I've been feeling increasingly week during the last past months. Jelly legs, crying for no reason (not depressed though). I just want to lie down. Legs feel like lead, physically exhausted after minor exercise (short walk). Dizzy spells. Nauseated sometimes. Blurred vision.
I thought maybe my iron was low again, but no.
Because drs keep telling me I'm on too much T3, I lowered my Cytomel with 1/8 (!) of a tablet, going from 62.5 mcg to 59.375 mcg. I took this from my 6.30 PM dose. I also did this because I was very jittery, my hands were trembling and my heart was skipping a lot of beats with high pulse; The latter is quite usual for me, but not over 90 all of the time.
Lowering the Cytomel somewhat helped with the jittery feeling, but I am still trembling. Pulse still high-ish but better, less skipped heart beats.
My blood work showes a sligltly highter FT3 level then the previous time on LESS Cytomel , how is this possible?
BP is all over the place. Sometimes I have like 10/7, then it can be 14/9. T° is higher than usual, around 36 - 36.5°C at night which is rather high for me.
Chronic UTI has been playing up badly which could explain the BP and the t° I guess.
Just as reminder: I have untreated adrenal insufficiency as well.
I'll try posting my latest blood works. Folate isn't included: the dr forgot and then it was too late to add. But it alwasy has been fine so there's no reason to presume it suddenly wouldn't be.
Thanks in advance!
Written by
Soloslim
To view profiles and participate in discussions please or .
I am suffering much the same as you Soloslim , and know my Cortisol is low, so suspect your symptoms are also low Cortisol. Sorry, but don't know as yet how to rectify this without taking Hydrocortisone. This means seeing a GP, if not an Endocrinologist. Wish you good luck with it.
Didn’t mean to confuse, for ferritin, we usually aim for 100. But that target is for the many of us who start out deficient. So to many of us 156 is on the high side, but it’s not dangerously high - and at your age the target range does increase.
Here’s probably more info than you wanted, but helpful in understanding the nuance of ferritin ranges (thanks to Jazz80 ) :
The lower limits of 30 are by the NICE threshold of <30 for iron deficiency. Our review of Medichecks data has determined the upper limits. This retrospective study used a large dataset of blood test results from 25,425 healthy participants aged 18 to 97 over seven years. This is the most extensive study on ferritin reference ranges, and we hope to achieve journal publication so that these ranges can be applied more widely.
Lastly re your iron. Although I do agree that there is nothing extreme in your iron that I’d immediately blame here.
But here’s a more nuanced look.
Although your ferritin is great (what’s the trend been?) when you said you were worried if it was iron again - when was your iron low and how did you treat it.
There are several measures that give me pause. I’m wondering if they are in their way up, or down, from a trends perspective.
Your transferrin saturation at 31% is at the bottom of where we want to see it. So not bad, but should ideally be 35-40%
Your hgb and hct - true trailing indicators of iron are on the low side annd not in anlignment with your high ferritin. So again wondering what the trends have been.
Lastly a snap opinion would be your b12 issues are impacting your iron.
Low b12 and folate impair red blood cell production - so that could explain your low hgb and hct regardless of iron.
Do you know your last mcv? That’s one of those measures that can help identify if low red blood cells is due to iron vs b. Since yours MCV is higher in range that points to the impact of b12 deficiency .
So without more info or trends, your iron profile is mixed, but I’d go with b12 becasue of your high ferritin and normal mcv.
Any trends would be helpful.
Net net - your symptoms are a little outsized for the ferritin and cbc you have. But if you just recovered from low iron ( did you recently have an infusion by any chance) maybe symptoms are lagging.
You obviously have sufficient b12… I have no experience with whether that’s too high or not.
And so I bet it’s more to do with your adrenal insufficiency.
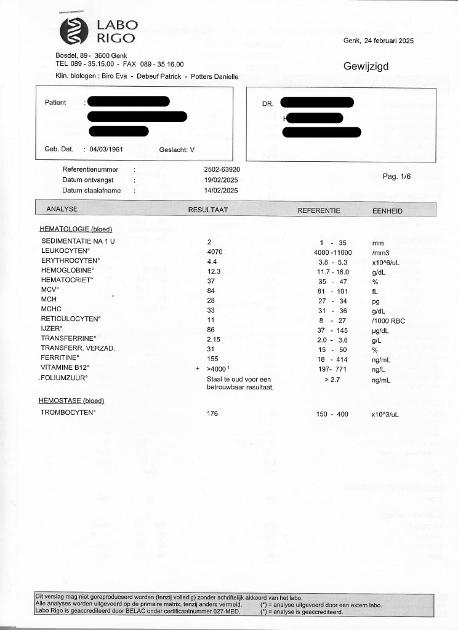
December 2024 (after a couple months of lactoferrin, because my iron was very low the previous time and I cannot tolerate iron supplements in any form)
Iron 92 (37-142)
Transferrin 2.35 (2-3.6)
Transferrin sat. 31 (15-50)
Ferritin 140 (18-414)
August 2024:
Iron 27
Transferrin 2.25
Transferrin sat. 10
Ferritin 170
Folate 10.6 (3.9-26.8)
CRP 7.3 (<5)
Hemoglobin 12.9 (11.7-16)
Hematocrite 38 (35-47)
MCV 84 (81-101)
November 2023:
Iron 83
Transferrin 2.22
Transferrin sat.29
Ferritin 177
CRP 1.9
Hemoglobin 12.4
Hematocrite 38
MCV 85
June 2023
Iron 99
Transferrin 2.2
Transferrin sat. 32
Ferritin 174
MCV 84
Is this helpful at all?
In the past I've had very low iron and have had injections, resulting in ferritin going through the roof and needing bloodlets.
I have been getting B12 shots for years now, cannot function without them. Drs tell me not to worry about it being too high since presumable you pee out the excess B12, it doesn't accumulate.
Between Aug and Dec ‘24 - the only change was some lactoferrin?
If so, your transferrin saturation responded great! 10 to 30.
Nonetheless - It’s hard to interpret when you’re getting both iron and b12 injected but don’t say when. Question - do you have a steady dosing schedule, including whatever injections you get, where you only change one thing at a time so you can isolate it’s impact?
I still GUESS (not sure) that it’s not your iron or b12. With the exception of your one over range CRP, other ferritins would be representative of actual ferritin - which clearly is sufficient . And your b12 is obviously sufficient.
How can you chase down the impact if your adrenals?
Maybe your answer is in your own post - you have untreated adrenal insufficiency. I know nothing about that though.
Are you sure you have adrenal insufficiency? Your cortisol is low but looks more like adrenal fatigue to me. Surely if it was insufficiency doctors would be treating it, no?
Anyway, what can you do about low cortsiol? Good question. Could be they just need a little TLC:
- plenty of salt - have you tried the adrenal cocktail?
- plenty of rest: always go to bed and get up at the same time so that you body slips into an easy rythm.
- have a high protein breakfast as soon as you get up - eggs and cheese and stuff.
- and, of course - easier said than done! - avoid stress as much as possible.
As to your T3, when on T3 mono-therapy, the way you feel is more important than blood test numbers. So, if you feel that you are over-replaced, try reducing it again - just a little. However, if it were me, I wouldn't change anything until my adrenals were a little happier.
And, of course, it does depend why you are on T3 mono-therapy. Is it because you're a poor converter, Can't tolerate T4? Or do you have some degree of resistance to thyroid hormone? If the later then splitting your dose isn't going to help. You would need to take it all in one go at some point in the day. I take mine early morning, when I get up for the loo (IF I get up for the loo. lol) But I have tried taking it at other times and didn't notice any difference. So, whenever is most convenient, I would say.
I've had an ITT (failed) and 2 more recent ACTH-tests (1 failed, 1 just passed), so yes, quite clear AI. Confirmed by several endos.
Cannot take steroids, have tried that for a couple of years. Felt like a hungover zombie all of the time, tried HC, pred, etc., in cremes, pills, e.c. pills, anally (yes!), just not possible. Esophagus ruined, cannot tolerate PPI's and c°. So I don't want to go there anymore. Ever. Endo wouldn't go for injections or pump, so no treatment whatsover.
I am not good at all in feeling what my body needs or doesn't need, having ignored it and pushed through with wrong treatments for so long. ANd my symptoms are not exactly distinct, I'm a bit all over the place, so I have to go by trial and error. I'm on the spectrum so not very good in interpreting symtoms.
I cannot tolerate anything with t4 in it. Not so long ago my endo insisted I added 25mcg of T4 just and after a day or 2 I started crashing badly. After 2 weeks I didn't know I was alive anymore and it just got worse and worse. After 2 1/2 months I stopped because I couldn't do this at home anymore. I just sat there and lost lots of time. Endo fired me, said I was not open to options. A couple of days after stopping the T4 the fog cleared. Have tried Armour and Erfa in the past, same thing.
How do you know if you have thyroid resistance? Is there a test for that?
I know about mono dosing but since I'm in such a weak state I'm afraid to try it. I'm ridiculously oversensitve to any change, even minimal. Scared to end up in the hospital with an adrenal crisis which would be a dangerous thing since I'm not steroids, hence they wouldn't accept that it's the adrenals, I have no treating endo and T3 isn't available where I live so they would either stop the thyroid meds or give me T4. And I've been really struggling with my UTI lately so that's not the best time to make major changes either. I'ts not that I'm not open to options LOL
OK, so you can't tolerate T4, I get that, I'm the same. I have tried myself to gently introduce T4 with my T3 and it never works. So, I've stopped trying. But you don't have to take it. You can manage without it - a lot of us do. So, let's forget about T4 completely and stick with T3.
Unfortunately, no, there is no test for resistance to thyroid hormone. There are just the normal tests but you have to know how to interpret them compared to how you feel. You may not be 100% in tune with your body at the moment but you do know when you don't feel well - otherwise, you wouldn't be here, would you.
So, you get your FT4, FT3, TSH tested and look at the results: your FT4 and TSH are very low - of course they are, that's to be expected. But your FT3 is at the top of the range yet you still feel bad.
You've tried reducing it, in case you were over-medicated, but that didn't help. So, the conclusion is that you need more, not less, right? Because it's there in the blood but not getting into the cells because your receptors are resisting it.
So, you need to flood those receptors, bombard them with T3, so that some of it at least is forced into the cells.
The problem with doctors is that they're all hung up on ranges - because they don't know what ranges are - and they freak out if something goes over-range. But that's not always a bad thing. Some people just need their FT3 over-range. And that's OK because T3 in the blood is inactive, it doesn't do anything. It only becomes active if it goes into the cells.
So, as I said, you have to flood the receptors to force at least some of that T3 where it's needed. And you can't do that by splitting your dose because that's just not enough T3 in one go. You need to take a large dose all in one go.
Now, I can understand that that idea is intimidating. But there was time when I was taking 225 mcg in one go, just before bed, and I didn't feel a thing. Slept like a long. It didn't do me any harm.
I would never suggest that anyone else take that much T3! But at that time, it was what I needed to wake up my receptors. And it worked! I don't need half that much now.
So, you're taking a much smaller dose, and that may be all you need. But, if you have resistance to thyroid hormone, you need that all in one go, not spread out through the day.
Don't make big changes if you're sensitive to them, just tiny, tiny ones. Just slowly take less throughout the day and more for, say, your first dose of the day. Just 2.5 mcg at a time removed from your second dose to your first - maybe one day a week to begin with. Then on two days. And when your taking that extra 2.5 more for your first dose - and less for your second dose - every day, then slowly start with another 2.5. And gradually move all of it to your first dose of the day, and see what happens.
If you find that taking it all in one go doesn't help. Fine. At least you tried, and you can just go back to what you were doing before. But, it could change everything for the better.
As to your adrenals, I'm no expert - not even a doctor - but going by my personal experience, and all I've read on here of other people's experiences, I don't even think you need HC. I took it for a couple of years because my cortisol was much lower than yours, but I was diagnosed with Adrenal Fatigue, not Adrenal insufficiency.
Adrenals can recover if you're kind to them. Did you open that link I sent? Did you look at the chart? Nutrition is even more important for adrenals than for thyroids. And it can't hurt to try and give them all they need. There's nothing alarming or controversial in that list. Give it a go and see if it helps. Never mind all these ACTH tests and the rest, doctors don't even know how to interpret the results! Just assume that your adrenals can do better and give them all they need.
Well, I don't know. The function dr I saw years ago when I was on steroids said I would never be able to wean myself off them, that I crash. And I do meet al the requirements for AI, every endo I saw (quite a few!) said the same.
My cortisol level seems more or less OK, but when something happens I can't cope. That something being someone rude to me or driving when there's a lot of traffic, really minor things. Then the shakes arrive. Having a pleasant family meeting (when I'm able to do) in the afternoon will result in several sleepless nights and feeling nauseated. Even too loud music or a sirene going by can cause this. Stimuli are a big no!
I hear you about nutrition. Unfortunately I have an absorption problem a, so according to the drs I'm quite undernourished despite a very very healhy diet. Too skinny as well but maybe that's because of my adrenals.
Take supplements is a hardship. Functional drs have prescribed me numerous supplements because I was always lacking everything, but I have huge problem tolerating even the silliest supplements, in whatever form. It really is ridiculous. Something about methylation and not being able to detox. If it has to go through the liver it's a no.
I'm sorry but why are you talking about AI in respect to Adrenals? Do you mean Addison's? According to the cortisol result you gave, yours is not low enough to be Addison's.
By 'absorption problem', do you mean low stomach acid - which most hypos have? Or something in the gut?
Can you not even tolerate sprays or oils on the skin?
Well, it does matter, but they haven't a clue about that!
I don't see why applying HRT twice a day stops you using other oils. You have plenty of skin area to apply them to. You wouldn't do it all in the same spot.
The HRT goes on my arms, belly, legs, chest , behind. I have to rotate because I have very sensitive skin (of course I have) and I get burning if I apply it too long on the same spot. Have to apply special ointments on chest area because of burning (of unknown origin, it's not allergies). Feet and legs get treated twice daily because of burning. You see why I'm not a big fan of applying more things...
Oh, about weaning off HC. It can be done if you only take it before 1 pm. If you take it throughout the day, to imitate the natural pattern of cortisol production, the adrenals will shut down. And once they have shut down, they will never function again, so you can't wean off them.
But, if you only take it in the morning, and leave the adrenals to cope by themselves for the rest of the day, when the need for cortisol is less demanding, it give them time to rest and recuperate and become stronger. Then, when you wean off the HC, they will slowly take up normal production again. I was able to wean myself off it after about two years.
I don't know but wouldn't it make more sense to add the 2.5 mcg (don't really know how I would do that, that's 1/10 of a tablet!) from my evening dose to my morning dose instead from my mid day dose to my morning dose? If I would do as you suggest it would leave me with a larger dose in the morning, then nothing all day until 6.30 PM for what used to me my 3rd dose. Does that seem right to you, just to be clear?
Not sure it would make any difference. But you'd have to work out your own best way of doing it, anyway. That was just a suggestion to explain what I was talking about. Besides, if resistance to thyroid hormone is your problem, none of those doses are doing much good anyway because they're too small, and that's the whole point of trying build it all up into one large dose. But, it's all trial and error, anyway.
I lowered my Cytomel with 1/8 (!) of a tablet, going from 62.5 mcg to 59.375 mcg. I took this from my 6.30 PM dose. I also did this because I was very jittery, my hands were trembling and my heart was skipping a lot of beats with high pulse; The latter is quite usual for me, but not over 90 all of the time.
Lowering the Cytomel somewhat helped with the jittery feeling, but I am still trembling. Pulse still high-ish but better, less skipped heart beats.
My blood work showes a sligltly highter FT3 level then the previous time on LESS Cytomel , how is this possible?
Based on the above (and ? maybe the raised temperature ) , i think it makes sense to try lowering yourT3 dose a little more to see what the effect is .....you have symptoms that could be the result of 'too much thyroid hormone' and those symptoms improved a little on lower dose, so personally i'd follow that trend , and see if they improve further .
No long term treatment, no. The occasional Monuril or short treatments when something useful shows up in my urine sample, but otherwise no. Just Hiprex (1/2 tablet daily).
With regards to the frequent/chronic UTI, have you considered asking the GP for a vaginal oestrogen creme?
Vaginal oestrogen can be an effective treatment for frequent urinary tract infections, particularly in postmenopausal women experiencing low oestrogen levels due to menopause. It can significantly reduce the risk of recurrent UTIs by restoring the health of the vaginal tissue and decreasing inflammation in the urinary tract. The gel you apply on your body might not be sufficient in significantly raising the levels in the vagina, so this might be worth exploring?
Content on HealthUnlocked does not replace the relationship between you and doctors or other healthcare professionals nor the advice you receive from them.
Never delay seeking advice or dialling emergency services because of something that you have read on HealthUnlocked.

")
")