I've been on 25mcg of levothyroxine for several years. About 9 weeks ago I moved up to 50mcg because of increased symptoms (didn't get a blood test at the time due to lockdown, but just had one and am awaiting results). There are a couple of symptoms I've had for years that I've only recently realized may be Hashimoto's related (LPR and tingling/numbness in hands), so I'm interested in trying a bit of T3 supplementation to see if it helps. The hand numbness has become quite bad lately, too, so feels like some kind of progression is happening. (I used to have tingling/numbness in my chest and feet as well, but magnesium supplements have kept those under control for years.)
Anyway, that's all just background for my question: If I want to try a bit of T3, which is the better choice: add a bit of liothyronine or use NDT? I'm hesitant to try NDT because I don't really want to mess around with my T4 dose at all. So my inclination is to try liothyronine. But would appreciate your advice.
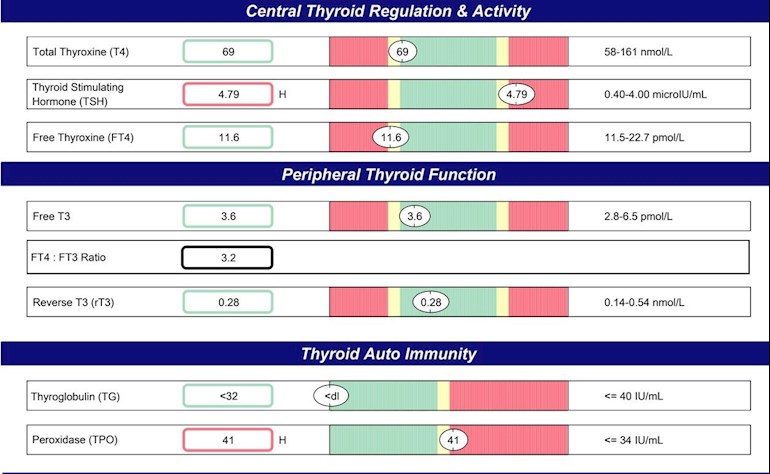
UPDATE: Have uploaded my last test results from a year ago -- see image.
Written by
Gophe
To view profiles and participate in discussions please or .
I think the first thing is to get those blood tests back and post the results. Hopefully you've done the full set - TSH, free T4, free T3, thyroid antibodies, ferritin, folate, vit D and B12.
Chances are you won't need either lio or NDT but just improving some nutrients and possible an increase in levo - you've been on a very very low dose historically - even the 50 mcg which you've been on for a couple of months is really only a starter-dose.
And that would be ideal - given how expensive lio is and tricky to find NDT is these days!
I neglected to ask for folate. They said they'd do antibodies, but I didn't see it on the lab form; and they'll only test TSH initially but apparently will test T3 if my TSH results are off. On the nutrients front, I eat whole foods, no sugar, no caffeine. But my diet's quite restricted due to intolerances and LPR (which I'm now thinking could be caused by Hashimoto's, hence my interest in addressing).
By the way, I'd like to add a screenshot of my lab results from a year ago -- is there any way to upload an image? The doctor at the time said I had Hashimoto's but the lab write-up said I didn't, so I haven't been sure.
UPDATE: Just figured out the image thing; have added to my original post.
UPDATE 2: I didn't change my levothyroxine dose after those results last year. I remained on 25mcg until just 9 weeks ago.
Unless you get your FT4 and FT3 tested at the same time, there is no way of telling if T3 will help you. But, frankly, you're more likely to be under-medicated than anything else. Leaving you on 25 mcg levo for several years is almost criminal negligence on the part of your doctor. It isn't even a starter dose, and should have been increased to 50 six weeks after starting it. And, just testing TSH is totally inadequate. You have been very badly treated so far, and your doctor should be struck off!
But, unfortunately, the NHS is unlikely to test T3 because they don't understand its importance. So, if you want to know the full story, you're probably going to have to do private testing. But, I really would not start taking T3 without having your T3 tested first.
Thanks, greygoose. I did private testing last year -- I've added the results to my original post above. The doc at the time prescribed NDT but he's a generalist (not an endocrinologist) and is quite alternative, so I wasn't confident enough in his advice at the time to make the jump. (The NDT was just one thing on a long list of about 30 things he prescribed me, and I wasn't up for taking 30 things.)
Those results don't show poor conversion, just under-medication. As expected. If your doctor was prepared to prescribe NDT, why was he against increasing your levo? Doesn't make sense.
So, all you probably need to resolve your symptoms is continual six weekly increases in levo until your TSH goes down to 1 or under, and your FT4/3 go up into the upper third of the range. You don't really want to get involved in messing around sourcing - which is expensive and difficult - and dosing T3.
Best not to get the idea that endos are the experts in thyroid. They aren't. The vast majority are diabetes specialists who think they can wing it with thyroid. And most of them are anti-T3/NDT. So, you were probably better off with your alternative GP.
Standard starter dose of levothyroxine is 50mcg (unless over 65 years old).
Bloods should be retested 6-8 weeks after each dose increase in levothyroxine
The aim of Levothyroxine is to increase the dose slowly in 25mcg steps upwards until TSH is under 2 (many patients need TSH significantly under one) and most important is that FT4 is in top third of range and FT3 at least half way through range
NHS guidelines on Levothyroxine including that most patients eventually need somewhere between 100mcg and 200mcg Levothyroxine.
Also note what foods to avoid (eg recommended to avoid calcium rich foods at least four hours from taking Levo)
All four vitamins need to be regularly tested and frequently need supplementing to maintain optimal levels
guidelines by weight might help push for dose increase
Even if we don’t start on full replacement dose, most people need to increase dose slowly upwards in 25mcg steps (retesting 6-8 weeks after each increase) until on full replacement dose
Consider starting levothyroxine at a dosage of 1.6 micrograms per kilogram of body weight per day (rounded to the nearest 25 micrograms) for adults under 65 with primary hypothyroidism and no history of cardiovascular disease.
There is a high (approx 40%) prevalence of B12 deficiency in hypothyroid patients. Traditional symptoms are not a good guide to determining presence of B12 deficiency. Screening for vitamin B12 levels should be undertaken in all hypothyroid patients, irrespective of their thyroid antibody status. Replacement of B12 leads to improvement in symptoms,
you have slightly high TPO antibodies this confirms cause of your hypothyroidism is Hashimoto's, (also known by medics here in UK more commonly as autoimmune thyroid disease).
Hashimoto's affects the gut and frequently leads to low stomach acid and then low vitamin levels
Low vitamin levels affect Thyroid hormone working
Poor gut function can lead leaky gut (literally holes in gut wall) this can cause food intolerances. Most common by far is gluten. Dairy is second most common.
According to Izabella Wentz the Thyroid Pharmacist approx 5% with Hashimoto's are coeliac, but over 80% find gluten free diet helps, sometimes significantly. Either due to direct gluten intolerance (no test available) or due to leaky gut and gluten causing molecular mimicry (see Amy Myers link)
Changing to a strictly gluten free diet may help reduce symptoms, help gut heal and slowly lower TPO antibodies
While still eating high gluten diet ask GP for coeliac blood test first or buy test online for under £20, just to rule it out first
Assuming test is negative you can immediately go on strictly gluten free diet
(If test is positive you will need to remain on high gluten diet until endoscopy, maximum 6 weeks wait officially)
Trying gluten free diet for 3-6 months. If no noticeable improvement then reintroduce gluten and see if symptoms get worse
The predominance of Hashimoto thyroiditis represents an interesting finding, since it has been indirectly confirmed by an Italian study, showing that autoimmune thyroid disease is a risk factor for the evolution towards NCGS in a group of patients with minimal duodenal inflammation. On these bases, an autoimmune stigma in NCGS is strongly supported
In summary, whereas it is not yet clear whether a gluten free diet can prevent autoimmune diseases, it is worth mentioning that HT patients with or without CD benefit from a diet low in gluten as far as the progression and the potential disease complications are concerned
Despite the fact that 5-10% of patients have Celiac disease, in my experience and in the experience of many other physicians, at least 80% + of patients with Hashimoto's who go gluten-free notice a reduction in their symptoms almost immediately.
Thanks, SlowDragon. I didn't know about the B12/peripheral neuropathy connection. I do supplement B12 but maybe not enough. Will see what my latest blood test turns up on that front.
Note: I've been off gluten and dairy for many years , so they're not behind the LPR.
On my levo dosage: When I first tried 25mcg many years ago, I had a really bad reaction, so I went down to 12.5 and stayed there for a long time; blood results were in range. When symptoms increased, I was retested and then went up to 25mcg and next blood results were in range and stayed there for several years. So there was no clear need for an increase.
I don't think I ever took this seriously enough. I didn't realize all these issues I was having could be related to my hypothyroidism until now. Feels like my body's been falling apart and I've just been clueless.
GP should be doing full iron panel test for anaemia
TSH is too high
The aim of Levothyroxine is to increase the dose slowly in 25mcg steps upwards until TSH is under 2 (many patients need TSH significantly under one) and most important is that FT4 is in top third of range and FT3 at least half way through range
Bloods should be retested 6-8 weeks after each 25mcg dose increase
NHS guidelines on Levothyroxine including that most patients eventually need somewhere between 100mcg and 200mcg Levothyroxine.
Also note what foods to avoid (eg recommended to avoid calcium rich foods at least four hours from taking Levo)
All four vitamins need to be regularly tested and frequently need supplementing to maintain optimal levels
Levothyroxine is an extremely fussy hormone and should always be taken on an empty stomach and then nothing apart from water for at least an hour after
Many people take Levothyroxine soon after waking, but it may be more convenient and perhaps more effective taken at bedtime
Many people find Levothyroxine brands are not interchangeable.
Once you find a brand that suits you, best to make sure to only get that one at each prescription.
Watch out for brand change when dose is increased or at repeat prescription.
Many patients do NOT get on well with Teva brand of Levothyroxine. Teva contains mannitol as a filler, which seems to be possible cause of problems. Teva is the only brand that makes 75mcg tablet. So if avoiding Teva for 75mcg dose ask for 25mcg to add to 50mcg or just extra 50mcg tablets to cut in half
No other medication or supplements at same as Levothyroxine, leave at least 2 hour gap. Some like iron, calcium, magnesium, HRT, omeprazole or vitamin D should be four hours away
Physicians should: 1) alert patients that preparations may be switched at the pharmacy; 2) encourage patients to ask to remain on the same preparation at every pharmacy refill; and 3) make sure patients understand the need to have their TSH retested and the potential for dosing readjusted every time their LT4 preparation is switched (18).
Also, I left this off because it didn't seem relevant, but my bilirubin level is a bit high: 29 umol/L with reference range (0-20). Doctor says it means I have Gilbert's Syndrome but that it's usually symptom-less, so nothing to worry about.
I’ll flag these results for SeasideSusie and humanbean to have a look at
Eating iron rich foods like liver or liver pate once a week plus other red meat, pumpkin seeds and dark chocolate, plus daily orange juice or other vitamin C rich drink can help improve iron absorption
This is interesting because I have noticed that many patients with Hashimoto’s disease and hypothyroidism, start to feel worse when their ferritin drops below 80 and usually there is hair loss when it drops below 50.
Yes, I've realized that since finding this group! It's good to finally know what's behind it -- for 4 years I've been experimenting with all kinds of things to find the cause. I'm hopeful that upping my TSH could be the cure. Is that too optimistic?
SlowDragon, since upping my levo to 75 mcg a few days ago, I've been feeling a bit wiped out -- tired/low energy. Any thoughts on why I'd be low energy with higher TSH? A few possible complicating factors: I've been trying to up my ferritin (mostly with black beans) during that same time and have started on a Selenium supplement -- and also just had a period.
Your full blood count doesn't suggest anaemia, so you need an iron panel to see if you have iron deficiency. You can have iron deficiency without anaemia. An iron panel tests serum iron, transferrin saturation, total iron binding capacity as well as ferritin.
You shouldn't supplement with iron tablets on low ferritin alone, if you have a decent level of serum iron already then taking iron tablets could take it too high, and too much iron is as bad as too little.
Medichecks do one, called Iron Deficiency Check, I think it's £39 and can be done by fingerprick. Use code THYROIDUK for 10% discount if it's not on special offer. Fast for 12 hours before doing an iron panel, although you can have sips of water.
SeasideSusie, I've just gotten my back the results of my iron deficiency test. What are your thoughts? (My Ferritin, which was at 18 a week before this test is now at 41.4. Maybe because I immediately started in on black beans, increased chicken, and pumpkin seeds?)
Serum iron: 55 to 70% of the range, higher end for men - yours is 63.75%
Saturation: optimal is 35 to 45%, higher end for men - yours is 37.89%
TIBC: Low in range indicates lack of capacity for additional iron, High in range indicates body's need for supplemental iron - yours is 68.89% through range so around mid-range-ish
UIBC: Low in range indicates that you may have too much iron in your blood which may be due to iron overload syndrome (hereditary haemochromatosis).
High in range signifies iron deficiency - yours is 33.33% through range
Ferritin: Low level virtually always indicates need for iron supplementation; High level with low serum iron/low saturation indicates inflammation or infection - yours is 20.44% through range
Apart from the ferritin, those are very nice results for an iron panel and there is no suggestion of iron deficiency. You already know that there is no suggestion of anaemia so you are left with just low ferritin. To go from a level of 18 to 41.4 in a week is quite remarkable and hopefully not a fluke. I would just continue eating lots of iron rich foods and maybe retest in 3 months. You might want to repeat the iron panel to make sure your serum iron hasn't gone too high and that it's only ferritin that is benefitting from your iron rich diet.
laryngopharyngial reflux -- also called 'silent reflux' (you don't get heartburn -- hence the 'silent', but the acid eats away at your esophagus, so not good long term).
Content on HealthUnlocked does not replace the relationship between you and doctors or other healthcare professionals nor the advice you receive from them.
Never delay seeking advice or dialling emergency services because of something that you have read on HealthUnlocked.