Back story. Hashi’s - 10yrs, sometimes good but never been ‘optimal’. Last few months the T4 just doesn’t seem to be as effective.
TSH - 2.1 (0.3-5)
FT4 - 16.8 (9-24)
FT3 - 3.9 (3.5-6.5)
Over the years my FT3 has been 3.9, 3.5, 2.5, 3.9 and 3.8
So this led me to think about conversion so I had the DIO2 test and I have a faulty gene from one parent which MAY have and effect on conversion. I think it’s clear that no matter how much T4 I take (and I’ve always pushed for more) my FT3 just doesn’t even get into the 4’s.
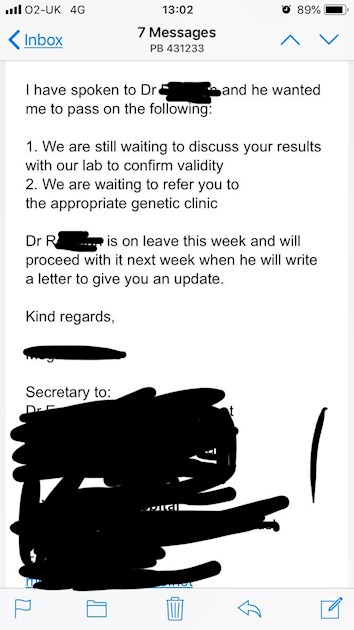
I am now pursuing a private endocrinologist but I haven’t told my NHS Endo. Why would he need to refer me? He is just passing me on so he doesn’t have to deal with me?
I was referred in Nov, I was seen on 14th February (Happy Fecking Valetines Day 😩) and now he wants to pass me along?? I think it’s really appalling!!
