Hello, I've been on levo since hypothyroidism was detected during my pregnancy in June 2019. I started on 25mg of Levothyroxine and this increased to 50mg last year. I still didn't feel well so I added some T3 and reduced my levo over the last few months. I currently take 6.25mg of T3 and 25mg of levo and have felt better save for some recent aches and pains (mainly tendons). My other results are as follows:
TSH 2.77 (0.27-4.2 mIU/l)
Free Thyroxine 13 (12-22 pmol/l)
Free T3 3.98 (3.1-6.8 pmol/l)
I don't think I ever had issues with my antibodies so would love advice of what this means. Do I have Hashimotos? Or could it be another autoimmune disease? I am almost 42 and take a number of supplements on top of my meds.
Thank you xx
Written by
Charltonjl
To view profiles and participate in discussions please or .
50mcg levothyroxine was only a starter dose, no wonder you felt terrible
Bloods should be retested 6-8 weeks after each dose change or brand change in levothyroxine
Most people on levothyroxine will need to increase dose slowly upwards in 25mcg steps until on or near full replacement dose. That’s typically 1.6mcg per kilo of your weight
Consider starting levothyroxine at a dosage of 1.6 micrograms per kilogram of body weight per day (rounded to the nearest 25 micrograms) for adults under 65 with primary hypothyroidism and no history of cardiovascular disease.
Traditionally we have tended to start patients on a low dose of levothyroxine and titrate it up over a period of months.
RCT evidence suggests that for the majority of patients this is not necessary and may waste resources.
For patients aged >60y or with ischaemic heart disease, start levothyroxine at 25–50μg daily and titrate up every 3 to 6 weeks as tolerated.
For ALL other patients start at full replacement dose. For most this will equate to 1.6 μg/kg/day (approximately 100μg for a 60kg woman and 125μg for a 75kg man).
If you are starting treatment for subclinical hypothyroidism, this article advises starting at a dose close to the full treatment dose on the basis that it is difficult to assess symptom response unless a therapeutic dose has been trialled.
A small Dutch double-blind cross-over study (ArchIntMed 2010;170:1996) demonstrated that night time rather than morning dosing improved TSH suppression and free T4 measurements, but made no difference to subjective wellbeing. It is reasonable to take levothyroxine at night rather than in the morning, especially for individuals who do not eat late at night.
Current results suggest you are very under medicated (hardly surprising on such low dose)
Recommended on here that all thyroid blood tests should ideally be done as early as possible in morning and before eating or drinking anything other than water .
Last dose of Levothyroxine 24 hours prior to blood test. (taking delayed dose immediately after blood draw).
This gives highest TSH, lowest FT4 and most consistent results. (Patient to patient tip)
If/when also on T3, make sure to take last third or quarter of daily dose 8-12 hours prior to test, even if this means adjusting time or splitting of dose day before test
Is this how you do your tests?
Taking any dose of T3 will significantly reduce TSH
Recommend you increase levothyroxine dose to 50mcg
Retest in 6-8 weeks
What vitamin supplements are you currently taking
Meanwhile test vitamin D, folate, ferritin and B12
All are likely very low when hypothyroid
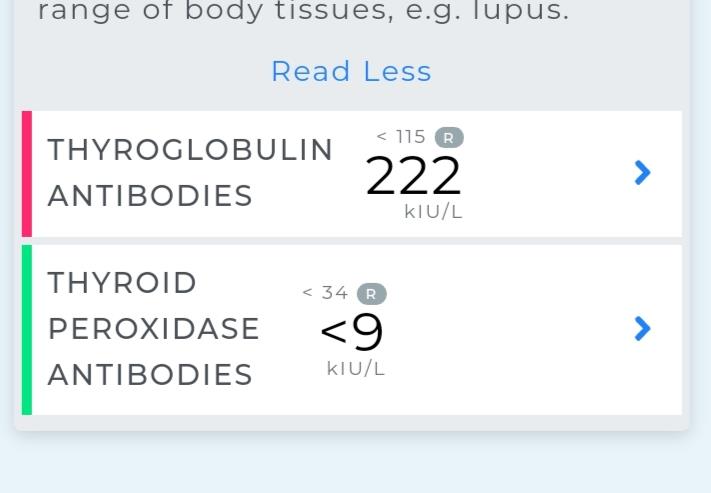
Your high TG antibodies confirms autoimmune thyroid disease, (Hashimoto’s) but currently NHS refuses to acknowledge this if ONLY TG antibodies are high
You might benefit from getting ultrasound scan of thyroid to confirm Hashimoto’s
Hello, thanks again SlowDragon. If you remember, my doctor and endocrinologist both refused to increase my levo dose after it was increased from 25mg to 50mg as they said my last test results (1st Nov 2020) were perfect despite me still having many issues. That's when I started taking T3 and it's made me feel better the last 2 months and I always thought it could be the levo making me feel bad.
I also always do my test first thing and take my last dose of levo 24 hours before and I also took my t3 10 hours before the test. I take the following supplements:
Adrenal tablets
Probiotic tablets
Vit D spray and tablets (5000iu day)
Collagen plus Vit C tablets
Tyrosine tablets
Alpha Lipoic acid
Omega 3 capsules
Biotin (although stopped it a week before the test)
Iron tablets
Magnesium spray
Ferrarin 79.1 ug/l
Folate 13.95
Vit B12 150 pmol/l
Vit D 104 nmol/l
I really wanted to know about the autoimmune side of things because it's the first time it's come up. Why doesn't the NHS acknowledge it and what does it mean for me?
I am on 50mg of Levothyroxine (I take it in the middle of the night). And bloods are done first thing (no food) with the last dose of levo 24 hours before. These results are the recent NHS blood test results:
TSH 0.59 (range 0.27-4.2)
Free T4 14.1 (range 12-22)
Obviously they were only looking at TSH .....which was very low
Now TSH is much higher and Ft4 is rock bottom
On levothyroxine TSH should be at least under 2 as absolute maximum
NHS in its wisdom won’t diagnose on just high TG antibodies, (you can have slightly high TG antibodies due to diabetes or Pernicious anaemia)
But most typical reason is Hashimoto’s
Majority of Hashimoto’s patients either have BOTH TPO and TG antibodies high, or have high TPO antibodies
Significant minority of Hashimoto’s patients only have high TG antibodies and struggle to get Hashimoto’s diagnosed On NHS (they won’t test TG antibodies unless TPO antibodies are high)
Hashimoto's thyroiditis (HT) is the most common form of autoimmune thyroid disorders characterized by lower production of thyroid hormones and positivity to autoantibodies to thyroglobulin (TgAb) and/or thyroid peroxidase (TPOAb).
Elevated TgAb levels are associated with symptom burden in HT patients, suggesting a role of thyroid autoimmunity in clinical manifestations of HT. Based on these results, we recommend screening for TgAb antibodies in HT patients with symptom burden
20% of Hashimoto's patients never have raised antibodies ....ultrasound scan can be helpful
Thanks so so much for all of this. I will have a read of it all. I've never really known much about it. If I get an ultrasound will it definitely confirm I have Hashimotos? I'm paying so much for blood tests so to add this is quite a bit for me. Thanks again xx
But they aren’t really bothered about the cause...they just treat the resulting hypothyroidism
If you were having trouble getting dose increased, you might consider getting one. If scan showed very small thyroid or very damaged it might be useful
Something to consider...one day ....and not in middle of a pandemic
Thank you. I will definitely consider it. As I've been getting muscles aches and also hair falling out etc it definitely maybe a reason. Thanks again x
In my experience my hair really likes T4 and I've also read this in multiple studies. I have gone through many bouts of pretty extreme hair loss but once I started levothyroxine, my hair loss stabilized. I haven't gone through a shed in years now. I take both T4 and T3 slow release. You should go back up to 50mcg T4 and take the T3 on top of it. But you likely need a levo increase as well.
Thank you. I was on 50mg of levo and it made me feel awful and it didn't help with my hair loss either which is when I started taking T3. Plus my GP and endo refused to increase my levo dosage. I've been feeling better too within myself since starting T3. This is the first time that my antibodies had a positive result so my question was more around what that result means and whether it indicates I have Hashimotos x
I only have TG antibodies, no TPO antibodies (never had these), and yes, these antibodies means Hashimotos. My thyroid no longer works at all. Ultrasound shows a heterogeneous echotexture and inflammation. After I had post partum thyroiditis I was able to quit T4 after a couple of years without noticing anything at all because my thyroid recovered when my antibodies disappeared. Antibodies came back at the tail end of perimenopause. However, I recently tried reducing my T4 for 1 week and I felt like death, so went back to 75mcg so thyroid will likely never recover now. You likely didn't feel good on T4 only due to the same reasons I don't feel good on T4 only, we likely don't convert T4 to T3 well. And you may not be on enough meds. The addition of T3 gave me my life back, no more pain, sleep GREAT, no more constipation, no more brain fog, the list goes on. The body needs both T4 and T3, at least mine does and they are finding out that there are more people out there that require this combination therapy. ncbi.nlm.nih.gov/pmc/articl...
Oh wow. I'm so sorry to hear that :(. Sounds rough. But thank you so much for replying. I will check out the article too and get an ultrasound done as I do seem to fit the Hashimotos profile with my symptoms. I may try and increase my levo then and hope for the best. Would it work if I increased my T3 instead of my levo in the first instance in your opinion? Any advice welcome. Thanks again for reaching out xx
T4 is better with the least amount of T3 to make you feel normal. I find I feel overmedicated when taking too much T3. 6mcg T3 had my T3 serum levels steadily climbing over a 2 year period. About a monthafter my T3 levels hit 4.2 (2.6-5.8) I felt VERY overmedicated. I've reduced to 4mcg T3 but may need to go to 5mcg. I'm getting tested again in March. If you read that article, they say the thyroid itself makes about 100mcg T4 and 6mcg T3 per day (for a certain sized person, I need to figure out what that size is), the rest of the serum T3 comes from conversion within the body. I believe if we just replace the amount of T3 that the thyroid would have made if it were working would be enough for me, and in fact, most people. As I'm diabetic I notice a HUGE difference in blood sugar when changing my T3 dosages. T3 makes your peripheral tissues more insulin sensitive, but it does rev up liver metabolism so you need to be careful, this can make the liver more insulin resistant. As long as your T3 levels remain in the middle or slightly above the middle of the range, you should do just fine and your TSH should not (and does not) become suppressed. No matter what they say on this forum, you DO NOT WANT your TSH suppressed. Do some research on the other things that TSH does in the body for your own knowledge. You will then understand why endocrinologists don't want your TSH to be suppressed. Good luck in your journey. If you don't have an endocrinologist, you need one that understands and agrees with T3 supplementation. I found mine by calling pharmacies and asking if they knew of any doctors that were prescribing T3.
My TSH level was between 1 and 1.4 over the last 2 years while on 75mcg T4 and 6mcg slow release T3. This TSH level is where I feel my best.
On the subject of a suppressed TSH - mine has been low on Levo only. In December it was 0.09, and in January 0.14 with T3 4.6 = 40.5% through range. You say the TSH will not be suppressed if T3 doesn’t go above mid-range.I’m not sure how low suppressed is as I’ve read different numbers, so I’m probably not that low (GP certainly thought I was suppressed) but how would you comment on my results?
TSH can become suppressed if you are taking too much T4 or T3 or both. You are likely taking too much T4, if you got a reduction in dose, your TSH will likely go up. Your T4 to T3 conversion may go up as well, the higher the serum T4, the lower the T4 to T3 conversion rate is in my experience. Causes LOTS of pain.
I’m only on 75mcg Levo and certainly don’t feel that I’ve reached full dose yet. My T4 has been gradually going up, from 10 a year ago, which was two points below range, to 15.9=39% through range, so not high. But the point that a high T4 can cause a lower conversion rate is interesting.I’ve just managed to get a dosage increase - to 100mcg - despite my low TSH.
Hmmm, weird. Have you been tested for any other endocrine disorders? Maybe you just don't make TSH due to a pituitary problem? Also, what is the range for your T4? Different assays test very differently. My T4 shows at the top of the range on one assay and middle of the range on another.
Thanks for your reply. The range for T4 was 12-22. I had a blood test at GPs the same time and just discovered the T4 result from their lab was 18 (same blood at same time, same lab range, just a different lab). So one of those results is not quite right.Yes, central thyroidism is a possibility but I’ve never been tested for anything else.
I would believe the higher result at 18 based on your TSH. Your body will get rid of T4 via the RT3 route until you have too much and then you become overmedicated and it will go over range. At 100mcg my T4 still didn't go over range, but I did not feel good. 75mcg with a bit of T3 is better for me. If you're still not feeling better on 75mcg then maybe you need 50 or 62.5 (50 + 25/2=12.5). It takes a LONG time for the levels to build up. It took 3 months of being on T3 before my T3 came up into the normal range, so maybe you are testing too early after a dose increase? If you start feeling even worse with lots of pain on your 100mcg dose you can assume that you are likely over medicated and should then try a reduction to 62.5 mcg. Or you can take 75mcg x 6 = 64.3mcg per day.
Wow, thanks for all this information! A lot to digest but it does seem to make sense. My T3 levels have gone down since I stated taking T3 meds? My Free T3 was 4.05pmol/l in September (to 3.98 now) and I only started the T3 on 1st December. Is that something to be concerned about? My TSH was 1.93 and now it's 2.77. I feel better overral but still not ideal and am obviously worried about Hashimotos now too. Hope you're ok with 2 autoimmune diseases? Poor you. Thanks again for all you help and advice xx
Your TSH is higher because you don't have enough T4 and your hypothalamus /pituitary glands are sensing that. If you have the correct balance of both hormones your TSH will normalize. Your T3 hasn't changed much, so don't worry about that, but you do need more T4. And you're welcome! It's a very complicated balancing act to feel good in this crappy old body, for sure. It also takes time to start feeling normal after taking/changing thyroid hormones. Everytime you change your dose you will feel it and will likely feel crappier before you start feeling better, especially with changes in T3 as it has a very short half life.
Content on HealthUnlocked does not replace the relationship between you and doctors or other healthcare professionals nor the advice you receive from them.
Never delay seeking advice or dialling emergency services because of something that you have read on HealthUnlocked.