Hi all, hoping for some advice regarding my latest medicheck results as I'm still trying to get to grips with understanding results.
Medichecks suspect Hashi's (I though both TGAb & TPOAb had to have high results for Hashi? If not is my TGAb result worrying as it's in the higher range). I know T4 needs to be in top third and T3 needs to be higher (although I'm struggling to understand T3).
My GP telephoned me back this morning (at my request of trying to obtain an emergency appt to discuss these results), but has resfused to accept I'm under medicated (50mg of Levo since Sept diagnosis). How do I approach him now and take a stand? I'm not naturally assertive and although hubby comes with me to appts for moral support he doesn't understand the results enough to fully fight my corner. Some advice on how to approach this would also be hugely appreciated from you assertive and experienced forum members 😊
PREVIOUS RESULTS
20th Sept 18 - TSH 5.3 miu/L [0.35 - 4.94]
Free T4 10.1 pmol/L [9.0 - 19.0]
29th Nov 18 - TSH 2.5 miu/L [0.35 - 4.94]
27th Mar 19 - TSH 1.7 miu/L [0.35 - 4.94]
25th Apr 19 - TSH 4.4 miu/L [0.35 - 4.94]
10th Jul 19 - TSH 2.9 miu/L [0.35 - 4.94]
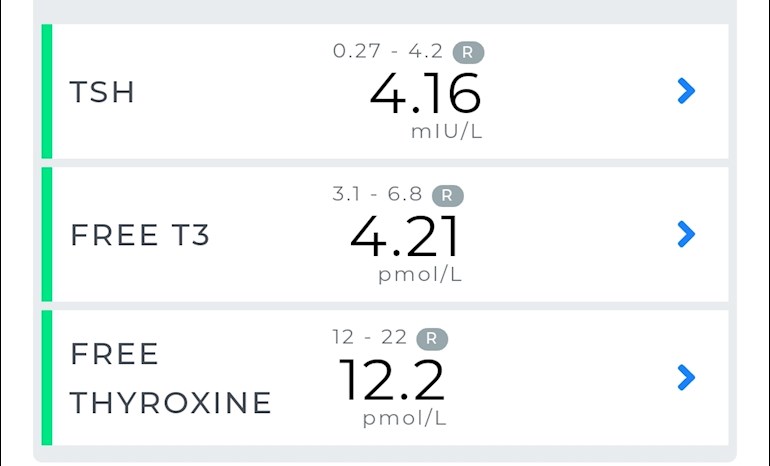
MEDICHECK RESULTS (5th August 2019)
TSH - 4.16 mIU/L [0.27 - 4.2] in range
FREE T3 - 4.21pmol/L [3.1 - 6.8 R] in range
FREE THYROXINE - 12.2 [12 - 22 R] in range
TGAb - 91.2 kIU/L [< 115 R]
TPOAb - 190 kIU/L [< 34 R]
Written by
ILR2019
To view profiles and participate in discussions please or .
I have no idea how to approach doctors, but you're right, you do need an increase in dose. When taking levo, the TSH should come down to 1 or under. Your GP obviously knows nothing about thyroid and believes it's ok if the TSH is just anywhere as long as it's in range. That is just not true.
There is an article by Dr Toft that explains that the TSH should be much lower than yours. Hopefully someone who has that article will reply and tell you how to get it - SeasideSusie , SlowDragon ?
You do have Hashi's. You don't have to have both sets of antibodies high. Your TPOab is well over the top of the range, so you do have Hashi's.
What is it about T3 that you find difficult to understand? Perhaps I can help?
I was hoping yourself and Seaside Suzie would respond with your wealth of knowledge 😊.
My GP said at my last appt that because my TSH was sat 'nicely in the middle of the range' that there was no need for a dose increase I question why my TSH has fluctuated so much and got little more than word salad. He dismissed Hashi's as I had no goiter. Today, he said I had wasted money buying tests online when lab results could not be verified (the results came from Guildford which I believe is a lab also used by the NHS!). When I questioned about TSH being under 1 he said I would risk heart problems by surpressing and this wasn't advisable 🙄
I'm not confused about one particular thing to do with T3 as such just that I haven't read and understood as much about it and reading regularly on the forums I don't understand why some people have T3 only meds or how reverse T3 happens. Im just confused by all the medical references Ive read
Oh dear, he's very ignorant, isn't he. I don't know where they get this idea that mid-range is the perfect place to be, but it rarely is. And, it certainly isn't with TSH, because the ranges are unrealistically wide.
Having a TSH of 1 is not suppressed. And, having a suppressed TSH is not such a bad thing as they imagine. In fact, it's often irrelevant. The TSH itself has no effect on the heart. What is dangerous for the heart is having long-term, vastly over-range FT3 - as in Grave's - which suppresses the TSH. But it's the high T3 that causes the problem, not the TSH. Most doctors seem to get confused with that.
Technically, your doctor is right about the goitre. But, you could have Ord's, which is more or less the same thing as Hashi's, but without the goitre - that's what I have, very high antibodies, but no goitre. These days, we tend to lump them both together and call it Hashi's. Try talking to him about Autoimmune Thyroiditis, he might understand that name better - just means Hashi's. lol
So, T3 only medication… Let me tell you my story. When I was diagnosed I was put on levo only - of course, most people are, and for a good reason - it's the easiest for the doctor to treat with. OK, so, it made me a thousand times worse! I was diagnosed by accident and didn't feel that bad at the time, but once on levo I felt awful! It often happens. With most people they get past that and feel ok. I didn't. Managed to get T3 added and felt better. So, I thought, if it's better with T3, should be even better on NDT - because I'd read the rave reviews! But it wasn't. it was worse than levo only. But, as I had some T3, I stopped the NDT and started T3 only. And, that was the best of all! So, I stuck to T3 only, concluding that T4 in any form was bad for me.
T4 is basically a storage hormone that has to be converted into T3, the active hormone needed by every single cell in your body to function correctly. T4 does have some functions of its own, though, so if you can tolerate it, it's best to have both. And, therefore, I have tried on a couple of occasions to reintroduce T4 with my T3. I can just about tolerate 25 mcg, but if I try to go higher, I feel bad. And, over-all, I prefer no T4 at all. It just does not suit me. And, apparently, there are other people like me, because quite a few of us are on T3 only. But, you do need to try levo first, because it's better if you can have some T4.
rT3... rT3 acts like a break on metabolism, like a safety valve. If you are ill, or injured, or have low ferritin, or high cortisol, or for many other reasons when the body needs to conserve energy, more T4 will be converted to rT3 than to T3 to slow things down. Normally, 20% of your T4 is converted to T3 and 20% to rT3. Both are then converted to T2, T2 to T1, and then the component parts are recycled.
Also, if you are a poor converter, and your T4 rises to somewhere near the top of the range, it will start converting to more rT3, simply to get rid of the excess T4 in a way that conserves the iodine it contains. rT3 is mostly inert, I believe. I have read that it has some function, but I can't remember what it is, and I don't remember where I read it! lol But, basically it is inert and only stays in the body for a couple of hours before being converted to T2. So, the rT3 itself is nothing to worry about, but the cause often is. Hope that makes thing a little clearer.
Wow! Thank you. I have to be honest when I first saw this particular GP I felt very reassured as he was more willing and pro active, even acknowlaging 50mg is a starter dose. Then once I got my results for PA he suddenly changed his mind. I'm so greatful to people like you in these forums. I would have struggled on accepting 'normal' meant normal, but quietly knowing something was amiss.
'Normal' in doctorspeak, just means 'in-range'. They don't seem to understand that it's where in the range the result falls that is important, not just being 'in-range'. The ranges are too wide.
Your results clearly show undermedication - TSH is a fraction below the top of the range, the FT4 is a fraction above the bottom of the range. The aim of a treated hypo patient generally is for TSH to be 1 or below or wherever it needs to be for FT4 and FT3 to be in the upper part of their reference ranges, if that is where you feel well.
Dr Toft, past president of the British Thyroid Association and leading endocrinologist, states in Pulse Magazine (the magazine for doctors):
"The appropriate dose of levothyroxine is that which restores euthyroidism and serum TSH to the lower part of the reference range - 0.2-0.5mU/l. In this case, free thyroxine is likely to be in the upper part of its reference range or even slightly elevated – 18-22pmol/l. Most patients will feel well in that circumstance. But some need a higher dose of levothyroxine to suppress serum TSH and then the serum-free T4 concentration will be elevated at around 24-28pmol/l. This 'exogenous subclinical hyperthyroidism' is not dangerous as long as serum T3 is unequivocally normal – that is, serum total around T3 1.7nmol/l (reference range 1.0-2.2nmol/l).*"
*He recently confirmed, during a public meeting, that this applies to Free T3 as well as Total T3.
You can obtain a copy of the article by emailing Dionne at:
tukadmin@thyroiduk.org
print it and highlight question 6 to show your doctor.
You can also refer to NHS Leeds Teaching Hospitals who say
Thyroxine Replacement Therapy in Primary Hypothyroidism
TSH Level .................. This Indicates
0.2 - 2.0 miu/L .......... Sufficient Replacement
> 2.0 miu/L ............ Likely under Replacement
T3 isn't too hard to understand. T4 is a pro-hormone, T3 is the active hormone that every cell in our bodies need. Our bodies convert T4 into T3. FT4 and FT3 measure the amount of "free" hormone that is measureable in our blood at the time of the test.
TGAb - 91.2 kIU/L [< 115 R]
TPOAb - 190 kIU/L [< 34 R]
Yes, the TPO antibodies confirm Hashi's, and the Tg antibodies are so high in the range that there's no doubt about those either, another test could very well see them over range. But as they fluctuate all the time any test could show them higher or lower.
Thank you so much. I knew you both would help! I'll get emailong now. Im keen to show my GP anything that will help my case. And thank you for the 'Leeds' link x
The aim of Levothyroxine is to increase the dose slowly in 25mcg steps upwards until TsH is under 2 (many need TSH under 1) and FT4 in top third of range and FT3 at least half way in range
NHS guidelines on Levothyroxine including that most patients eventually need somewhere between 100mcg and 200mcg Levothyroxine.
Print out guidelines that SeasideSusie has given you
Take Husband along for moral support and request 25mcg dose increase in Levothyroxine. Bloods should be retested 6-8 weeks after each dose increase
Many people find Levothyroxine brands are not interchangeable.
Once you find a brand that suits you, best to make sure to only get that one at each prescription.
Watch out for brand change when dose is increased or at repeat prescription.
Many patients do NOT get on well with Teva brand of Levothyroxine. Though it is the only one for lactose intolerant patients.
Teva is the only brand that makes 75mcg tablet.
Your antibodies are high this is Hashimoto's, (also known by medics here in UK more commonly as autoimmune thyroid disease).
Hashimoto's affects the gut and leads to low stomach acid and then low vitamin levels
Low vitamin levels affect Thyroid hormone working
Ask GP to test vitamin D, folate, ferritin and B12 as recommended by guidelines
See pages 9 & 13 here on clear guidelines that TSH should be under 1.5 when adequately treated on Levothyroxine and that testing to rule out vitamin deficiencies is required (print out pages and highlight relevant sections...take to these to GP appointment)
Poor gut function can lead leaky gut (literally holes in gut wall) this can cause food intolerances. Most common by far is gluten. Dairy is second most common.
According to Izabella Wentz the Thyroid Pharmacist approx 5% with Hashimoto's are coeliac, but over 80% find gluten free diet helps, sometimes significantly. Either due to direct gluten intolerance (no test available) or due to leaky gut and gluten causing molecular mimicry (see Amy Myers link)
Changing to a strictly gluten free diet may help reduce symptoms, help gut heal and slowly lower TPO antibodies
While still eating high gluten diet ask GP for coeliac blood test first or buy test online for under £20, just to rule it out first
Assuming test is negative you can immediately go on strictly gluten free diet
(If test is positive you will need to remain on high gluten diet until endoscopy, maximum 6 weeks wait officially)
Trying gluten free diet for 3-6 months. If no noticeable improvement then reintroduce gluten and see if symptoms get worse
If your GP refuses to increase Levothyroxine then you will need to go either see different more knowledgable one, or over their head and see an endocrinologist
Email Dionne at Thyroid Uk for list of recommended thyroid specialists
Thank you! I was tested last month for celiac. My IgA was 2.04 g/L [0.65 - 4.21] strangely though I have been saying for a few years that when I omit gluten from my diet I feel better, perhaps that was an early indicator. My Vit D was also tested (45 nmol/L) so I'm supplementing at GP's request. B12 has been low for at least 2 years (as far back as I can go online atm). Tested last month it was 238 ng/L [187.0 - 883.0] and antibodies tests confirmed I don't have PA, but battling with GP about this and folate which was low at 8.2 ug/L [3.1 - 20.0]. Although I don't yet supplement, Im at a loss as to why my vitamins can be low when I eat a healthy diet which includes lots of veg, fruit and salad and little processed food, but am happy to supplement.
My GP said at my last appt that because my TSH was sat 'nicely in the middle of the range' that there was no need for a dose increase
Most healthy people do not have a TSH in the middle of the range, they have a TSH substantially lower than that. The distribution of TSH is not a normal distribution, it is substantially skewed towards the lower end of the range.
See this thread for more details and follow all the links :
The centre of the Reference Range for the test kit used in the study is 2.35. Almost 85% of the healthy population have a TSH reading below this value." [My emphasis]
That is exactly the ammo I need to go to the GP armed with. Fabulous thank you so much. I wonder though, if so many healthy patients need a TSH so low in that normal range why the level needs to be 4 times higher before a GP considers hypothyroidism and if normal is bormal then why labs across the country have different ranges? Particularly considering the research is general.
if so many healthy patients need a TSH so low in that normal range why the level needs to be 4 times higher before a GP considers hypothyroidism and if normal is bormal then why labs across the country have different ranges?
I think it is a combination of poor training, politics, economics, sexism, and sadism.
The political thoughts behind it, from the point of view of doctors, Big Pharma (BP) and the govt are (in my opinion) :
a) Govt and doctors : If we don't treat people we save money.
b) BP : If we don't train doctors to understand the effects of hypothyroidism then we can persuade doctors and patients that sufferers need anti-depressants, anti-anxiolytics, blood pressure medication, statins, diabetes medications, drugs that are alleged to help people with dementia, and we can treat all the effects of nutrient deficiencies without ever actually training doctors that nutrient deficiencies make people feel awful and can (usually) be fixed very cheaply. The money just rolls in.
c) Govt and doctors : Most of the patients are female - and we all know they are attention-seeking, hysterical, time-wasting, wastes of air, food and space, that never stop whinging.
Content on HealthUnlocked does not replace the relationship between you and doctors or other healthcare professionals nor the advice you receive from them.
Never delay seeking advice or dialling emergency services because of something that you have read on HealthUnlocked.

")