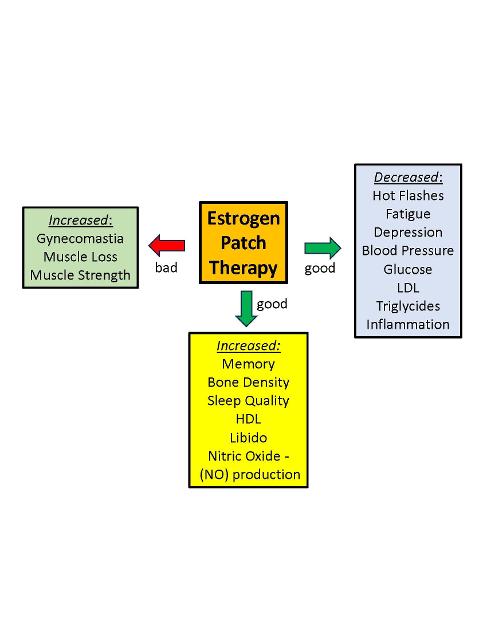
Here's a chart summarizing the benefits and detriments of modern Estrogen Patch Therapy, supported by numerous publications. Overall, the large numbers of benefits outweighs the few negatives.
Benefits of Estrogen Patch Therapy - Prostate Cancer N...
Benefits of Estrogen Patch Therapy
Written by

janebob99
To view profiles and participate in discussions please or .
Read more about...
39 Replies
•
Thanks.....that is great!! Do you have a link to the article that included that graphic? Is the PATCH trial maturing yet? and if so, your thoughts on any early results
Thanks for your questions and comment. I made the graphic myself. Here's an updated version of it, after reviewing it with Prof. Wassersug. He says the PATCH phase-III trial is 1 year behind schedule, perhaps due to one of the lead researchers passing away from Parkinson's Disease. I'm going to post some charts of the Early Results from the Phase I and II PATCH studies. Stay tuned. You can order estrogen gel at Estrogel.com. They will use their own doctor to provide a prescription, which is really nice.
Bob
Transdermal Patch Therapy
Great info again! I've been on Lupron 5.5 years, I have to weigh all that carefully.
I'm going to discuss with MO soon, but he'll probably be reluctant, since not FDA approved.
There are two ways to do transdermal estrogen therapy (Patch/Gel/Creme). One is as an "add-on" with low-dose estrogen where the goal is to bring estrogen levels back to normal baseline levels while continuing Lupron treatment.
The other approach is to do high-dose estrogen to induce testosterone castration levels. With high-dose estrogen, you can replace the Lupron shots with estrogen patch/gel/creme. Most of the bad side effects of Lupron therapy disappear with estrogen therapy. The main side effect of any estrogen therapy is breast enlargement (gynecomastia).
Estrogen therapy was already the Standard of Care from 1950 to 1980 (for ~30 years). Huggins won a Nobel Prize for his discovery of this effect. But, because it was Oral Estrogen (DES) it was discontinued due to a tendency to form blood clots, and replaced by Lupron after Lupron was invented. The new/modern form of estrogen is transdermal (though the skin), which doesn't cause blood clots to form (this has been published in The Lancet by R.E. Langley).
Bob
Transdermal Estrogen Therapy
My MO says "no" because of FDA - where would we go?
Same question here. My MO will be very reluctant.
Here are two suggestions: (1) go to Estrogel.com and they will provide a doctor who will write a prescription for estrogen gel , or (2) tell your MO that you will agree to start Relugolix ADT if your testosterone does not drop below 50 ng/dL (castration) after you start high-dose transdermal estrogen therapy. That's a comprise position (which I plan to present to my MO). Check your testosterone monthly after starting treatment.
Since you can get Estrogel yourself and cheaply, you don't need your MO's approval.
Bob
Yes. I haven't done deep dive on the Patch Trial. Has it shown to be as effective as Lupron over the long term (the outcomes)?
And while keeping your T low, does it actually keep Mets from growing/spreading as effectively?
It has so far but I added Xtandi 80 mg daily after psa started to slowly increase to .6 after two years on just the patches. Since then ( Feb 21 ) psa has stayed at <.1.
I think the fact that my Mets have been oligometastatic (ie only one or two at a time) has surely kept me alive longer even with Gleason 9.
Excellent control. Good work!
How low has your testosterone gone on this regimen?
The best survival outcomes are associated with a Testosterone nadir < 10 ng/dL. I've posted on this recently. The "official" castration level of 50 ng/dL is way too high, according to recent research.
Bob
My T has been steady at <3.0 for years.
Here are two suggestions: (1) go to Estrogel.com and they will provide a doctor who will write a prescription for estrogen gel , or (2) tell your MO that you will agree to start Relugolix ADT if your testosterone does not drop below 50 ng/dL (castration) after you start high-dose transdermal estrogen therapy. That's a comprise position (which I plan to present to my MO). Check your testosterone monthly after starting treatment.
Since you can get Estrogel yourself and cheaply, you don't need your MO's approval.
Bob
Since estradiol is natural and not a drug the FDA isn’t interested in it. And big pharma sure as hell doesn’t want the FDA approving it!
The surgeon that performed my RP last April is an excellent surgeon. Recovery was quick with no complications. Did find the post-surgery care lacking but acceptable.
Was referred to a radiation oncologist for a meet and greet. The meeting with the first radiation oncologist was a complete failure, we did not connect, ended the session after about 15 minutes of the PowerPoint presentation. This triggered that it is up to me to put my healthcare team together.
Had meet and greets with 3 other radiation oncologists and 3 urology oncologists before, before finding ones that 'think outside the box' and are willing to work with me. Refused any LHRH or Relugolix ADT, due to SE, cost and would work with me on estrogen/estradiol as an ADT alternative.
Did start estradiol this month, doctor was familiar with PATCH study and the use of estrogen. Also have postponed adjunct radiation until the results from Signatera test and outcome of estradiol therapy.
One must advocate for their healthcare, do research, find doctors have an open mind, will listen to you, think outside the box and have a compatible personality.
Thank you so much for your courageous story. You are an inspiration!
I'm assuming you are having a rise in PSA from your nadir?
Are you measuring your T-levels? Have they dropped?
Bob
The doctor was not able to get a full 3mm clear border during the RP. There was no cancer found in the seminal gland or any lymph nodes, which was a big positive.
4-month PSA was 0.00, 6 month 0.02, 9 month 0.03. Had MRI with contrast and CT scan in prep for adjutant radiation, no mass or discernable cluster was identified. As my oncologist says, there are a few bad boys still partying. Waiting for the results from the Signatera test and will check testosterone when I go back next week. If all goes well, could be on a monitor every 3 months. Not against the EBRT, but if it can be avoided, one less thing to deal with side effects, urinary and bowel issues, at a point right now they are not a problem. Yeah, my situation is better than a lot of others. Also feel that I have a good understanding of my situation, can have an open and productive dialog with my healthcare team. Not one to take anything at face value, will research and not afraid to ask questions. it is too easy for a doctor to say it is a Standard of Care, which is a general blanket response which may or may not be the best for your personal situation. Same goes for off label use of drugs, and FDA's draconian reaction to some. Too easy for a doctor to say take a LHRH drug and skim over the SE.
Only been on estradiol gel for 3 weeks, have not experienced any SE. My neighbor was on LHRH for 6 months while he underwent EBRT, has been miserable the entire time and has not recovered T level over a year later and is still miserable. He is one of the percentage that will probably never recover T.
From my research, the biggest SE will be getting a pair of girls (which is still a SE for LHRH and Relugolix), can deal with that vs being miserable from SE and foggy brain. Cost was another consideration, a month of estradiol gel is $55 out of pocket vs the several thousand $$$ cost for LHRH and Relugolix, still a lot even if covered by insurance. Besides love not adding to the coffers of the big pharma machine 😁 which is another subject.
Sorry for the long rant, one's healthcare comes down to personal responsibility. The information is available, sometimes not easy to locate and finding a healthcare professional that will not put you in a one size fits all box.
There's a drug to treat gynecomastia -- tamoxifen. Urologists rarely mention that. They treat the disease and not the man so what do they care if you become boobalicious?
Thanks !
I was just reading about that...
Tamoxifen is more effective at stopping Gynecomastia than Radiation Treatment.
Someone said that tamoxifen can interfere with transdermal estrogen therapy. I need to look into that aspect more.
Bob
No need to apologize. It's very helpful information. Thanks for sharing.
Here's a plot of % of men who have recovered their baseline T after stopping Lupron ADT, as a function of time after stopping ADT, for different durations of ADT. You may wan to share this with your neighbor. The rule of thumb for ADT durations less than 20 months is that 50% of men will recover their baseline T in a time equal to their ADT duration. So, if the ADT duration is 12 months, the T-recovery time is 12 months. The curve goes quadratic over 20 months of ADT. For example, for ADT = 36 months, 50% of men recover their baseline T after 5 years of waiting. Yikes! But, that's for 50% of men. There is considerable scatter among the responses, depending primarily on age , baseline T-level, and physical fitness level. Lower baseline T, older age, and poor fitness significantly increases the T-recovery time.
Relugolix is much faster on/off T-recovery than Lupron.
Your neighbor may want to consider adding testosterone replacement therapy (TRT). It's safe and well-tolerated at his point in treatment. He may want to review the papers by Abraham Morgentaler at Harvard, who talks about the safety of doing TRT with prostate cancer.
Thanks for bringing up the cost of these cancer drugs. Estrogel is indeed very cheap. I'm going to add that to my chart of Pros/Cons for high-dose estrogen therapy.
I'm going to consider doing RT of my breasts to prophylactically reduce the chance of gynecomastia (which I already have). I think they can do it in one session.
You might want to consider getting a genetic test to see if you have BRCA 1/2 mutations. Your risk of getting breast cancer goes waaay up if you have those mutations. It's unlikely that you do, however (1/600 risk).
Bob
T-Recovery Time vs ADT duration
My T will never recover because when I tried Lupron vacations I had an immediate increase in psa. So keeping my T at castrate level or below is necessary for me. That’s another reason why switching from an LHRH to the patches is/was vital for me to lead a more comfortable life.
What area are you in? Large city area?
PHX, AZ metro area.
I'm in Albuquerque, NM. Wanted to go to Mayo Clinic, but they wouldn't take my insurance (United Health Care, Medicare Advantage).
I'm going to get SBRT here at the UNM Comprehensive Cancer Center (University of New Mexico). It's a very modern facility, and the doctors are great!
Bob
Thanks. Neighbor is now on T gel, has helped but still has severe SE. Did have DNA test, no BRCA 1 or 2 mutations.
As far as dealing with the girls, that is a wait and see.
Currently BMI is 20.1%, stay as active as possible. I am a high school football officials (both tackle and girls flag), this last season, Aug - Dec, averaged 4 games a week. Do best to stay in shape in the off season. If weight, BMI stay controlled, activity level is kept up, the problem with the girls should be minimized without any meds or other treatments. Otherwise, may need a minimizer 😂.
Good plan. Must be fun referring those games!
I assume your neighbor is on Androgel, which has a very low concentration of testosterone. He may want to dramatically increase the amount he is applying, to get a bigger effect.
I have hypogonadism and I take daily testosterone cream (20% T), which is made by a local compounding pharmacy. It allows me to reach 1000 ng/dL. I wonder what your neighbor's T-level is?
Bob
Nice chart and one with which I agree based on switching from Lupron to the patches in 2019. Added Xtandi in 2021. I’m stage 4 Gleason 9 . Diagnosed in 2013 at age 69. No mets discovered since 2018 ( two bones treated with SBRT). My biggest problem in last few years has been incontinence due I’m told to salvage radiation of prostate bed in 2014.
Sorry to hear about your incontinence. That's rough. I guess you had a lot of radiation to the prostate. That was 10 years ago. I think RT has improved its techniques since then.
How dare you doing on the estrogen patch therapy? How low does your testosterone go? Any bad side effects?
Bob
My T has been <3.0 since starting the patches in 2019. I don’t think IMRT has improved since I had it in 2014. But ensuring you have a good RO team is vital.
Your low testosterone level with Estrogen patches is very impressive! Thanks for sharing that! I'm trying to convince my MO to use estrogen instead of Lupron ADT.
Here's a plot that shows significantly improved prostate cancer survival metric as a function of different testosterone nadirs after Lupron ADT (which should be the same as high-dose estrogen patch castration). Getting below 10 ng/dL has a huge improvement in Survival probability.
Where do you get your E-patches?
Good Work !
bjui-journals.onlinelibrary...
survival plot
Here's the original source data from:
bjui-journals.onlinelibrary...
Survival vs time for different Testosterone Nadir levels
Not what you're looking for?
You may also like...
Disability benefits?
Hi all. Im starting to think of trying to get disability benefits but dont know where to start so...
Which Estrogen Patch dose to use?
This plot shows the median serum estrogen (E2) concentration (in pg/mL) versus total Weekly...
Important caveat regarding estrogen therapy
Prof. Richard Wassersug tells me that estrogen therapy may be contraindicated if you have a BRCA 1...
Benefits of diet and fasting
Had a physical last March, was okay, but Cholesterol again high for over 5th year in a row +245....
Estrogen ADT vs Lupron ADT
Here's a chart showing % of men who have a given condition, comparing Estrogen ADT versus Lupron...