Hi, I’d appreciate your opinion on my daughters latest results . She is in thyroxine but still has symptoms of under active thyroid. Her GP wouldn’t authorise test so we paid private.
latest blood results : Hi, I’d appreciate your... - Thyroid UK
latest blood results
Written by

BRITT1DENMARK
To view profiles and participate in discussions please or .
Read more about...
26 Replies
•
PurpleNailsAdministrator
What is her current dose? Previous post said levothyroxine - 150mcg.
GP wanted to reduce to 125mg. Was her dose reduced?
How long has she been on current dose level, & does she has same brand.
Was test done as recommended on forum?
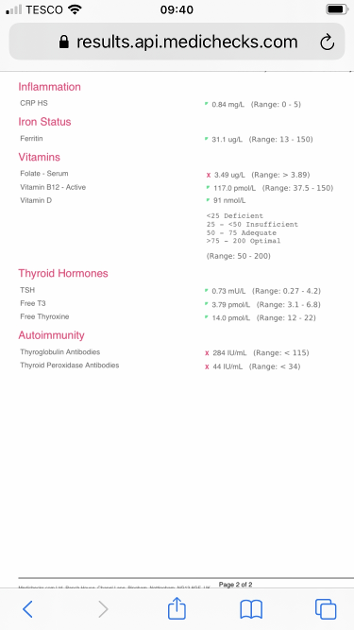
Folate & ferritin very low - Deficient. Needs further investigation.
Edit: I previously noted - Antibodies currently negative. Have they been positive previously? but they show as positive. Not sure how I misread. Sorry for any confusion.
Hypothyroidism from non autoimmune is treated in same way.
Was her TSH high when diagnosed? - How long has she been in levothyroxine?
PurpleNails
Antibodies currently negative. Have they been positive previously?
Antibodies currently positive, they are both showing well over range.
Hi, She’s on 125mg for about 6 months . Not sure if her TSH was ever high, I’ll check
This reply is meant for PurpleNails
Yes sorry
That's OK, I've tagged PurpleNails so they'll know now ")
So continuous dose for 6 months gives a settled level. (Always test after an unchanged & consistent dose of minimum 6 weeks)
The FT4 & FT3 are too low in range. GPs tend to look at TSH and may say as thyroid levels in range it is adequate. You can push for increase stating how low in range levels are and if symptoms are present on lower dose, better in higher dose.
NICE guidelines are the steps that GP are recommended to follow. In the strictest sense it is not compulsory and Doctors / -working with patients- can use their judgement to vary treatment if appropriately justifiable.
A group or surgery can’t choose to practice a different protocol if in disagreement with advice.
When doctors don’t follow or deviate from the crucial steps they are open to fault (and possible disciplinary / legal action)
So you can quote nice guidelines to argue for further investigation.
You can also say following the advice to keep TSH in range for example - is not appropriate as this would keep you unwell so knowing the potential consequences (doctors say low TSH causes heart and bone issues*) you (your daughter) would prefer to be treated adequately to feel well.
Low TSH is usually associated with high thyroid hormones - but here the situation is different.
Thank for your response. The gp said her last TSH indicated she was over medicated and wanted to lower her thyroxine again, that’s why we had the test done privately. They wouldn’t do full thyroid check, as TSH level was ok. I’ll find out the last TSH result
SeasideSusieRemembering
BRITT1DENMARK
TSH: 0.73 (0.27-4.20)
FT4: 14 (12-22)
FT3: 3.79 (3.1-6.8)
FT4 and FT3 currently show that she is undermedicated. The aim of a treated hypo patient on Levo only, generally, is for TSH to be 1 or below with FT4 andFT3 in the upper part of their reference ranges. FT4 is only 20% through range and FT3 is 18.65% through range, so an increase in Levo is indicated - 25mcg now and rtest in 6-8 weeks.
Thyroid antibodies are postive and confirm Hashi's (auto immune thyroid disease). This is likely to be the cause of her dreadful ferritin and folate levels mentioned below.
Ferritin is dire, if it was less than 30 then NICE consider that to be iron deficiency. GP should do an iron panel consisting of serum iron, saturation percentage, total iron binding capacity and ferritin, this will show if she has iron deficiency or just low ferritin. GP should also do a full blood count to see if she has anaemia. You can have iron deficiency with or without anaemia.
B12 and Vit D are OK.
Folate is dire and may be indicative of folate deficiency, again she should see her GP, see:
cks.nice.org.uk/anaemia-b12...
Folate level
◦Serum folate of less than 7 nanomol/L (3 micrograms/L) is used as a guide to indicate folate deficiency.
◦However, there is an indeterminate zone with folate levels of 7–10 nanomol/L (3–4.5 micrograms/L), so low folate should be interpreted as suggestive of deficiency and not diagnostic.
SlowDragonAdministrator
Her ferritin is terrible
Is she vegetarian or vegan
Or heavy periods?
Request GP do full iron panel test for anaemia
cks.nice.org.uk/topics/anae...
In all people, a serum ferritin level of less than 30 micrograms/L confirms the diagnosis of iron deficiency
Also See page 7 on here
rcn.org.uk/-/media/royal-co...
Look at increasing iron rich foods in diet
Eating iron rich foods like liver or liver pate once a week plus other red meat, pumpkin seeds and dark chocolate, plus daily orange juice or other vitamin C rich drink can help improve iron absorption
List of iron rich foods
Links about iron and ferritin
An article that explains why Low ferritin and low thyroid levels are often linked
preventmiscarriage.com/iron...
irondisorders.org/too-littl...
davidg170.sg-host.com/wp-co...
Great in-depth article on low ferritin
oatext.com/iron-deficiency-...
drhedberg.com/ferritin-hypo...
This is interesting because I have noticed that many patients with Hashimoto’s disease and hypothyroidism, start to feel worse when their ferritin drops below 80 and usually there is hair loss when it drops below 50.
Thyroid disease is as much about optimising vitamins as thyroid hormones
healthunlocked.com/thyroidu...
restartmed.com/hypothyroidi...
Post discussing just how long it can take to raise low ferritin
healthunlocked.com/thyroidu...
Never supplement iron without doing full iron panel test for anaemia first and retest 3-4 times a year if self supplementing. It’s possible to have low ferritin but high iron
Medichecks iron panel test
medichecks.com/products/iro...
Iron and thyroid link
healthunlocked.com/thyroidu...
Posts discussing why important to do full iron panel test
healthunlocked.com/thyroidu...
healthunlocked.com/thyroidu...
Chicken livers if iron is good, but ferritin low
healthunlocked.com/thyroidu...
Heme iron v non heme
hsph.harvard.edu/nutritions...
Good explanations of iron
theironclinic.com/iron-defi...
theironclinic.com/ironc/wp/...
Thanks for your reply. She isn’t vegetarian and hasn’t been having regular periods till the last couple of months
SlowDragonAdministrator
High thyroid antibodies confirms autoimmune thyroid disease also called Hashimoto’s
Is she on strictly gluten free diet
If not request coeliac blood test via GP BEFORE considering trial on strictly gluten free diet
nice.org.uk/guidance/ng20/c...
1.1.1 Offer serological testing for coeliac disease to:
people with any of the following:
persistent unexplained abdominal or gastrointestinal symptoms
faltering growth
prolonged fatigue
unexpected weight loss
severe or persistent mouth ulcers
unexplained iron, vitamin B12 or folate deficiency
type 1 diabetes, at diagnosis
autoimmune thyroid disease, at diagnosis
irritable bowel syndrome (in adults)
first‑degree relatives of people with coeliac disease.
We are having a struggle with the GP. Can I quote this site when she speaks to them?
BRITT1DENMARK
Certain say that you have spoken to ThyroidUK who are recommended by the NHS as a source of information about thyroid disease. However, best not to mention the internet or forums, they dislike that and will ridicule it. Just say you've been in touch with ThyroidUK or spoken to them and they have advised you......
Thank you
SlowDragonAdministrator
She’s currently under medicated
Ft4 and Ft3 too low
Getting all four vitamins improved to OPTIMAL levels essential
High B12 (especially with low folate) can be deceiving
Paradoxical B12 deficiency
b12oils.com/paradoxical.htm...
Frequently necessary to supplement vitamin D and vitamin B complex continuously
Does she always get same brand levothyroxine at each prescription
Many people find different brands are not interchangeable
Strictly gluten free diet can give astonishing improvement, but get coeliac test first
Hi thanks for your reply. She isn’t gluten free.
Hi, everyone on this chat is saying she’s under medicated but the gp is saying she’s in the normal range. Do you know if endocrinologist recommends levels should be in high end of range please. Many thanks
GP is just looking at low TSH
Low vitamin levels tend to lower TSH (because of poor conversion of Ft4 to Ft3)
Are you in U.K.
Email Thyroid U.K. for list of recommended thyroid specialist endocrinologist and doctors
tukadmin@thyroiduk.org
Ft4 should be at least 50-60% through range
Thank you, I have ordered the list of specialists
BRITT1DENMARK
They are all taught that it's only TSH that matters. Unfortunately.
TSH is useful for diagnosis but that's basically where it ends. Once diagnosed and treated the TSH has no real importance because it's a pituitary hormone not a thyroid hormone. It's the thyroid hormones - FT4 and FT3 - that show our thyroid status and it's these - more importantly the FT3 (which is the active hormone that every cell in our bodies need).
The NICE guidelines don't mention this and the only information we have that may possibly be taken into account (but no guarantee) is the article by Dr Toft, past president of the British Thyroid Association and leading endocrinologist, who states in Pulse Magazine (the professional publication for doctors):
"The appropriate dose of levothyroxine is that which restores euthyroidism and serum TSH to the lower part of the reference range - 0.2-0.5mU/l. In this case, free thyroxine is likely to be in the upper part of its reference range or even slightly elevated – 18-22pmol/l. Most patients will feel well in that circumstance. But some need a higher dose of levothyroxine to suppress serum TSH and then the serum-free T4 concentration will be elevated at around 24-28pmol/l. This 'exogenous subclinical hyperthyroidism' is not dangerous as long as serum T3 is unequivocally normal – that is, serum total around T3 1.7nmol/l (reference range 1.0-2.2nmol/l).*"
*He confirmed, during a talk he gave to The Thyroid Trust in November 2018 that this applies to Free T3 as well as Total T3 and this is when on Levo only. You can hear this at 1 hour 19 mins to 1 hour 21 minutes in this video of that talk youtu.be/HYhYAVyKzhw
You can obtain a copy of the article which contains this quote from ThyroidUK
Email : tukadmin@thyroiduk.org
and ask for the Dr Toft article from Pulse magazine. Print it and highlight Question 6 to show your doctor.
Also, our member Diogenes is Dr John Midgeley who is a thyroid researcher and advisor to ThyroidUK (and one of the inventors of some of the thyroid function tests) and he has made many posts about this and links to many studies that he has had published so you could check out those for helpful information. One of his recent posts states:
This is what my colleagues and I wrote as a summary to a paper we had published:
It appears that what we are witnessing constitutes an unprecedented historic change in the diagnosis and treatment of thyroid disease, driven by over-reliance on a single laboratory parameter TSH and supported by persuasive guidelines. This has resulted in a mass experiment in disease definition and a massive swing of the pendulum from a fear of drug-induced thyrotoxicosis to the new actuality of unresolved designation of hypothyroidism. All of this has occurred in a relatively short period of time without any epidemiological monitoring of the situation. Evidence has become ephemeral and many recommendations lag behind the changing demographic patterns addressing issues that are no longer of high priority as the pendulum has already moved in the opposite direction. In a rapidly changing medical environment, guidelines have emerged as a novel though often over-promoted driver of unprecedented influence and change. Treatment choices no longer rest primarily on the personal interaction between patient and doctor but have become a mass commodity, based on the increasing use of guidelines not as advisory but obligatory for result interpretation and subsequent treatment. Contrary to all proclaimed efforts towards a more personalised medicine, this has become a regulated consumer mass market as with many other situations. This is of little benefit to patients who will continue to complain, and with some justification, that the medical profession is not listening, thereby abandoning one of its primary functions in the doctor-patient relationship.
This is very helpful, thank you
Do you know anything about central hypothyroidism?
Yes. Central Hypothyroidism is where the problem lies with the pituitary or the hypothalamus rather than the thyroid gland.
With Central Hypothyroidism the TSH can be low, normal or slightly raised, and the FT4 will be low.
TSH is a pituitary hormone, the pituitary checks to see if there is enough thyroid hormone, if not it sends a message to the thyroid to produce some. That message is TSH (Thyroid Stimulating Hormone). If there is enough hormone then there's no need for the pituitary to send the message to the thyroid so TSH remains low.
In Primary Hypothyroidism, which is where the thyroid fails, the TSH will be high.
However, with Central Hypothyroidism the signal isn't getting through for whatever reason so the message isn't getting through to the thyroid to produce hormone, hence low FT4. It could be due to a problem with the pituitary (Secondary Hypothyroidism) or the hypothalamus (Tertiary Hypothyroidism).
There is no way Central Hypothyroidism can be diagnosed now that your daughter is being treated, you would have to look at her original results from before being prescribed Levo - was TSH below range or at the very bottom limit of the range? Once on Levo FT4 will rise so you just can't diagnose then.
To be honest, as far as treating the hypothyroidism is concerned, it will be the same whatever the cause - primary or central hypothyroidism or autoimmune (Hashimoto's)
If her original results do suggest central hypothyroidism then it may be useful to investigate further (scan), the pituitary produces other hormones so if it is at fault it would need to be established whether there were any problems in producing the other hormones.
Thank so much. Obviously I’m out of my depth. Just exploring every avenue. I really appreciate all of your responses and knowledge
This question may be missed as at end of post & to post in general (to yourself) not to specify person.
You may want to start new post about subject.
Here’s my information on central hypothyroidism.
Your daughters hypothyroidism is primary hypothyroidism - as confirmed by positive antibodies. Autoimmune Thyroiditis (also known as Hashimoto’s)
Secondary hypothyroidism is where there is an issue with the pituitary gland and does not produce sufficient TSH to stimulate thyroid. So TSH would not rise in response to low levels.
In tertiary hypothyroidism, inadequate secretion of thyrotropin-releasing hormone (TRH) from the hypothalamus leads to insufficient release of TSH, which in turn causes inadequate thyroid stimulation.
Both secondary & tertiary are referred to as central hypothyroidism.
All forms of hypothyroidism is treated by same method, replacing low thyroid hormones with levo.
It can be difficult to diagnose central hypothyroidism - as normal (in range) TSH are not investigated further and it can remain unknown FT4 & FT3 are low.
Not what you're looking for?
You may also like...
Latest blood results
Hi everyone, ive today got my latest blood results and would like some advice on your thoughts...
Latest blood results
Do these results look normal
Serum ft4 18.6 pmol/L (10.00-22.00)
Serum tsh 0.51 mU/L...
Latest blood results
Hello
My 17 year old daughter had a total thyroidectomy (March 2016) due to a large goitre...
Latest blood results.
Hi All,
Just got my latest results back super quick from blue horizon.
I only posted yesterday, how...
Latest blood results
Managed to get my last 2 blood results from docs
September:
Free t4 = 12.2 》 7.86-14.41...