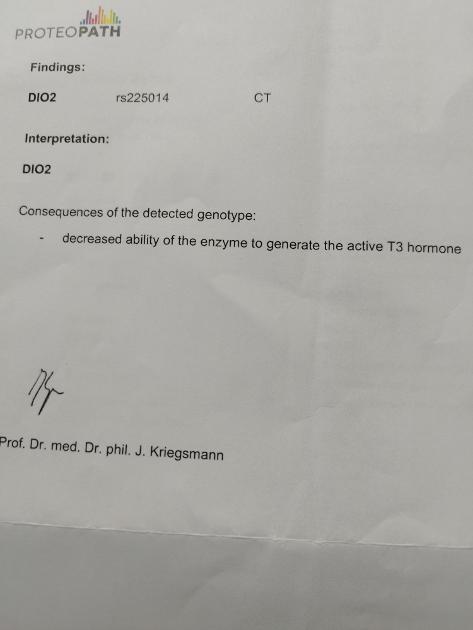
Hi allI would appreciate if any of you knowledge people could expand on my DiO2 test result from Regenerus Labs.
Yes I totally understand the overall result indicates a possible T4/T3 conversion issue but without needing too much technical info what do the numbers and CT mean?
My endo had neither the time nor inclination to expand on this result.
I also have a question about recent Syncathen Test Result but probably be better to start a different post for it
Any help would be much appreciated
Written by
Hollybushroad
To view profiles and participate in discussions please or .
Common Variation in the DIO2 Gene Predicts Baseline Psychological Well-Being and Response to Combination Thyroxine Plus Triiodothyronine Therapy in Hypothyroid Patients
No doubt I will be posting again re Synacthen result but got so many questions about my crazy cortisol I don't even know where to start so will leave that one for tomorrow.I always like to read your reply posts as they are very informative. Thanks again😄
I see you had the requested explanation already so just to add my practical experience of it…..
I have the exact same and all the local endocrinologists are also dismissive and disparaging about doing the test and its significance - how wrong they are…. In order to meet their challenge that it had no significant effect on my conversion I went onto levothyroxine only replacement for 2 years and varied the dose over 3 monthly periods measuring free t4 and free t3 and TSH , clearly and unequivocally my fT3 was always below normal unless fT4 was at or above maximum.
On top of my direct negative experiences of trying to manage on levothyroxine only, it is widely reported that excess fT4 is potentially damaging in itself, with many adverse effects. Consequently, I dropped fT4 to normal levels but which, for me and my DI02 disability, conversion could only yield bottom of the range fT3 leaving me chronically hypothyroid (despite normal levels of f T4)….. Adding Liothyronine and replacing both T4 & T3 at physiological proportions (85mcg T4 5-7 mcg T3 for me, down from 125 mcg T4 alone) completely resolved symptoms and produced euthyroid normal blood levels (16 fT4 4.5 fT3 1.5 TSH). Even without the DI02 test, or other evidence the defect does impair conversion, such fT4 blood levels with dragging fT3 are patient centred PROOF of a conversion problem/defect and if tied to symptoms the medics should be prescribing t3. Otherwise it’s a simple case of disability discrimination and lack of patient centred care, which is our right enshrined in the NHS constitution. Making a formal complaint on these grounds may be enough to drag them into the 21stC…….
It wasn't so much that endo was dissmiive of the gene test as he does recognise this can be helpful to know when deciding treatment (( He's private) In Pts with very low baseline T3I and High range T4 . It was more I found overall my appt was generally very rushed and I hadno time to ask questions as he kept looking at the clock above each time I would ask a new question. It was very much a 10 minute "business transaction" for him
That very useful info thank you. Im stuck, for years now, also Dio2 CT, various combos of T4, NDT , T3 only but not yet T4/T3 synthetic combo , as I have yet to find a Levo recently that doesnt make me itch or head spin.
Can I ask, when you found your sweet spot with T4 /T3 combo, do you split the doses? do them nighttime etc?, what worked for you please?
Did you have any gut issues and if so were they finally resolved?
It was a long and rocky rocky road, whether I'm on the straight and narrow remains to be seen but......
like you I felt stuck after various regimens which didn't work well or were absolute hell albeit with glimmers of hope from each of the bad jobs!... in that I found high T3 combos made me overly anxious and irritable and created almost addiction to the next dose and a roller coaster of highs and lows, metabolically speaking. And Levothyroxine indeed made my head spin at the doses prescribed to be taken all at once (possibly something to do with the negative feedback on T4-T3 conversion) and because T4 builds up insidiously, up and up and suppresses TSH. Titrating T4 is difficult and time consuming to zero in on the amount of T4 that gives the best free T3 because of T4's long half life. Plus, simply chucking in too much T4 overall in the chase for decent conversion of T3 aint good for the heart!
So; there are many reasons to reduce T4 to a permanently stable optimal (healthy normal fT4) dose and the only way to do that when T4-T3 conversion is sub-optimal is to add T3! Using NDT isn't great because it costs and T3 should be free on the NHS, IF you can prove you need it to get normal levels of fT3 & fT4, whereas NDT is never on the NHS.
I started splitting levothyroxine into 5 x 25mcg because of so many adverse effects of large single or even double doses night and morning, including mild gut disturbances. The 5 were equally spaced, which did mean taking it during the night and taking it closer to food and drink than the prescribing notes call for - did that make any practical difference to absorption or have obvious gut issues? NO.
I was able to get better levels of fT3 by splitting T4 BUT it still require way too much T4 because of my conversion disability, as seen in my blood levels at the top of or exceeding lab range fT4 to get even modestly normal fT3 but eventually increasing cardiac ectopics and arrhythmias. However it was a useful lesson in the benefits of splitting T4 because T3 also benefits from splitting so now I combine T4 & T3 in physiological proportions 3 times over 24 hrs which isnt so bad to manage and keeps fT3 and fT4 at normal euthyroid levels (and TSH as it happens). And no gut issues I could observe.
So the split dose that does for me is 25mcg T4 plus 2.5mcg T3 three times a day or some small variation around that because T3 replacement allows micro adjustments according to changinhg physiological needs, such as temperature/season/activity etc. in ways that are not even possible to adjust for with T4 alone. This is completely physiological because of the short half life of T3 and that the healthy thyroid gland adjusts T3 first then T4 and in so doing contributes 20% of total T3 directly, no peripheral conversion required - the human body must have evolved to do that for a reason!......
In my experience all the issues with levothyroxine come from unphysiological dosing, perhaps especially for people who are disabled in their capacity for converting T4 - T3?... It is also absolutely clear from vast amounts of observational population data that the NORMAL euthyroid range for fT4/fT3/TSH (14-16/4.2-4.8/1.5) is remarkably narrow compared to the typical lab ranges, which are far far too wide to say that someone can be anywhere in it and be OK. I mean some individuals may be off the normal healthy euthyroid range but somewhere apart from their healthy optimum in the lab range could be as off for them is it is for most people who should be within the normal healthy range. The typical lab range does not tell anyone where anyone should be to ameliorate their symptoms as well as thyroid hormone replacement could do...
If the normal euthyroid levels are exactly that - statistically normal, then surely for most people who don't know where they should be aiming their therapeutic interventions these euthyroid normal levels should be the first port of call for replacement therapy? Whatever replacement therapy gives normal euthyroid blood levels AND no adverse symptoms then so be it, whether that is NDT, T4, T3 or some combination.
A final note, on top of the obvious caution in case we are uniquely different with all of this, is that when adding T3 to T4 a little goes a long way and it takes weeks if not months for the T4 to come into balance with replacement T3. So changes have to be small and stable for at least a month to measure the trend in blood levels and observe symptom responses. I started with quarters of a 5 mcg T3 tablet split 4 times over 24 hrs with 25mcg T4 and then gradually reduced the number of doses and the amount of T4 while gradually increasing T3 to a max of 7.5mcg/24hrs. This is round-about what the healthy thyroid gland produces and I am now mostly symptom free, so something must be about right.......
Thank you for taking the time to reply, and with such detail.
Somethings you have said have really struck a chord, such as trying to get enough T4 in to get the T3 you need, and requiring another sort of hit of T3. But never really being able to achieve our balance by too little of one and too much of another etc etc, to fit ranges.The bugbare for me are the ranges which my GP told me were set based on a 22 year old healthy male. Well I am female, 65 and DIO2 +............I except that it is not ideal to have a suppressed TSH, and not acceptable to have out of range T3, but where are the physicians knowledgeable enough to help us, and guide us so clearly as you have demonstrated. Everything you have said makes logical sense. Thank you.
I like many on this forum have been left .Now I am very weak,incapacitated and just left to work out what to do next. Until I read your words yesterday I think I had pretty much given up. After a demoralising, bullying endo consultant f/u recently ending in me being verbally dismissed as a waste of time, waste of her time,and waste of an NHS appt. But you have spurred me to try your approach.
I am not sure how to go about this as I currently take 1 3/8 grain grains NDT split in 2 doses, this puts my TSH just out at 0.067, T4- 17, T3- 5. I like you think the T3 side of the NDT at this amount makes me anxious, but I need more T4 to do its thing.
I am constantly afraid, because I feel so awful and incapacitated now, to feel even worse by starting over again. Is it possibly did you find, to say drop out my afternoon dose of NDT in favour of Levo equivelent, or did you find it better to take out all your NDT and straight swap to Levo and Lio.?
I too in the past could only tolerate 1.25mcg of Lio (on T3 only reg ) to start with, but was always edgy on it.And I always waited 6 weeks before a change an amount of anything.
Have you ever noted a difference between Liothyronine Hydrochloride and Liothyronine Sodium at all?
Thank you for making me rethink after , I suspect I need less of everything current but a higher proportion of T4-T3 than I am currently getting and/or able to tolerate.I have been struggling with these meds 8 years now, and I really cant afford NDT anymore despite its smoothness.
I am so sorry you have had such a lousy time in the past, but very inspired and glad to know you have some quality of life now.
I am so sorry to hear of your experience with the NHS consultant; although sadly I am not surprised; I had the same, repeatedly and I am now in the throes of a second formal complaint against him for bullying and clinical negligence and lack of patient centred care. They should not be allowed to get away with it, their ignorance and arrogance combined is utterly unacceptable. Endocrinologists seem to be among the very worst of the worst of the profession and the NHS. Perhaps endocrinology is too difficult for these ‘doctors’ to really understand anything beyond diabetes so they are constantly in the defensive and blaming the patients.
Anyway….. without being sure what your personal optimal levels for thyroid hormones are I would hazard a guess based on my personal experience that your TSH is actually telling you that you need less and T4 and T3 but that in swapping out NDT at first you could perhaps drop T4 only slightly and leave T3 the same overall and see what happens… So you wouldn’t be starting all over again but continuing the ongoing process of finding your optimum.
Personally I think there’s a lot of red herrings in type of T4 and various other supplements vitamins etc., with the possible exception of selenium for thyroid metabolism. T4 & T3 are so powerful that whatever form you get them and whatever supplements you may or may not be taking are probably irrelevant compared to how near or far you are from the optimal doses for you Unless you have a strong allergy to a pharmaceutical excipient in say a brand of Levothyroxine compared to another I would say forget about everything but the mcg dose amounts and timing, and then the resultant blood levels and symptoms!
On timing…. I dose to allow a circadian rhythm of TSH, which means taking my combos at midnight, waking and midday then nothing until midnight again; this allows TSH to rise as it should to a peak around 2am and low point at 2pm - assuming you haven’t suppressed it totally by chronic overdosing of T4 and or T3!…. That completely annihilates the natural circadian rhythm., again its there for a reason, whether we fully understand it or not!
So, if I were you (and I have been I would definitely seek to replace NDT with levothyroxine and Liothyronine and you absolutely can do that quite quickly if you match the doses up, mcg for mcg, then adjust the synthetics gradually to lower the free T4 and work toward normal healthy thyroid hormone balance, which hopefully will be as good for you as it is for all the normally euthyroid people in the world:). If I remember right from the Baltimore study on ageing, looking at tens of thousands of individuals by decade of age and sex, normal fT4 for your (and my) decile is around 14-15, fT3 around 4.4 and TSH around 1.5; you could aim for that from whatever you take to get it! ……
In my experience the synthetic hormones are indistinguishable from the NDT once the doses are giving appropriate blood levels. Often when we think its the type or specific medication itself causing a problem its actually simply incorrect dosing (overall and timing). Don’t give up, you’ve got this!
Firstly my apologies for not responding a week ago to your very kind encouragement and explanation of what perhaps I could try next. I have had an absolutely dreadful week, same old, same old rollercoaster, weak,fatigue,gut ,etc.
Whilst I make sure I can get T3 suppy in place (tricky) I have started moving some of the NDT to bedtime dose, rising and nearly midday ish........its not going that well, but I am persevering. This will help me adjust the switch over to Levo/Lio I am hoping. A week of changes, clocks back,cooler weather, meds timings have all impacted the week,but keeping positive.
My TSH is out of NHS 'range' but how does one know if it's totally suppressed. What figure = zero? I suppose that is individual? Back in 2019 I was on 2 1/2 grs NDT and TSH was out of range for a year or more (felt dreadful/non functioning then too.) When I dropped NDT in 2020 to try T3 only regime for a year (felt so ill), previous kind Endo was astonished that my T4 plummeted in 6 dys from 20 -11 expecting it to be 28 dys + to clear, and TSH came back into range..........then I started adding back NDT up to this sorry state I an in now. Meaning I have unsupressed TSH before but that doesnt mean I can again.
I would be interested to know how you get on in the future with your official complaint about your Endo. I feel very uncomfortable knowing that 'bully' might be hurting and demoralising another, so I have decided when I have more energy I must report her. I am not entirely sure how to go about it. And I think you are correct, many Endos seem only to be interested in Diabetes, there doesnt seem to be any Thyroidolgist any more........ I wonder why ?
Im not sure 'ive got this' but Im giving it another good go. Thank you for being there.
sad to hear youre having a tough time of it. First of all I would say whatver theories anyone has about what should/may work for you no matter how well founded they may be, our body will tell us if it aint right for us. Sorry, I know that doesnt help other than it all being part of our journey of figuring it out.
So if taking NDT in the evening is causing disruption, particulalry to sleep I am immediately suspicious that its too much T3 from the NDT, its easy to overdose that because the ratio of T3:T4 in the NDT is excessive for humans. Dosing of NDT should be T3 led and for me anything over 1 mcg T3 at bedtime is too much, whereas I can take 3mcg on waking and another 3 at midday without purturbation. Also its worth considering that although T3 has a short half life it's still cumulative if we are taking more than we need!
As for what constitutes 'supressed' TSH, I have read that the concensus seems to be this is when TSH is a tiny fraction of the lowest point on the lab range e.g. 0.05 or even 0.2 because even 0.5 is low and a fraction of what it could normally rise to in healthy circadian cycle. I am pretty sure that very low TSH let alone totally supressing it isnt healthy, unless it is being clinically managed for thyroid cancer control for example. TSH has been associated as having other roles as well as feedback to the thyroid gland eg bone formation and even influencing T4-T3 conversion elsewhere. Whatever the scientific detail of that and any arguments around it, what is unequivocal is that healthy normal TSH is beween 0.75 and 2.5 so it seems logical, physiological, to aim for that if we are struggling to find our personal set-point for T3 T4 and TSH.
As a side note I feel much worse and unstable if my TSH is very low and T4 is high normal than I do if my TSH is high (eg 4-5) and T4 scrapping the bottom.... makes me think that even without a thyroid gland functionality TSH is doing something useful in ways we can only guess at...
Also, you may consider that you are making changes which could be in the right direction but they are disrupting the regimen you had established and even if that wasn't optimal our thyroid metabolism doesnt like what it may sense as unaturally profound changes...... It always amazes me how little T3 it takes to push me over the edge from optimal to overcooked, the difference is night and day!
The great thing about T3 over T4 though is that we can adjust it and find an optimum in a matter of days rather than weeks or months, so long as we are not making big changes all at once.
Also worth considering that seasonality (cold weather exposure) and varyimg demands on our overall metabolism will affect thyroid hormone balnce (demand and supply) and, without a functing thyroid gland, supply of first response T3, can only come from what we take as a pill particularly if we are poor converters! And this is TSH mediated! Another reason to allow TSH to do its thing by taking care not to supress it but also to follow it; a bit like riding a horse.... we push the horse on but also listen to it and allow it to guide us!!! weird metaphor for anyone that doesn't ride I know
if you are paying attention to it, you've got it:). maybe think of it as an experiment, you are your own clinical trial, be careful and mindful absolutely but accept that you may experience discomfort in pursuit of a liveable solution and if it gets too uncomfortable pause and take another blood test! Bulldozing on with changing medication without regular and frequent blood test can end up with us relying on guesswork to interpret symptoms which are sometimes counter-intuitive. I test monthly even if that is too soon to show a settled response to significant changes; at least it alerts me to vital signs heading too far in the wrong direction.
Thank you for taking the time to reply. I have experience some similarities, such as not being able to tolerate 2.5mcg T3 at bedtime (be it synthetic or within a 1/4gr NDT) but ok on 1.25mcg, but can tolerate up to 5mcg T3 ( or 5/8gr NDT) on waking ,provided there was reasonable sleep, but less tolerant of T3 in the afternoon, and feel that blurr slump 2hrs after afternoon dose that wears off in 6hrs......so that must be the T3.
However, you really really have made me think. I had been working on the basis that from the start of all this I had norm in range TSH 4,and rising with low in range T4 but struggling. When high TPO/TG and DIO2+ were diagnosed, the assumption was fluctuations of these hormones was causing the symptoms, and advised to medicate. And that I should be keeping the TSH as low as poss at 1ish, T4 18-20 and T3 5.5-6.............aint working for me.
Its possible back then I may have only needed a little T3....., I will never know, and it would not have been an option.
So thank you again, I will go back to the drawing board, look at getting TSH detectable again, and either add spread doses of T3 to the NDT, or better still revisit Levo and T3, and as you said it will be so much easier to monitor this and simpler through climatic changes.
'T4 18-20 and T3 5.5-6.............aint working for me.' hah ! no I am not surprised, it may seem only a little over mid range and well in lab ranges but as we know that dont mean ****It could even be profoundly excessive with other health complications as well as being a hypothyroid treatment fail and, sadly it also allows doctors to dismiss us as treated but neurotic. It seems to me that in most hypothyroid treated cases TSH should be allowed to float at what would be normal for a euthyroid person eg 1-2! If someone isnt getting on with that I would question whether the fT4:fT3 balance is optimal? TSH responds to T4 and T3 so it can look right under the influence of only fT3 or fT4 whereas in the healthy normal system it is BOTH that are inextricably linked to act physiologically with TSH. I suspect the best we can do is seek to manipulate TSH with replacement T4 & T3. Another guide to that, apart from sympom relief of course, is that a ratio of fT3:fT4 of 3-3.3 has been comprehensively linked with normal TSH in healthy normal thyroid blood panels.
I think I may have been guilty in the past/ say 5 years ago of adding NDT increments too quickly, and therefore I thought more recently may have missed my sweet spot back then. I did at one time back then feel a flicker of improvement and thought this to be ok ish, but very fatigued when T4 hit 18 but that was on NatureThroid (much less potent than Armour to me) And then 3 years ago best of all on 1grain + 7mcg T3 still fatigued ,but that put T3 at 13 me jittery, fast pulse and Endo with concern.
This time round building up Armour NDT I have waited at least 9 - 12 wks before a dose increment and still housebound.So it has got to be either more T4 and less T3 ,or less T4 and more T3. To work as you suggest with a detectable TSH.
Either way , I shouldnt be freezing cold all summer, very low temp and BP, along with all the other bits sand bobs that drop off with this disease. !
from you said so far if I remember it correctly its likely less of both! Which seems counter-intuitive since you have profoundly hypothyroid symptoms… But, too much T4 can be like too much sugar - causes a crash and sudden low blood sugar!and too much T3 well that just blows out socks off and can disrupt the body’s attempts to stabilise….. Sounds like you need to estimate the amounts of levothyroxine and liothyronine that should give normal TSH and make adjustments toward that, without NDT and with monthly blood tests of thyroid levels from blood taken the same time of day (or night) every time! I wonder if you could manage on 100 + 5 mcg levothyroxine/Liothyronine for long enough to get a blood test to show the effect of that for 4-6 weeks?>….. Then you could se where free T4 sits and whether you can lower the levothyroxine dose, although it does seem to take more like 2 months for long term over supply to dissipate. You could make MICRO adjustments to the liothyronine if you’re feeling acutely hypo during this process of finding your baseline but try to keep whatever feels right stable with minimal adjustments (eg +- 1mcg!).. In my experience the amount of T3 & T4 we need are inextricably linked and changes in the free amounts in the blood of one will affect the other so it is a fine balancing act for sure, the trick is to dampen out fluctuations caused by any mismatch in demand and supply. Regular and consistent Blood test are crucial to this !
I was actually thinking (once assured I can get more T3 in place) that if I switch from my of the last 2 weeks of 1 1/4 gr NDT ,go over to Levo/T3 , by switching it to a gentle 75mcg of Levo + 5mcg T3 in split doses (that would be approx = to 1 gr NDT ish) this would be a drop down of a 1/4 gr (and within 6 weeks that would have been a drop of 1/2gr Octobers dose, im less edgy too) but gives room for adjustment upwards.
Or did you ever when you were fine tuning, just start Levo, test, move Levo up and down, then later added in T3 as you fine tuned?
I agree blood test at same timings etc very useful. Thank you for taking the time to reply.
Two years trail of levothyroxine only, adjusting that is …. Difficult to interpret symptoms, disruptive, and hugely time consuming in the sense it takes so long for the changes to yield a stable fT4. Short of an apocalypse I will not go back to that!
Finding a stable levothyroxine baseline which may, without sufficient T3, feel undermedicated seems better that pitching T4 too high and working back with both T3 and T4 potentially combining to suppress TSH …
And yes starting your levothyroxine at 75 with potential to add a bit after first month or two…. You could add in an extra mcg of T3 if you are feeling hypo during that period. Almost as if you were just diagnosed and beginning medication…
Ive felt hypo continuosly for 14 years , bar 3mths when I was on 1gr NDT 7.5mcg T3 which put T3 levels at 13 and me a bit wired, edgy. And unhappy Endo.
Content on HealthUnlocked does not replace the relationship between you and doctors or other healthcare professionals nor the advice you receive from them.
Never delay seeking advice or dialling emergency services because of something that you have read on HealthUnlocked.

") Unless you have a strong allergy to a pharmaceutical excipient in say a brand of Levothyroxine compared to another I would say forget about everything but the mcg dose amounts and timing, and then the resultant blood levels and symptoms!
Unless you have a strong allergy to a pharmaceutical excipient in say a brand of Levothyroxine compared to another I would say forget about everything but the mcg dose amounts and timing, and then the resultant blood levels and symptoms! ")