Manouche posted the very new Majic-PV trial.
Some thoughts (sorry it's not better organized, I'm not top of my game these days):
Rux is looking similar to IFN for allele reductions (My Dr sort of said "I told you so")
This like most other Rux studies have been handicapped by selecting for HU intolerant/resistant pts.
More than one study now shows Rux can reduce allele quite well and that these reductions are beneficial. Monitoring VAF is recommended. IFN studies have not made this beneficial connection so clearly (doesn't mean there isn't a like one).
--
Details:
All pts were intolerant or resistant to HC, same as for the earlier RESPONSE trial. It should follow that any responses on Rux are proportionately more impressive vs pts not selected for HU intolerance. The 2nd option, not so selected, is being studied now in the new RuxoBeat trial which seems to show better hematological results so far at 6 months, but not easily comparable.
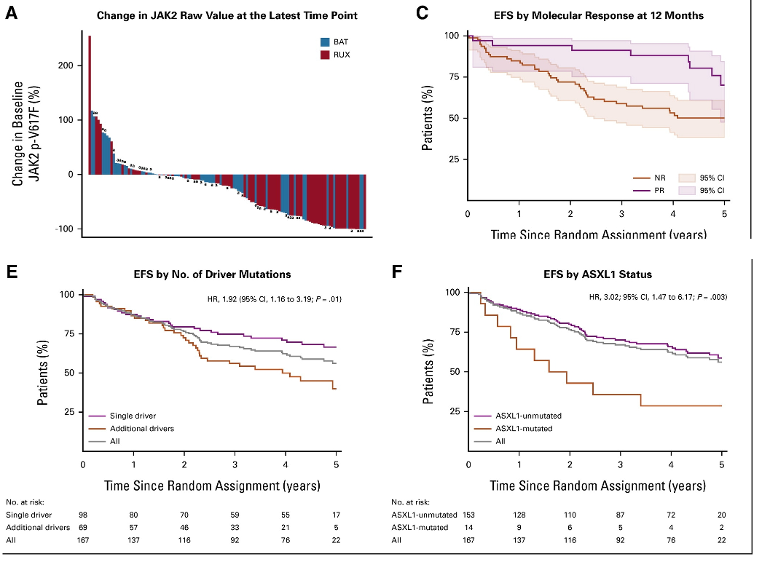
The Figures here show:
A-molecular response. Lots of red pointing down; this is good and indicates Rux is doing well to reduce mutations and is not so different from the equivalent IFN plots, as supported by this note for a separate study:
" Data published from (the earlier RESPONSE) study also suggested that molecular responses can occur (with Rux), perhaps to the same extent as with IFN"
ascopubs.org/doi/full/10.12...
The blue lines pointing down, esp the long ones, could be disproportionately the IFN cohort since HU cannot do this past ~ one year.
B- Getting a partial molecular response (MR) improves event free survival. Interesting to compare to the similar plot for the earlier Rux study in-- healthunlocked.com/mpnvoice...
See plot in replies below. They are indeed similar if you look at the 5 year mark in the prior study. So this result has been reproduced and thus has added meaning, ie getting at least some MR is very useful. This connection has not been studied for IFN that I know of but presumably would be similar. Note in the prior Rux study <2% allele has zero transformations at 12+ years. This MAJIC study did not separate the very best responders.
F- Consistent with prior threads, ASXL1 is a clear added risk. I think I've posted somewhere on possible combo therapies being considered for help with ASXL1.
--
Dose increased from 10mg:2/day-
Ending median dose is 35, equiv to 20+15. Implication is a large dose is needed to get the molecular response, among others.
--
This study is a partial comparison to IFN as BAT, so it's partially Rux vs IFN, but not broken out as such:
In the comparison arm (BAT)
44% had IFN in the mix
10% had Rux in the mix.
But it's a stretch to assume the IFN comparison is suitable with this info as many IFN pts had combos.
