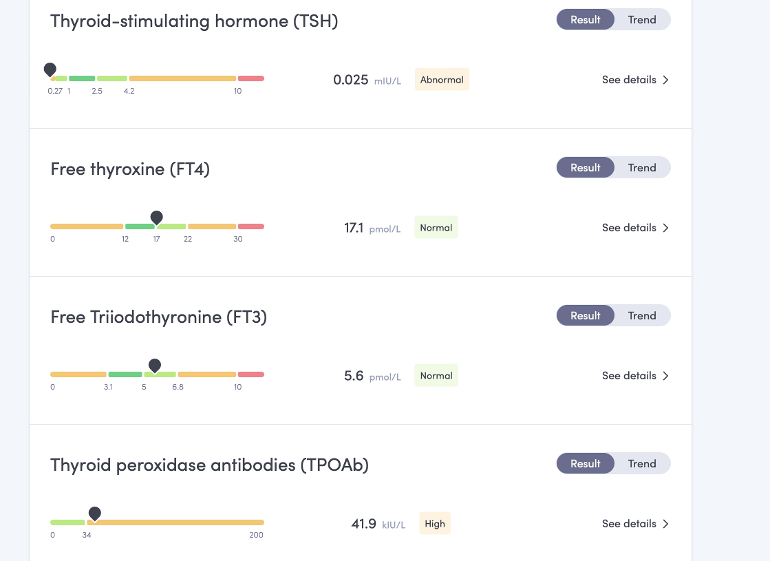
Hi, these are my recent results taken exactly 3 hours after I had taken my thyroid meds. (Normally, I wouldn't take my thyroid meds the morning of a thyroid function test, but my functional health doctor wanted to see whether I was overmedicating, worries about bone health....) I take 75mcg Levo and 2 x 5mcg T3 tablets daily. As you can see, my T4 and T3 are optimal - bang in the middle there - bless 'em!). But, my TSH is, as ever, suppressed. No surprise there - has been like this for several years now. I think my current regime suits me well, I feel better than I have felt for a long time. In the meantime, one of GPs in the practice who I don't normally see has sent me a text saying that before they will issue my next prescription they would like me to go in and "review" my medication. (I am VERY fortunate to get the T3 on the NHS - and I shouldn't have to say that!) For reference, I have the DIO2 polymorphism (homozygous) and on the strength of this was issued T3 by my GP (not an endo) before the review in 2017 that stated only an endo could prescribe T3.
Can anyone recommend any academic papers please that would help me support my case - i.e., T3 and T4 show I am not overmedicated, TSH less relevant? I know we all have our own personal set point. Personally, I know that when my TSH was only 2.87 I felt like death. I really don't want them to start trying to normalise that TSH. The last time it was "normal", I felt anything but, struggling along on only 50 mcg of levo and no T3 medication.
Many thanks in anticipation.
Written by
MacG
To view profiles and participate in discussions please or .
There is some concern that administering thyroxine in a dose which suppresses serum TSH may provoke significant cardiovascular problems, including abnormal ventricular diastolic relaxation, a reduced exercise capacity, an increase in mean basal heart rate, and atrial premature contractions.12 Apart from an increase in left ventricular mass index within the normal range, these observations have not been verified.13 Moreover, there is no evidence, despite the findings of the Framingham study, that a suppressed serum TSH concentration in a patient taking thyroxine in whom serum T3 is unequivocally normal is a risk factor for atrial fibrillation.
Research showing Levo and T3 combo superior for heart
the best paper on this that I have seen indicates that a TSH of 0.03-0.5 is best on therapy. Above that is insufficient and below MAY or MAY NOT indicate slight overdosing
Interestingly, patients with a serum TSH below the reference range, but not suppressed (0.04–0.4 mU/liter), had no increased risk of cardiovascular disease, dysrhythmias, or fractures. It is unfortunate that we did not have access to serum free T4 concentrations in these patients to ascertain whether they were above or within the laboratory reference range. However, our data indicate that it may be safe for patients to be on a dose of T4 that results in a low serum TSH concentration, as long as it is not suppressed at less than 0.03 mU/liter. Many patients report that they prefer such T4 doses (9, 10). Figure 2 indicates that the best outcomes appear to be associated with having a TSH within the lower end of the reference range.
Hi Slow Dragon, there is a lot to think about here. Many thanks for responding in such detail. I am going to take some time to go through all of this then may come back to you if that’s ok. Yes, I did slowly increase the levo in 25mcg increments over 7ral months with follow-up blood tests but having done this was still horribly symptomatic, which is what prompted the DIO2 test and subsequent addition of T3.
Many (most?) on levothyroxine plus T3 find they need BOTH Ft4 and Ft3 at least 60-70% through range or higher (testing 24 hours after last dose levothyroxine and 8-12 hours after last 1/3rd of daily dose T3)
Just to add a little to what SlowDragon has said and not to contradict in any way. I'm one of those who can't quite get ft4 and ft3 as high as that on combo so it is ok to have slightly lower results When I started on combo I was aiming for ft4 and ft3 to be 60%-70% through their ranges as I'd read about it quite often from different folks on here. However hard I tried I could manage to get my ft4 higher than 50% measured at its lowest and my ft3 sits about 72% measured at its average. After 2 years of trying different doses I realised that I needed to be on a set dose longer term so I settled for those percentages through range and have continued to see symptoms ease.
We are all different Lalatoot. And it's ultimately what is the best level for you that truly counts. Percentages are only guidelines not definitive. I know of someone else who felt best on levels you describe. It's why signs symptoms and how you feel are really important. Shame doctors no. longer take not of these any. more! Wish you well on your journey.
Please could you check the link to the ncbi.nlm (second to last ref) as it says it cannot be found and I am gathering articles to fire back at the Endo. Thanks.
As you can see, my T4 and T3 are optimal - bang in the middle there - bless 'em!).
Optimal doesn't mean " bang in the middle" it refers to the exact point in the reference range where one is symptom free. This will vary from person to person.
T3 reduces both TSH and FT4
FT4 is ideally tested 24 hours after the last dose and FT3 after 12 hours
Testing 2/3 hours after dosing will hit the post-dose peak and may show your labs as falsely elevated ....the labs may be lower for the rest of the day.
The post- dose peak is therefore unreliable and may result in your hormone dose being wrongly reduced due to the transient higher hormone levels
So long as FT3 remains within ref range you are unlikely to be overmedicated
Once medicated TSH is no longer a reliable marker...you are correct to avoid medication by TSH level
If you feel well on your current dose refuse to accept a dose change without both FT4 and FT3 being tested.....before 9am and at least an hour away from food and drinks....but maybe not that easy unless you test privately!
I've just come in from a GP consultation about Chronic UTI and if was like hitting my head against a brick wall. I'm now convinced it's ( along with other health issues) the result of decades of low cellular T3. Medics receive that as if I have two heads!
I'm also Dio2 snp/homozygous.....which has a greater impact on conversion than if heterozygous
Hi DippyDame, many thanks for responding. Yes, I don’t normally do a test 3 hours after meds but my functional health doc (who is an endo) wanted me to do this. I suppose, she wanted to assure herself that the T3 wasn’t causing a spike. Once again, lots to take in here. Much appreciated!
But T3 always will rise then fall fairly quickly it's the nature of the product. What's in the blood level does not describe what happens at cellular level as Dippy dame explains so well. It just annoys me about the way endos obsess with blood level of T3 and do tests out of known paremeters. What is the point of this?
I wonder, is it that we metabolise hormones differently maybe? Meaning, some of us can live with a peak and metabolise slower (and cells uptake is slower? Maybe hmm) and some of us metabolise quicker and can't have it peaking too fast. It's something I'm trying to figure out myself, but I have no clue if this is even correct in any way!
I really don't know. I think what Dippy Dame said is more likely that some people need more T3, to act as a battering ram to get the T3 into the cells.I just find NDT a smooth experience no ups or downs just a constant even level all the time.
I do my blood tests with and without medication prior. I notice that when I’ve taken my meds prior the T4 and T3 levels go up and down when I’ve not taken them , both ways are in range results. However , my TSH always remains a similar figure again in range but only just at about 1.00ish. Does your T4 and T3 levels change??? This way of bloods checking keeps my Drs, GP and Endo happy so they prescribe T3 without question. Most importantly I feel good and symptom free keeping in range. It’s hard to understand why your levels are not going over range but your TSH is suppressed.
Hi mcpammy, re. 'It's hard to understand why TSH supressed if not going over range'.
For quite a lot of people, even those on levo only , TSH can sit a little below range even though their ft4 is well within range when Levo is taken on morning of the test . Back when i still used to take levo as usual on morning of test, I had 10 yrs of results where TSH was always 0.05 -0.4 ish, while ft4 varied between about 50- 80% (and when fT3 was occasionally tested it was about 30-50%) So in my case i have no reason to suspect that fT4 (or fT3) spiking over range for a few hrs after Levo dose was the cause of my below range TSH .
Endo's seem to struggle with with this individuality ~ some patients, like you, will keep TSH in range as long as their fT4 /fT3 aren't spiking over range , but some will have TSH below range even though their fT4/ fT3 are staying comfortably within range all day.
One time when i was actually overmedicated and had symptoms of such , my TSH went a bit lower 0.02 ish. So it seems to me that my 'personal' range for TSH does not match exactly with the '95% population range' .. my 'bottom end' is just a bit lower if you see what i mean .
I'm one of those Tattie. My TSH was below range at 0.19 with ft4 at 60%and ft3 at 17%. These figures were fairly consistent for me and got me NHS liothyronine.
I wonder if the TSH stops working properly. My TSH remained consistant suppressed even when my thyroid hormones plummeted downwards rapidly. TSH on its own would have indicated I was over prescribed.... In reality my Ft4 & Ft3 were at the bottom of the range and still dropping rapidly. In my case the TSH is pointless.
This seems to be the case for me too! One of the GPs reduced my meds about 18 months ago. When I went for the follow-up FT4 and FT3 had dropped to the bottom of the range and TSH hadn't budged!
Hi McPammy, many thanks for responding. In answer to your question yes T4 and T3 do fluctuate slightly but always within a narrow margin and they never get near the top of the range. I feel good and symptom free at the moment and just want to be left alone.
Content on HealthUnlocked does not replace the relationship between you and doctors or other healthcare professionals nor the advice you receive from them.
Never delay seeking advice or dialling emergency services because of something that you have read on HealthUnlocked.