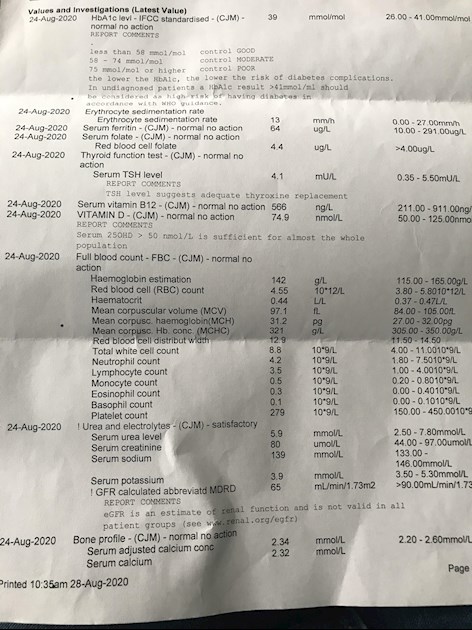
Hi, wondered if someone could help. I was diagnosed hypothyroid about 3 years ago and was put on 50 Levo which I had to fight to have increased to 75 18months ago! I know I’m very hypo again and have attached my latest results from the doctor which has shown an increase in my tsh to 4.1 (it was 1.36 12 months ago) I monitor my own with private blood tests every 6 months and have got high antibodies, indicating Hashimoto’s. I take all the usual supplements as recommended on here, the only thing I’m not is gluten free. My doctor is refusing to up my Levo, even though I clearly need it and to be honest I don’t want to change doctors. I am thinking of asking to be referred to an endo just to take it out of their hands!
My last Medichecks results were in May and they were
Tsh 2.69 (0.27-4.2)
T3 3.55 (3.1-6.8)
T4 13.5 (12-22)
Wondered if anyone could give me any advice how to approach this with the doctor and a decent Endo in the northwest (Wigan area) can’t remember who to email for the list and if you think this is the right approach!
Thank you in advance, can’t go on like this and hold down the job I am doing!
Written by
Tiberess
To view profiles and participate in discussions please or .
You are horribly under-medicated - you must feel dreadful
The aim of a patient on levo is for TSH to be less than 2 (often less than 1) and for free T4 and free T3 to be in the top third (often the top quartile) of the range. You are nowhere near ... your free T4 in May was 11.5% through range and free T3 was 12.16%. So utterly feeble (albeit balanced!)
I think SlowDragon or SeasideSusie may have links etc that you can show your GP
Even though I feel I was treated very negligently by my GP, I at least got a letter from an NHS endo saying my TSH needed to be between 0.27 and 2 when I was diagnosed.
I'm happy to forward my letter to you Tiberess (with my personal info redacted) so you can show your GP.
Here are two articles which may help you persuade your GP to increase your dose:
Dr Toft, past president of the British Thyroid Association and leading endocrinologist, states in Pulse Magazine (the professional magazine for doctors):
"The appropriate dose of levothyroxine is that which restores euthyroidism and serum TSH to the lower part of the reference range - 0.2-0.5mU/l. In this case, free thyroxine is likely to be in the upper part of its reference range or even slightly elevated – 18-22pmol/l. Most patients will feel well in that circumstance. But some need a higher dose of levothyroxine to suppress serum TSH and then the serum-free T4 concentration will be elevated at around 24-28pmol/l. This 'exogenous subclinical hyperthyroidism' is not dangerous as long as serum T3 is unequivocally normal – that is, serum total around T3 1.7nmol/l (reference range 1.0-2.2nmol/l).*"
*He recently confirmed, during a public meeting, that this applies to Free T3 as well as Total T3.
You can obtain a copy of the article by emailing Dionne at
tukadmin@thyroiduk.org
print it and highlight question 6 to show your doctor.
You can also refer to NHS Leeds Teaching Hospitals who say
Thank you and as I said to seaside Suzie above, thank you for all the support you And other admins give to people on here, it really is such a massive help.
Even if we don’t start on full replacement dose, most people need to increase levothyroxine dose slowly upwards in 25mcg steps (retesting 6-8 weeks after each increase) until on full replacement dose
Consider starting levothyroxine at a dosage of 1.6 micrograms per kilogram of body weight per day (rounded to the nearest 25 micrograms) for adults under 65 with primary hypothyroidism and no history of cardiovascular disease.
Traditionally we have tended to start patients on a low dose of levothyroxine and titrate it up over a period of months.
RCT evidence suggests that for the majority of patients this is not necessary and may waste resources.
For patients aged >60y or with ischaemic heart disease, start levothyroxine at 25–50μg daily and titrate up every 3 to 6 weeks as tolerated
For ALL other patients start at full replacement dose. For most this will equate to 1.6 μg/kg/day (approximately 100μg for a 60kg woman and 125μg for a 75kg man).
If you are starting treatment for subclinical hypothyroidism, this article advises starting at a dose close to the full treatment dose on the basis that it is difficult to assess symptom response unless a therapeutic dose has been trialled.
A small Dutch double-blind cross-over study (ArchIntMed 2010;170:1996) demonstrated that night time rather than morning dosing improved TSH suppression and free T4 measurements, but made no difference to subjective wellbeing. It is reasonable to take levothyroxine at night rather than in the morning, especially for individuals who do not eat late at night.
Interestingly, patients with a serum TSH below the reference range, but not suppressed (0.04–0.4 mU/liter), had no increased risk of cardiovascular disease, dysrhythmias, or fractures. It is unfortunate that we did not have access to serum free T4 concentrations in these patients to ascertain whether they were above or within the laboratory reference range. However, our data indicate that it may be safe for patients to be on a dose of T4 that results in a low serum TSH concentration, as long as it is not suppressed at less than 0.03 mU/liter. Many patients report that they prefer such T4 doses (9, 10). Figure 2 indicates that the best outcomes appear to be associated with having a TSH within the lower end of the reference range.
TSH more than 4 causes issues to patients on levothyroxine
In summary, patients on long-term T4 with either an increased serum TSH (>4 mU/liter) or a suppressed TSH (<0.03 mU/liter) have an increased risk of cardiovascular disease, dysrhythmias, and fractures when compared with patients with a TSH within the laboratory reference range. Patients with a low, but not suppressed, TSH (0.04–0.4 mU/liter) had no increased risk of these outcomes in this study.
Igennus Super B is good quality and cheap vitamin B complex. Contains folate. Full dose is two tablets per day. Many/most people may only need one tablet per day. Certainly only start on one per day (or even half tablet per day for first couple of weeks)
Or Thorne Basic B or jarrow B-right are other options that contain folate, but both are large capsules
If you are taking vitamin B complex, or any supplements containing biotin, remember to stop these 7 days before any blood tests, as biotin can falsely affect test results
If your GP remains obstinately refusing to increase dose you will have to go over their head and see a recommended thyroid specialist endocrinologist. Who will write to GP informing GP to keep dose levothyroxine higher and TSH under one
Email Dionne at Thyroid UK for list of recommend thyroid specialist endocrinologists
I have emailed her, didn’t even realise the link with GFR, and just been told I have lichen planus where I’d much rather not have it which I’ve just discovered is linked to hypothyroidism too! How much more things do you need to add to the list before someone listens to you! Feeling very disillusioned with my general practice right now.
It’s quite extraordinary how poor training is on how to treat hypothyroidism .....there are almost 2 million people in the UK on levothyroxine....it’s the 2nd or 3rd most prescribed medication....yet thousands of patients are left woefully under medicated
Levothyroxine doesn’t “top up” a failing thyroid, it replaces it. So almost every patient will need to be on a full replacement dose
Re lichen planus
I have a friend with difficult lichen planus....she was extremely sceptical that gluten free diet would help...but has been very pleasantly surprised
Getting coeliac blood test while still on high gluten diet before trial of absolutely strictly gluten free diet
I have done a coeliac test which was clear but find it so very difficult to see my life without gluten which I know is such a cop out! Really need to give it a go I think!
The predominance of Hashimoto thyroiditis represents an interesting finding, since it has been indirectly confirmed by an Italian study, showing that autoimmune thyroid disease is a risk factor for the evolution towards NCGS in a group of patients with minimal duodenal inflammation. On these bases, an autoimmune stigma in NCGS is strongly supported
In summary, whereas it is not yet clear whether a gluten free diet can prevent autoimmune diseases, it is worth mentioning that HT patients with or without CD benefit from a diet low in gluten as far as the progression and the potential disease complications are concerned
Despite the fact that 5-10% of patients have Celiac disease, in my experience and in the experience of many other physicians, at least 80% + of patients with Hashimoto's who go gluten-free notice a reduction in their symptoms almost immediately.
Content on HealthUnlocked does not replace the relationship between you and doctors or other healthcare professionals nor the advice you receive from them.
Never delay seeking advice or dialling emergency services because of something that you have read on HealthUnlocked.