce testosterone to castration levels, all of your many posts showing that lower testosterone is better makes sense. However, all of your posts on this topic show studies and results before or without the use of second generation anti androgens, which have been shown multiple times to extend time to CR and OS.
Again, logically, by design, these anti androgens should be a bit of an equalizer for remaining low levels of testerone.
Above is a chart of time to castration resistance from ARASENS - >60% of the population achieving 4 years before CR.
Thanks for the plot. I agree with your assessment.
I've not researched the 2nd generation anti-androgens. Your plot shows a huge effect of adding darolutamide to the mix. I've heard good things about darolutamide from Dr. Metzger (Ret.).
I vaguely remember reading a post where Abiraterone reduced testosterone down to 1 ng/dL. Anything that reduces testosterone to the sub-castrate level (< 50 ng/dL) has been shown to greatly improve survival probabilities, in a linear fashion.
Content on HealthUnlocked does not replace the relationship between you and doctors or other healthcare professionals nor the advice you receive from them.
Never delay seeking advice or dialling emergency services because of something that you have read on HealthUnlocked.