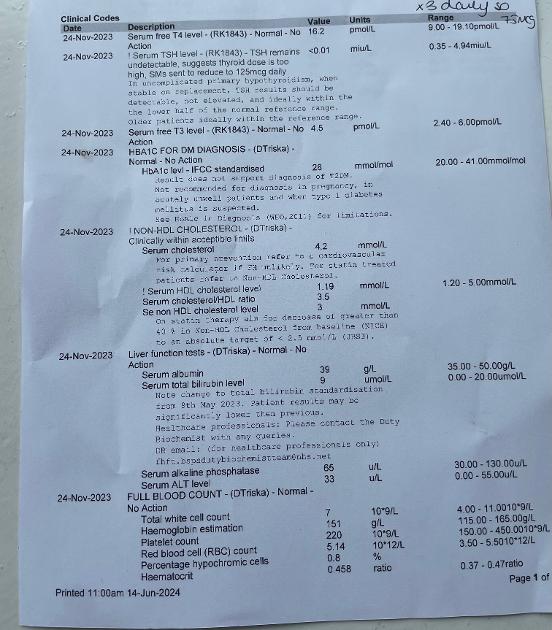
Bloods above - is anyone able to help me with a response to this letter please? I have asked for my levo to be put back up to 150 and they have refused - I have previously posted that I regularly don’t get meds I can take, brands are changed regularly - they often give me meds I have reactions to so I never get a full dose, they have reduced my meds because of my TSH reading - I take T3 and T4.
Thank you
Dear …………
Thank you for your email of 17 June regarding the ongoing discussion about the management of your thyroid conditions. We are very sorry to hear of your concerns you raise.
Please accept our apologies for the delay in responding to you. We felt ti was important to take the time to review your care with clinical input from myself and to set out the practice position clearly for you.
We are sorry that we have not been able to reach a shared plan for your thyroid management. We can see from your clinical record that both Dr ….. and Dr …… have been involved in discussion with you and shared the NICE guidelines for the assessment and management of Thyroid disease.
Clinically we believe the evidence concludes that TSH is an appropriate measuring tool for those with hypothyroidism caused by Hashimoto's and that TSH is indeed helpful in those on Levothyroxine.
In terms of the best approach to monitoring someone on thyroid treatment we would agree with the NICE guidelines that this is not T3 and T4. This simply reflects a snapshot of the day's level and not the longer term measure that is provided by the monitoring of TSH.
TSH is helpful as ti tells us how much thyroid hormone the body thinks it is getting. tI is important to note that the brain cannot distinguish between the hormone produced by the body's thyroid gland and that provided by the thyroxine replacement tablets. If the TSH is high this means that the brain is trying to stimulate the thyroid gland to work harder which is a response to low levels. The reverse situation is also true, where the TSH level is undetectably low this shows that the brain has recognised that there is an over supply of thyroid hormone and is therefore trying to switch off production.
As Dr ……. explained ni his message to you on 1th June, having too much thyroid hormone ni the system over the long term increases the risk of bone thinning and heart failure. It is for this reason that we are unwilling to prescribe a dose of thyroxine which lowers your TSH down into the undetectable range as this is not safe longer term.
Of course, we do appreciate and agree with you that symptom control is an important measure of whether you have sufficient thyroid hormone. Hence, we do not have a set TSH target, most patients feel at their best when their TSH is running ni the bottom half of the normal range.
Ihope that from this review and explanation you will understand why we are unable to increase your thyroid dose at the moment. fI you have not been able to source the preferred brands of levothyroxine then we would suggest that following a period of 6 weeks of consistently taking the medication we then repeat your blood tests and review the results with you.
We do understand that our position is not fully in accordance with your request, however we hope that by laying out the clinical rationale and the potential risks involved will reassure you that we have your best interests in mind in deciding on clinical treatments. fI you would like a further opinion on this then we would be happy to refer you to a thyroid specialist for further discussion and advice.
Iwould like to thank you for taking the time to raise your concerns with us and give us the opportunity to review your care and explain our treatment approach.
We hope that you are satisfied with our response. However fi you remain dissatisfied you have the right to raise your complaint with the Parliamentary and NHS Ombudsman. Further information about how to contact them can be found on their web site at ombudsman.org.uk/
Yours sincerely
