I'm posting this partly just to get it in one place. This info has been discussed before, but now at least I can find it easily as the relevance of VAF comes up often.
I've posted on both of these but got the title of the first study with this image here wrong, it has no proper name, rather it drew from various other Rux studies other than Majic PV.
--
As in prior posts these studies separately found strong correlation of VAF reductions to event free or progression free survival. There is a lot of info in these studies I've posted before. CHR (blood counts) correlates are included. ASXL mutations had clear negative effects. In near all Rux studies pts were HU intol/resistant, this is how Rux is prescribed - a tough audience as I say.
IFN has a large retrospective study that also found benefits for progression.
Written by
EPguy
To view profiles and participate in discussions please or .
I was told that ASXL1 gene gives 20% chance of getting AML. Then there are the wild type -ASXL1 MF and the ASXL1- mutated MF. It also depends on what type of ASXL1 mutation you have, ie. insertion or frameshift. Since my mother also carries this ASXL1 mutation I was also worried a lot so I did read up some research papers. Most studies would say ASXL1 associates with poorer prognosis but it depends on which type, what kind of change, the starting VAF of ASXL, and whether you are responding well to current treatment. What I have learnt so far is MPN is so profile-unique that what is true for one person is not for others and most should be taken for general reference only. Steve from Australia, or @socrates_8 also carries this ASXL1 mutation and he is living to the fullest possible. I take the positive note from him as well as from Steve from USA, or hunter5582
Having said all of these, 20% chance of progressing to AML actually cannot dictate that you are heading down to AML road. The chance of a person getting AML is actually 50%, either you have it or you do not have it. Looking at this perspective, you can see that the stats of 1 in 5 people with ASXL1 mutation will get AML is a lot less.
So please stay positive and hopeful for better future when there are many more drugs are in development now. This is what I tell myself every day
You made some good points Steve, I know some MPN veterans with ASXL1 for a very long time who are doing very well so one shouldn’t jump to conclusions, each case is different and best discussed with a MPN expert who knows the full case history.
I didn’t quite follow where you say 1 in 5 with ASXL1 get AML at some point, then you say the chances of a person getting AML is 50%. This is confusing as 1 in 5 is 20% .
I am always concerned some of these stats maybe out of context and only a snap shot and can scare people unnecessarily although I am certain that is not your intention.
This is what a veteran hematologist, almost considered an MPN specialist here in Viet Nam told me when I consulted with him. He said 1 in 5 people with ASXL1 mutation is likely to develop AML, so that is 20% of one with ASXL might go down to AML. But statistics in MPN, to me, is probably best taken by a grain of salt as how unique each person’s profile is. What one can be certain of is proper nutrition and regular exercise should help tremendously.
My mom has been very disciplined in exercising every day since more than 10 years ago and manage her food intake. I think without it she would not still be here with me today. On the same note, my uncle has passed away recently due to lymphoma non-hogkin type T cell. I recall Steve hunter5582 brother or cousin just finished the chemotherapy treatment and cleared up all the disease. My mother case of PV now MF and her brother case of lymphoma I did trace back and learnt that my maternal grandma once developed some swell lymph nodes in her body and used medicine to treat before giving birth to my mom and uncle. Thus I really think this contributes significantly to cause mutation in both my mom and uncle body, might be even at birth. It is sad that my uncle treatment failed as he was in stage 4b metatasis and T cell is a truly malignant one. Yet Iearnt that having good health without any major disease prior to conceiving and delivering the baby is a true blessing
Regarding to the part where I said the chance is 50%, I should have elaborated more. All the stats are based from large population. Yet when it comes to each individual, it will be the case of either you get the disease or you do not. So the chance, individually, is much greater. When we talk about percentages, it always comes from many point plots, but if you look at each plot point, it can either fall into positive or negative notes. I could have said it is like the Schrödinger's cat experiment. When you open the box, you either see it dead or alive and you wont know until you open the box. Prior to open the box you cannot say for certain if it is dead or still alive. And this is what I mean
Well if that is what you mean I have to say I have no idea what any of that means in terms of "point plots" or "negative notes" and last but not least "Schrödinger's cat experiment". 😊, maybe others do though
I cannot ge t my head around graphs,reminds me of maths at school,I do no know whatASXL is either,think A M L is a Leukaemia,better ask my consultant……Hope you are well with all this going on Lizziep,I try hard not to read about what might happen,French treatment is so different from U K & harder to understand all my results etc. Very Best ,🥰Sally
I wouldn’t assume for a minute that you are destined for AML or anything else based on what you read on here, each case is individual and only a expert MPN doc (eg CH in your case) can give a more accurate view, although I suspect they can’t say for sure either way but certainly a better plan than making assumptions from what posters (me included) write on here. As I said in my reply to Steve and he implied the same many do very well long term with ASXL1. And yes treatments are changing very fast so who knows our long term future. Try not to worry (I know easier said than done) about something you can do nothing about at the moment , if very worried the best person to ask is your MPN expert. 🙂
Thank you, I’m not sure I really want a definitive answer! It is something that is always at the back of my mind, but I try not to dwell on it.
When I was first diagnosed with MF, after having ET for a few years my local haematologist said I’d probably got a couple of years before the MF progressed! (You know why I got in touch with Guys now!) that will be two years in May, so, obviously, that has stuck with me.
I saw a post from someone on a different site today that has MF and the same mutation and is doing well after 6 years.
Exactly, careful about these so called predictions, when I was diag and tortured by itching my Haem at the time said you better get used to it because you will be itching for the next ten years, I said what happens after 10 years and she just well…, kicking up the daises, she didn’t say exactly that, ie kicking daises
Anyway , meanwhile 15 years later and expecting another 15-20 at least and I sorted the itch with UVB then Rux, ie all she told me was wrong.
I think I have said before I know of plenty with MF at 20 years and some with ASLX1, we have to be a bit realistic but very optimistic
The study also shows a pretty high Jak2 starting point for those on Rux. There's some good data which suggests starting Rux earlier is helpful.
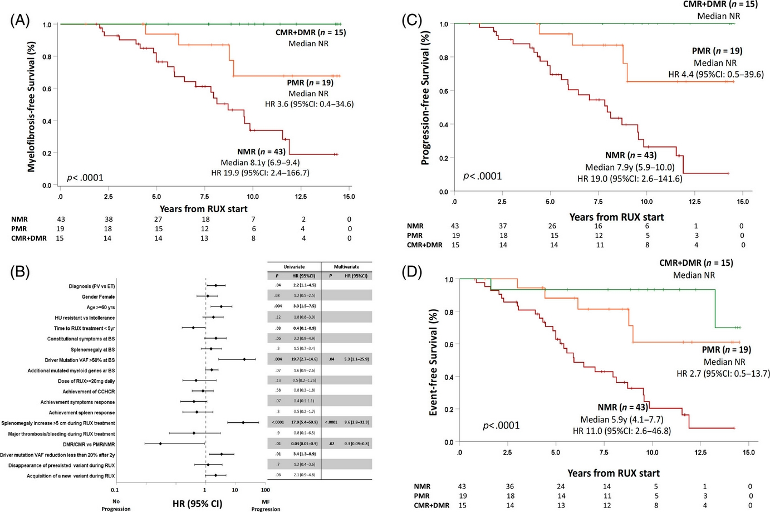
No and partial molecular response (NMR and PMR) had a Jak2 AB starting point of low to upper 70s.
But DMR and CMR had a Jak2 AB of mid to upper 30s. That seems to suggest starting earlier improves chances of DMR/CMR.
Most importantly, if I also am reading the charts correctly, CMR and DMR seem to virtually stop progression to myelofibrosis and even PMR reduces the chances massively. In the NMR group, by year 15, nearly 80% progress to myelofibrosis. But in the PMR group only 20% had progressed to myelofibrosis. That is an astounding difference when compared to PMR.
These are very strong numbers on Rux -Jakafi. I need to read this several more times -thanks for posting -
I made some comments in this thread on these studies. I posted this new one mostly to get the links and titles corrected in one place. But it's also topical these days.
That's a good observation on the better outcomes with lower starting VAF. I hope to review these deeper when I'm more free to do so.
--
Two items to note, from the prior thread:
-These Rux pts were HU intol/resist, which makes the cohort a more challenging set than for most IFN studies that did not select for HU resistance. This HU status follows the Rx rq't for Rux, to have failed HU (and now "or IFN") HU resistant has ~5-7 x higher odds of bad outcomes as in:
-The BAT (comparison therapy) included a large pt group on IFN, rather than just HU. So it was partly a comparison to IFN, but as I noted there does not seem to be enough detail to directly compare these.
These studies are all very interesting. However, as a VAF assay regarded as part of the standard of care for MPNs. I haven't had a VAF study since my initial diagnosis in 2015, and none of my doctors (hematologists or MPN specialists) have ever suggested it. Is it covered by Medicare?
Mutation status and percentage is part of good quality modern care. It was rare in 2015, but more recently we know it has at least some connection to outcomes and we can often do something about it. I understand here you got a result in 2015 but not since. I get it once a year these days, but only because I ask. During my IFN year I got several at my Dr's initiative.
My most recent VAF test was covered my medicare. I'm in a plan G version, maybe that is relevant.
Also worthy is knowing what, if any, other mutations are present. This is NGS, nex gen, that finds as two examples among many, TET2, DNM3TA...
Medicare has covered all my JAK2 Quantitative Analysis labs.
Not all hematologists are checking VAF, yet. I expect it to become standard of care at some pint in the future. Time will tell. My MPN care team has already moved to checking annually at my request.
I may mention VAF at my virtual consultation with my MPN specialist in May. However, I'd like to see a clear statement of the clinical significance of reduced VAF before I push hard for getting it checked.
This is a very good summary of managing PV in 2025 by Dr. Raajit Rampal. The whole thing is worth watching but you can go to minute 38:50 for the commentary on VAF.
The plot at top Figs A and C, are another data set pointing to a demonstrated benefit. Getting to <2% provided zero progression, and getting a 50% reduction provided a still substantial benefit.
This is for Rux, but as I've posted, there is implicit good news for IFN too on the general question whether VAF reductions are useful.
But even if VAF relevance is still debatable, the value of having historical results should still be clear. With future possible treatments targeting VAF precisely, and ever more studies pointing to why we care, it is good to know its past course.
On Incyte's website, the results of the Majic PV study are discussed by two MPN specialists, but no mention is made of any disease progression slowing or stopping benefit from the use of ruxolitinib. The specialists emphasize symptom relief, HCT and WBC count control and blood clot risk reduction: hcp.jakafi.com/polycythemia....
The presentation is an advertisement. We know that because they have the fine print talk at the end. So Incyte, on their site, is limited to claiming aspects of the drugs labeled approval. Mutation burden was not an endpoint and was not part of Rux's approval. So her focus on conventional, and quite important, measures, is appropriate. Same for Bes, but PharmaEssentia tends to push the boundaries in their public statements. Incyte is more by-the-book in public relations.
Dr Harrison did discuss the 2ndary point of Event free survival which includes (major thrombosis, hemorrhage, transformation, and death). This is Fig. 3C above.
Majic PV did find for VAF "... >50% reduction observed in 56% (39 of 70, median FU 48 months) and 25% (14 of 57, median FU 36 months) of ruxolitinib and BAT,".
27% of BAT included IFN, so that is likely where the 25% number here comes from, vs being from HU.
Likewise the waterfall Jak2 plot, Fig. 3A, looks similar to those for IFN. The blue down lines likely include a large portion of the IFN BAT cohort.
Anyway what is the point of this reply?
--
A couple side notes on the talk:
Majic PV was done bec RESPONSE had crossover, so they wanted a cleaner slate.
They could measure the 2ndary endpoint of EFS because there there was no cross over
--
For a VAF study of Rux the first report here may be a best source since it was designed for that purpose and looked thru multiple studies. But no doubt, like most studies, it has weaknesses.
Do a subset of Rux using patients achieve durable Complete Hematological and Molecular Responses, like a subset of interferon using patients do, that enables them to quit the drug for rather lengthy periods of time ranging from several months to a few years?
"Do a subset of Rux using patients achieve durable Complete Hematological and Molecular Responses"
Yes, it's all over this thread if you chose to read it. I just posted that the lowest VAF cohorts are similar for both. But these lowest are a clear minority for both drugs ~20%.
There is anecdotal evidence that a subset of IFN pts can pause or quit, consistent with its deep action. There are no data for Rux, since its ability to reduce the mutation was unexpected and new. And its trials were largely limited to HU intol/resist pts. I may be a case study and the next year or two, I discussed with my Dr. I'll be pleasantly surprised if it works out like that, but I'm always curious.
But more important, this development with Rux is good news for all of us. You should be pleased to learn that your peers have good options that aren't IFN. And these results are good news for IFN too, as it is more support for the VAF benefit that IFN also offers. We want our MPN companions to have options and good news. The terms of service on HUnlocked include " ..in the spirit of supporting and learning from your fellow Users". You have invariably tried to spoil this party, I have no idea where this IFN-or-Bust un-supportive attitude comes from.
--
IFN is an elegant and life altering solution for the cohort that can tolerate it and respond to it. Some MPN pts would like to try or continue IFN but cannot. Others prefer not to risk its uniquely severe sides that earned it the only black box in our common meds. There are sampling of members for whom it has been devastating. How do all these pts feel when you endeavor to denigrate the other potentially safer options?
Please take time to empathize with our members without regard to their choices, and reasons therefore, of medications.
To me it's a matter of common sense that if it were true that a substantial subset (~20%) of Rux using patients achieves DURABLE Complete Hematological and Molecular Responses comparable to interferon, even if they discontinue using it for months to years of time, then this capability would have been discovered years ago by multiple MPN specialists and their patients.
But if Rux does not have durable disease modifying capabilities comparable to interferon then I think it is unethical for Rux enthusiasts to lead others into thinking that it does.
The truth may lie in-between these extremes; i.e. that Rux has substantial disease modifying capabilities, but often not as good as interferon.
Need to get below 10% VAR to get ‘durable progression free survival’ with PEG/Besremi so 2% is a tough ask for Ruxo.
Regarding AB at diagnosis, I was 54% JAK2 in 2016, shot up to 85% in 2018. Started Pegasys and within 2 years reduced AB to about 15-20%.
I also have TET2 and imo the additional inflammation this causes has reduced Pegasys efficacy. This is why I was so keen to try statins. Inflammation is something we should all try to minimise with diet, exercise etc.
My take is that the higher the AB, the more aggressive your version of PV. Normally PV is c. 30 - 40% and MF about 75%.
The good news on that 2% is that, while getting there on Rux or IFN is a minority, but one at least forum member is there (~1%), I'm at 3% on a downward slope (no guarantee it continues) and the bar plot far above (Fig. 3A) shows a signif cohort that got there, no too different from IFN.
Here is the actual data they got at "latest time point avail" in the Majic data supplement Fig. S5. That is a lot of blue dots at or adjacent to -100%. Not too different from IFN.
There are various cutoffs for a special number on VAF, 10, 5, 2, 1 and less show up depending on the study and what is being tracked.
In general IFN has looked better for VAF reductions, but Rux is not that different. Importantly near all the Rux trials selected for HU resist/intol while IFN studies did not. So Rux had a "tougher" audience.
--
Some indirect comparisons, Figs. A and C at top give us the % that achieved 0-2% on Rux, it was 15/77=~20%.
In the ropeg study, ~20% got to <1% VAF at 5 years.
These studies were not intended to be compared this way, but it does show both treatments are not too different on achieving the lowest values, and that both can and do reduce the mutation and can modify disease.
As a reality check, 20% having near full molec response means that 80% did not. If this follows us, 80% of us will not get there on either treatment.
I recall the same TET2 and DNM3TA, among others, can reduce response to IFN, and I assume Rux, but I'm not aware of data on that for Rux. ASXL had a particular influence on the Rux results.
Content on HealthUnlocked does not replace the relationship between you and doctors or other healthcare professionals nor the advice you receive from them.
Never delay seeking advice or dialling emergency services because of something that you have read on HealthUnlocked.