Hello, I've posted about this before but thought I'd just see if anyone has any new ideas.
I've been treated for hypothyroidism (autoimmune) for the last two years and have had on average one appointment a month - which in some ways is lucky as I know many people struggle to see specialists, however, I don't really feel like I'm in a better place than when I started.
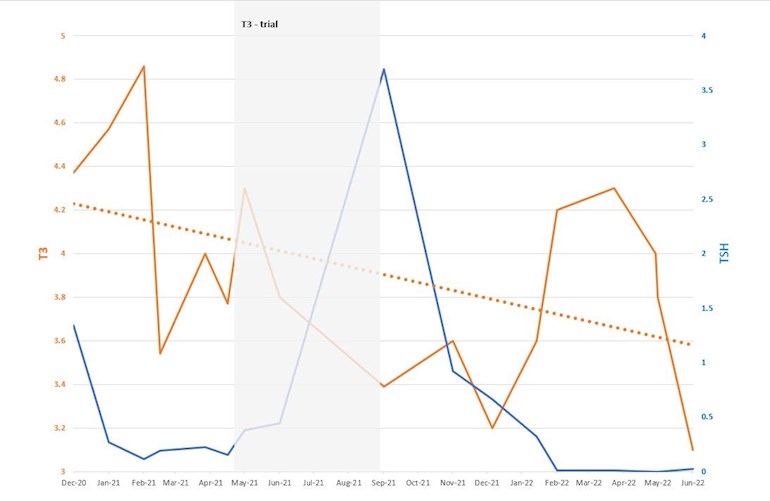
Initially I responded to levothyroxine (TSH came down, free hormones went up) but ever since I've been on a trajectory of upping my dose, seeing my TSH fall AND seeing my FT3 fall as well. I got to the point where I was taking 160mcg levo / day and my TSH was undetectable but T3 was still under halfway through the range. Several members made helpful suggestions which I explored, including getting pituitary tests (all came back normal), but now my T3 is the lowest it's ever been and my TSH is still suppressed (currently on 150/day). I've had the whole raft of hypo symptoms back again (poor sleep, back ache, SIBO relapse etc.) so I feel convinced I'm under-medicated, but I can't understand why my TSH isn't higher as a result. I know TSH isn't the be-all and end-all, but wouldn't I still expect it to be above where it is now for these hormone levels?
TSH: 0.02 (0.3 - 4.2)
FT3: 3.1 (2.4 - 6)
FT4: 13.9 (9 - 23)
(B12, Folate, Ferritin and Vitamin D are all nicely medium-high in their ranges).
To try to explain my concern to my endo, I charted my results over time...but not convinced it will get me anyhere. Any suggestions about what I can ask for in my apopintment tomorrow would be gratefully received!
")