As a lot of you know, I have never had a conclusive, definitive diagnosis, it has always just been an "assumed" or "possible" sjogrens and my second opinion rheumy who my vasculitis doc referred me to clearly doesn't think I have anything autoimmune at all. My RF is through the roof, my ANA's visible but not enough to give a positive result, and my lip biopsy inconclusive. Just recently though, things took a different path and symptoms changed dramatically. Lots more autonomic symptoms than usual and longer lasting, big changes in bowel function, fatigue, appetite, sleeping, dizziness, overheating, headaches, nausea, heart rate, blurred vision and overall just feeling weak and ill.
I managed to get another appointment with the autonomic unit that I saw 5 years ago and who I have previously complained about as not only did they find things in my tests that they didn't tell me about until I later discovered them, but they also refused to recognise that people with autoimmune conditions can and do often have autonomic symptoms that is not necessarily a primary autonomic disease.
They had referred to this as "anxiety".
Eventually, after my complaint, I got an apology and an acceptance that autoimmunity can very much cause people to have autonomic dysfunction without there being any autonomic condition. A victory I thought.
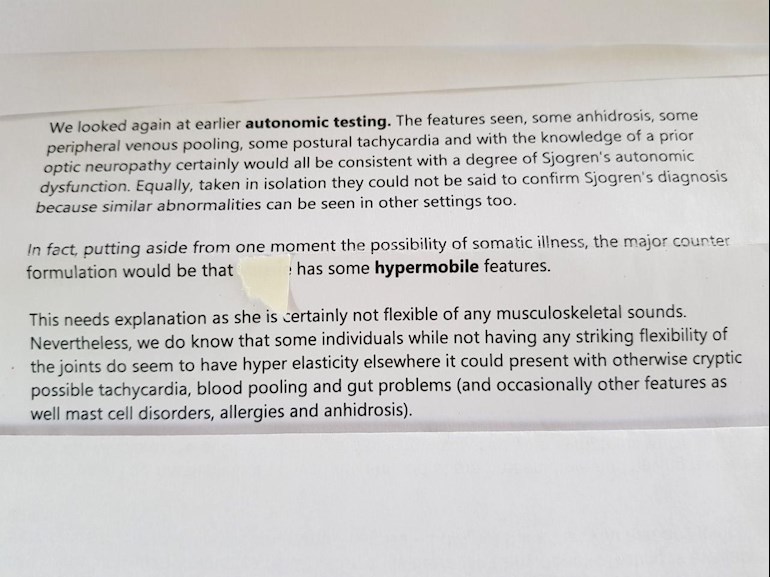
Anyway, at my GP's request, I attended an appointment there again and once again found that they had not given me all my results from my previous testing 5 years ago. I was lead to believe at the time that my tilt and cardiac tests were normal, but I now find out I have a tendency towards POTS, blood pooling and vessel issues and that I am hypermobile. Now, I am the least bendy person I know, but apparently, you can be hypermobile internally without it showing externally. Does anyone know if this is correct? If it is I ask, why do they do the Beighton score to test for it?
(part of letter from them attached)
Now, I can buy into the blood flow thing as I have always thought a lot of my problems were somehow related to blood flow, but the hypermobile bit I am not so sure about.
They went on to mention briefly EDS, SS, Mast cell diseases, Mitochondrial conditions etc and left me totally confused before offering to re do the tilt/cardiac test. I left there with more questions than ever.
Can anyone shed any light on anything? What does this all sound like to you? I know a lot of you have all these conditions, but what stems from what? What comes first so to speak?
I have got a referral to a cardiologist, but what kind of doctor/s would I need to see to confirm or rule out Mast cell things or EDS, Mitochondrial etc? What are the tests for these things?
Thank you all so much for your ongoing support. I would be so lost without you all and this forum. X
Written by
Georgie-girl
To view profiles and participate in discussions please or .
Great post GG! This is good news, i think! Knowledge is power and this info sheds a lot of light on your multisystem manifestations & cormorbidities. Am sure you'll get some great replies, so i’ll try to be brief
Pretty much all of us tend to be a set of overlapping cormorbidities - a bit due to nature & some due to nurture, or all more or less due to both
Looks like you & i have stuff in common:
My 3 primaries are hEDS (hypermobile ehlers danlos syndrome) + infant onset SLE & PID (primary immunodeficiency disease (my version is a type of CVID (common variable immunodeficiency disease)) and the secondaries these primaries have predisposed me to include my Sjogrens, small vessel vasculitis, anhidrosis etc etc
Even basic hEDS & hypermobility generally are thought to be genetic & PID is genetic, whereas the official line is that SLE has been thought not to be genetic, although my paternal & maternal families feature other immune dysfunction & connective tissue disorder conditions and lately one of us here posted about exciting recent research findings indicating there is a genetic basis
Eg My dysautonomia & some of my vascular stuff (eg blood pooling, paroxysmal haematomas etc) & GI tract hyperreactivity + dysmotility etc issues are due to my overlapping imm. dys. & conn. tiss . dis., especially hEDS (MCAD hyperreactivity can be a feature) + PID (MCAD also can be a manifestation) + Sjogrens.
Some of my joints are hypermobile and some less so - i know other hEDS people whose main issues are skin & internal stuff, with no joint involvement. Then there are the totally loose jointed hEDS folk with less internal issues....as with pretty much all our stuff, it’s a spectrum
Here are links to the best 2 UK sources of official info on hypermobility of all types:
Thanks coco. Can always rely on your vast wealth of knowledge to write something informative and extremely helpful. Its all so baffling and I'm at a loss as to where I go next and who I see or what disorder I treat? Does treating the underlying AID take care of the mast cell and hyper mobile stuff or vice versa? Does one cause the other?
I'm so looking forward to reading your links. Thank you X
Oh boy did i feel that way too when i first started getting my head around this years ago...and our wonderful online support group websites + forums have helped me loads to feel less baffled...but research is coming up with news ALL THE TIME so i always keep an open mind....the best experts i know on our types of illness all tend to say there is LOADS they still don’t understand well enough! My fav consultant (a chief immunologist) says caring for patients like us is as much an art as a science! 1 step @ a time: you’ll get answers to your questions 👍❤️
Wow. If they don't understand it, how the hell are we supposed to? Perhaps I need a referral to an immunologist. You are right though. This wonderful forum is such a wonderful source of help and support.
I feel as if my lead clinicians have a pretty good handle on my overlapping cormobidity mix cause their diagnoses are so convincing & their treatments so effective that i’m now feeling better generally than i have since i was a child...but getting here has been a lonnnnng process, involving a lot of collaboration between my medics & me + a lot of advice from my support groups & forums. And the strain our NHS is under doesn’t speed this process up. We need to do our best to gradually understand our cases as best we can & step up to work as our own patient advocates alongside our medics...it’s not easy...it more or less simply ‘is what it is’...this life we lead of managing our manifestations is an on & on thing 😉😘
I agree that it would have to be an immunologist to diagnose MCAD. There are not that many immunologists, at least not in the U.S., who know much about it. It is a very newly understood condition. You are extremely complicated, and I completely understand how you would be totally frustrated. I waited four months to see an immunologist and traveled out of state to see someone. Very glad I did. Ruling things out is important as ruling them in. Wondering why no one told you that you have POTS.
Sounds like you are moving forward. As Barnclown said, there is lots of over-lap. Was that your GP who wrote the letter?
Feel free to ask any questions about the work up for MCAD. Happy to help any way I can.
No Kay, it was the autonomic clinic who wrote the letter. I had this test 5 years ago and was told it was normal. When I got quite ill recently my GP arranged for me to go back to them. That's when I learned of the real results from a different doctor in the clinic .
I completely agree that ruling stuff out is as important as ruling things in but this is all new to me. For the last few years I just thought I had sjogrens, now a whole new can of worms seems to have opened up.
So what is the workup for MCAS? And what is the treatment? Does an immunologist confirm hypermobility too?
Rheumatology can diagnose you on the hypermobility spectrum, but a good GP or expert physio can too. I’ve never heard of immunology diagnosing hypermobility. But if one of the more severe forms of hypermobility is suspected, we tend to be referred for genetic tests. There is an excellent official approved Royal College of GP’s EDS GP TOOLKIT that can help you & your medics with diagnosis. Here is the link:
Also HealthUnlocked EDS Support UK community forum is full of experienced helpful people who know about most aspects of hypermobility inc some with MCADs:
PS my PID immunology team & i have discussed the possibility of being investigated for MCAD in the UK. My impression is that if you need to go beyond v basic prelim testing (eg tryptase blood test) there is 1 UK immunology consultant specialist in MCAD to see. I’ve been thinking about seeing him privately, cause via the NHS will be so difficult....
otherwise patients are investigated at Immunology Allergy clinics, and my univ hosp Imm allergy clinic has refused my referral via gastroenterology TWICE over the past 3 years because , basically, they say they are too busy helping patients with peanut allergies etc etc! Of course this is outrageous, but maybe in immunology depts without a big MCAD expert in staff, specific food allergies take priority over MCADs which so far are less well researched & understood...
Well, in my case the point is: i am in Intestinal Failure partly due to being so hyperreactive in a MCAD-like way to all food stuffs...and here i am after a lifetime of chronic mouth to a*s GI track conditions and the past 5 years of tertiary MDT GI investigations: so far am diagnosed with an immune dys + conn tiss disorder- related GI enteropathy, and for over 1 year have been stuck on prescription Elemental Enteral Nutrition (EEN) with no sign of improved intestinal function & food tolerance (thank goodness my SLE + PID + EEN etc are helping me feel lots better even without food!)
Makes me V worried for any of us with suspected MCAD...
Here is a link to the UK MCAD support group website info re diagnosis:
Mast cell activation is common and possibly necessary for maintenance of survival. Disordered mast cell activation occurs when mast cells are pathologically overproduced or if their activation is out of proportion to the perceived threat to homeostasis. Mast cell activation syndrome refers to a group of disorders with diverse causes presenting with episodic multisystem symptoms as the result of mast cell mediator release. Despite introduction of diagnostic criteria and some advances in treatment in the last decade, many areas of mast cell activation syndrome are in need of research. This article reviews our current knowledge about the various types of mast cell activation disorders, their treatment, and areas of uncertainty in need of future investigation. (J Allergy Clin Immunol 2017;140:349-55.)
You are a star, thank you so much for the great links and expert knowledge. I have so much reading to do now with all these wonderful links I'll probably be missing for weeks. X
Thanks louise. It is so reassuring to know others have, or are being treated successfully for similar things even when they seem to come at you all at once. Its a minefield, but you lot here have far more knowledge than many doctors and I have far more trust in you. I am still on MTX but it just doesn't seem to be helping any more.
I am so sorry you have so much to cope with, but you seem to have kicked it all in to touch. Well done.
I will keep pushing and hope to get some answers eventually. Thanks again X
I see. Well, I can definitely see why your doctors are perplexed and you are confused. One good thing is that your doctors are ruling out mast cell disease. There is actually something called autoimmune mast cell, so it gets pretty crazy.
What tests they do will depend on your symptoms, I think. I will tell you the tests I had: initial testing was tryptase and a few others that I don’t remember but all were blood tests. The immunologist later did blood tests and special 24 hour urine tests for leukotriene inhibitors and other things. Those tests were sent to a special lab at Mayo.
It is important to see someone who specializes in mast cell disease. The guy I went to figured out just listening to me for four minutes that it was not mast cell disease but autonomic dysfunction. Of course, he did all the tests but he is so familiar with the presentation that he could diagnose me right away. He did ask about food allergies, which I do not have, and asked the fellow who was in the room about EDS symptoms. Sounds like you may have food allergies?
You and I pose similar difficulties in diagnosis. I was told it is extremely complicated. Really feel for you. Hang in there. I think they can get to the bottom of this. I am so much better once they figured it all out.
Thank you Kay. You are not kidding when you say it's complicated. Funny enough a GP at my practice mentioned Tryptase testing. He said speak to my GP about it when she is back from her holiday. I assume that's the first port of call? Does this test rule mast cell stuff out or in definitively?
I don't have any food allergies that I am aware of and in fact, I really don't have any allergies at all except certain metals. This one I think was triggered in my younger days when the fashion was large earrings made from who knows what, and apparently, the cheap metal got into my system and now causes a reaction whenever I wear any jewellery that isn't gold or silver. Works well to my advantage at Christmas and birthdays haha. This is the only allergy I have though.
I'm really glad you got sorted out in the end and it's all under control. Hopefully I will get there too. Thanks Kay X
Georgie — impressive that your doctors are already talking about the Tryptase test. As I remember, there were several initial tests and my doctor was thinking of sending me to a hematologist for a bone marrow aspiration. But when I was willing to to go out of state where an expert was, he preferred that route. The immunologist I saw actually developed the Tryptase test.
No, I don’t think the Tryptase test rules out MCAD, but you need to ask your doctor. They might want you to have allergy testing. I had a lot of patches on my back.
I will tell you exactly what my regular dermatologist said to me when I was in for routine cancer screening. The air conditioning went out that day and she walked in to see me with ice packs the nurse gave me. She wanted an update. After hearing, she sat down, put her hand on my arm and said, “I am very sorry you have to go through this. Be patient with your doctors. This is very, very complicated. And we’re just not that smart. It will take some time.”
I think you will get there. Maybe remember what my dermatologist said when you feel down. Your situation is very similar to mine. These mast cell disorders apparently occur more commonly in people with any inflammatory conditions.
K
You maybe do “just have Sjögren’s” GG but Sjögren’s and autonomic dysfunction are joined at the hip with EDS and MCAS as besties of SS. I certainly think this is my combo along with confirmed Hashimoto’s - but like you it’s assumed where I live that mast cells activating and hypermobility are just not worth the paper they were written on. We did have an immunologist here until a few years ago because I met her walking the dogs and got to know her a bit but she got appointed as a fellow at London uni and we lost touch. Don’t know if she was ever replaced.
Yes EDS comes in many shapes and sizes and I’d love to be tested for this and MCAS but can’t see me being referred for testing any time soon. I’d ruled out PoTS because my rheumy referred me for tilt table test which was normal although I’d fractured my ribs a few weeks earlier just where the monitor was strapped and had terrible tooth ache so all I could think about was escaping to the dentist.
My rheum wrote to tell me that all was normal thus excluding autonomic neuropathy. I checked this with my neurologist who looked distinctly uneasy when she reluctantly nodded so I don’t think it’s the only definitive test but could be wrong. I’ve had anaphylaxis 3 times and many unexplained allergies over a life time and my physio and a former Pilates instructor explained I’m hyper-mobile but the CTD doc ran a really unlikely and cursory (and just plain wrong!) version of Beighton on me a month ago and declared my banana knees are just due to loose cartilage?!
As so often we are running in tandem with our symptoms - the ones you list here are also currently mine to a tee. Plus a lot of pain with high inflammation. My rheum is trying to discharge me with “just Sjögren’s” and my GP is resisting on my behalf (and hers I’m guessing!). I have booked to see a rheumy privately on other side of Scotland on Thursday. I hope to ask him about what is relating to “just Sjögren’s” and whether inflammatory arthritis (most likely spondy) should go back on my list. If PsA I’ve read that a normal/ negative RF is one of the diagnostic criteria so this wouldn’t do for you but it would for me. ANA is often positive for PsA so not the same.
Have you ever had your serum tryptase tested for MCAS I wonder? X
Oh poor Twitchy. It must be so hard for you where you are to find the right doctors. It can be tough here at times so it must be awful for you. Could you maybe google to find if there's a decent immunologist not too far away and try getting a referral? I feel you would benefit from that a lot. I really feel for you dear Twitchy.
I too had ruled out POTS as I was told my test from 5 years ago was normal. It wasn't till I went back recently with progressing symptoms (and a complaint along the way) that a different doctor told me it was far from normal and wants to retest.
Also, I don't think a normal tilt test would rule out autonomic neuropathy. I'm not surprised your neurologist looked uneasy. With your allergies etc I would definitely try get a referral to an immunologist if you can and it isn't too far away. That would probably kill a lot of birds with the one stone.
How dare your rheumy try to discharge you with "just sjogrens". There is no "just" about it. You've been through an awful lot. What a cheek and I'm so proud of your GP for fighting it. He can't just leave you high and dry. That made me quite angry when I read that.
We are very similar but you always seem to have high inflammatory markers where as I never do. Once I had a bad chest infection, a tooth abscess and terrible joint pain and yet my ESR struggled to make 7. It just never seems to raise. CRP sometimes raises a little but not much.
Funny you mention tryptase. A GP at my practice just said I need to speak to my GP about a tryptase test when she is back from her holiday. Hope this will give me some clarity.
I really hope you get some answers on Thursday TT and it all goes well. Please let us know and do please try get a referral for an immunologist. X
This area is extremely complicated - as Barnclown says even for the experts let alone the patients! I really struggle to understand it and I am being well treated for a combination of the medical issues you mention. I hope some of what I write might help you.
Barnclown is absolutely correct about there being one particular UK expert immunologist on mast cell issues and to see him you will almost certainly need to go privately. I am one of his patients so please pm me if you would like his name. He runs his private clinics a little like an NHS one ie you are given a date and time and have to pretty much make that. I have followed patients ftom Australia and Spain into his consulting room - patients come from a great distance. One of my other consultants says the imlunologist will not see you unless he thinks it necessary.
A few years ago the definitive tests for Mcas did involve blood and urine being sent to the Mayo Clinic in the US - as Kay mentions. This is extremely expensive, however, I could be out of date and possibly this can now be done in UK. I chose not to pay for Mayo testing as enough came up on my UK based blood tests which meant I could be treated for histamine intolerance/mcad - the treatments are pretty similar. Mast cell stabilisers such as sodium cromoglycate Ketotifen and antihistamines eg Fexofenadine and H2blockers eg ranitadine are used. These are all common drugs used for other purposes as well. If you can consult an immunologist they will probably run quite comprehensive screening tests - mine showed up other problems with my immune system to do with immune deficiency. Again some of these can be treated and some not. Now as well as having some immune deficiency I have developed unspecified autoimmune problems ie overactivity as well as underactivity.
I think it is fair to say if you see an immunologist they help to draw all the loose ends of your medical journey together. Mine works together with my rheumatologist. The rheumatologist prescribed the autoimmune meds eg hydroxychloroquine and pred. In my case my autoimmune rheumatologist confirmed ehlers danlos but I have several extremely close family members with a confirmed Eds diagnosis from different rheumatologists with an specialism in Eds which makes it easier. As Ehlers Danlos is inherited this was important.
Recently to try to narrow down the genes involved in Heds the diagnostic criteria for having Eds has been changed. I believe this is a short term measure but I think there might be a guideline that if you have an autoimmune disease then subsequently being diagnosed with Eds is currently not "encouraged". This probably partly because you are born with Eds but have generally "acquired" the autoimmune problem. In real life it is not as clear cut and many doctors recognise this. It also seems that those with Eds are more likely to get autoimmune problems.
There are few medications bar pain relief to help with Eds. There are more medications to help with Mcad, and autoimmune and Pots.
I have another family member with Pots. He had excellent advice from a specialised cardiologist so if you have an option to go down this route to help your autonomic issues I would take it.
At the moment - again as part of this searching for the genetic base for Heds --the current view is you do need current or historic hypermobility to qualify for Eds. But a few years ago this was less the case and some worldwide experts have questioned the emphasis on hypermobility of joints. When men are diagnosed hypermobility can be less pronounced as testosterone encourages stiffness. It will probably be hard for you to be diagnosed with Eds of you truly have no hypermobility but you could be diagnosed with Co morbid conditions like Pots and Mcad and then maybe back into an Eds diagnosis.
There are forms of Eds other than hypermobility eds which obviously don't require hypermobility but these are less associated with Pots and Mcad.
I hope this helps. In my view it is worth trying to get treated but this area is so complicated and new that it is very difficult to have all your treatment on the NHS. Living near a specialised hospital helps but even so unless your symptoms are very severe the NHS service is limited - perhaps understandably.
I am not sure it matters very much what comes first or what causes what. The main thing is to get treatment and feel better - if possible. In twenty years time probably much more will be known. As my rheumatologist says twenty years ago these syndromes were either not or barely on the radar. It is very cutting edge so in this sense I think we have to be kind to our doctors if they don't have all the answers.
With very best wishes
Pb
Hi Georgie-girl,
I also have a type of EDS that does not present with hypermobility. I have transparent skin, easy bruising, cigarette paper scars, blood vessels fragility and a long list of other symptoms. My sister, my mother, my father and my cousins all have different presentations and I think I have inherited different mutations from both parents, hence the confusing symptoms and difficult diagnosis.
EDS has 13 subtypes (so far), all of them are the direct result of mutations in genes coding for the protein collagen (28 types and a number of variations called isoforms) or proteins and enzymes involved in the processing of procollagens into collagen. They are the most abundant and ubiquitous protein in the human body and their function varies depending on the specific site but generally they provide a net of connections and structure to all other tissues in the body, but also affect their development and normal function.
Being widely distributed complex big proteins makes them particularly prone to act as antigens (mutants) for autoimmune attack, hence the co-morbidity with autoimmune diseases.
Regarding treatments, I’m still trying to figure that out. Most doctors are not clued-up on the basic aspects, not to mention the extremely complex interactions with co-morbidities.
Meanwhile, we try to treat symptoms and not the condition itself, which is basically what we can do regarding genetic disorders.
Thank you Chinchi. You lot here never cease to amaze me with your knowledge. That was really helpful and gave me a much better idea of how this all maybe started. It all made so much sense.
I agree that treating the symptoms sometimes is all we can do but I would still like to know what exactly is wrong if possible. I just find it more helpful to actually have a name or a label even if the treatment is the same regardless. But that's just me. In the meantime I feel I have a long road ahead to get anything definitive diagnosed as it all seems so complicated but I will do my best and with all you wonderful people here for support, I'm sure I will be fine. Thank you Chinchi X
Absolutely, putting a name to the condition is the fist step to seeking reliable information, understanding your symptoms and being able to explain to others why you feel so bad, despite looking 'great'.
I personally think that EDS is under-diagnosed. Giving the fact that many variants will only be diagnosed by very expensive genetic and molecular tests, it's not a surprise that most sufferers stay in the limbo for decades.
Forgot to say... I really like Dr. Peter Rowe's approach to POTS.
Absolutely agree. What type of EDS do you have? I'm wondering if it's the same as I can barely move my thumb let alone touch it to my wrist. All seemed unbelievable at first that you can be hypermobile inside but not out but I guess it's true. That too must lead to a lot of under diagnosis.
I don't have a definitive diagnosis, it's probably a mix of bad skin collagen and bad blood vessels collagen. As I said above, apparently the condition runs in both sides of my family, making things complicated. I have cousins with skin hyperextension (laxity), which I don't have. My Mum had basically the same symptoms as mine. She and alll of her siblings died of vascular issues. My father has hypermobility but never had dislocations. Both have thin, fragile, transparent skin with bad scarring.
I'm still trying to make sense of it all. Mind you, I also have Asperger's Disorder, migraines, chronic allergy (asthma, bronchitis, rhinitis, sinusitis), and peripheral neuropathy (still waiting diagnosis), all made worse since menopause hit me.
Oh my word, what a lot to cope with. Like you, menopause played a big role in my problems. It all seemed to start around the same time. This helped the assumed diagnosis of sjogrens. My daughter's problems started after she had the birth control injections so there is a definite hormonal link here.
Definitely! Have you ever tried hormonal replacement therapy? I tried for 3 months (bio-identical patch Estradot plus bio-indentical progesterone Utrogestan), migraines returned with a vengeance and had suicidal ideation. No way...
Good grief. No I never tried it. Rheumy said I could only have progesterone HRT, no oestrogen so it didnt seem worth it as oestrogen was what I seemed to need. I didnt have that many problems with it though to be honest. My problems was the autoimmune thing starting.
Oh my word Pussbella, what knowledge you have. It was like speaking to a qualified doctor. Thank you so much it has helped immensely. To be honest, all this complicated stuff just makes me want my sjogrens back. It was so much easier just blaming everything on that.
How on earth do you have an overactive and underactive immune system? That's bizarre. How do you begin to cope with that? I notice you take just hydroxy and pred and that made me think perhaps I should stop the MTX?
I completely agree I should try to see an immunologist and in the first instance I think perhaps local as we do have a couple of relatively good ones at my teaching university hospital and then perhaps a private one after if I haven't got anywhere.
I was told by another doctor at my surgery, (my GP is on holiday) that I should speak to her when she returns about a tryptase blood test? Is this something you had initially?
I am pretty lucky in that I have lots of tests lined up at different clinics, but can't help feeling I'm going round in circles by seeing the wrong doctors.
Funny enough my daughter who has a UCTD started having autonomic issues and faints and her rheumy has referred her for hypermobility testing so there is definitely a link here. She though has bendy joints where as I don't.
For now I think it's one day and one doctor at a time and hopefully I will get there in the end. Thank you again for your wonderfully helpful response. X
There are several of us here on forum with simultaneous overactive & underactive immune systems....including dear Shaista (of the Lupus in Flight blog, our jimbo’s wife pooh bear, lou & me. In cases like ours, our lead clinicians are heads of both rheumatology & immunology immune dysfunction clinics.
This has been a great discussion GG! Am so glad you posted ....and i hope you’ll let us know how things go for you & your daughter 🍀❤️🍀❤️
I'm so confused how anyone can be over and under active at the same time but there you are, living proof. Once you have an auto immune condition, which causes over activity in the immune system, how do you later discover you have an under active one?
Of course I will keep you posted.
I so love this forum and all the wonderful people.
GOSH...good question...i’ll have a go at answering, but have a feeling this is more than i’m capable of...
my simultaneous immune system overactivity & underactivity were both v early onset, and both were diagnosed based on blood test results + clinical examination + medical history. But my lupus was diagnosed first & then that diagnosis got lost for 40ish years. While my PID diagnosis only finally happened a few years ago. As you know, it’s v common for both types of immune dysfunction to go unrecognised for a lonnnng lonnnng time
As i understand it, my infant onset primary autoimmunity (SLE) would probably be more severe if i hadn’t also been born with immunodeficiency (PID) ...eg my autoimmune disease is seroneg because my immunodeficiency disease prevents me from being able to make antibodies. And because i can’t make antibodies, my autoimmunity inflammatory process has had to use up my lymphocytes & complements instead. Meanwhile my immunodeficiency has meant i constantly have had what immunology calls complex persistence pattern multisystem infections & chronic pockets of bacteria driven sepsis. So these 2 types of immune dysfunction have operated in distinctly different ways with different effects on my bod
And the differences between AID & PID treatment plans goes someway to showing how distinct these 2 types of immune dysfunction are - my PID means i need to take daily antibiotics + have 3 weekly IVIG all the time in order to protect me from infections. My AID means i need to take immunosuppressant meds + steroids. Neither rheumatology or immunology see anything contradictory about my needing both types of treatment plans day to day forever
And then there is this: my version of PID doesn’t seem to me as severe as the PID of other patients i know. And likewise, my ‘moderate’ SLE doesn’t seem to me as severe as the SLE of other patients i know. So i figure my combo of under active + overactive immune dysfunction has always been somewhat cancelling out each other’s intensity....thereby reducing the severity of my case of immune dysfunction generally
Also, my rheumy helpfully first described my immunodeficiency to me as “a bone marrow disease”...which makes me think of my immunodeficiency as something quite different from my autoimmunity.
Hope something in there makes some sort of sense...have never before tried to explain this to anyone! On my PID forums, more knowledgeable patients explain this much better. There are quite a few cases of simultaneous immunodeficiency & autoimmunity on my PID forums, which kind of means this combo no longer seems so weird to me
Yes I am. I think he's wonderful on so many levels but not on others. I was diagnosed with internal hypermobility but he wont accept that you can be hypermobile inside but not out. He's also not really buying into the mast cell thing. Maybe he's right, I dont know but so many doctors have such conflicting views it's really difficult to understand anything.
It is hard to understand! You may be similar to me. Are they trying to figure out if your issues are Sjogren’s nerve-related or mast cell/EDS related? I was told this is very complicated. Like you, my tilt table test was positive. I had other strange hypersensitivities and they wanted MCAD rules out. I saw an immunologist who knew right away I didn’t have mast cell disease. Why does Dr. Kaul think it is not mast cell related? Things like this are not black and white. It could be your order symptoms are not consistent. I would want to know his reasoning. As a rheumatologist, his opinion counts with the EDS diagnosis. I know how difficult it is when doctors are speculating because there are no definites.
Yes, it sounds like I'm very similar to you. One doctor is adamant its sjogrens and another dismisses it completely. Dr Kaul seems to think you cant be hypermobile on the inside without having it show in the joints. Other doctors say you can have it in the gut and connective tissues but arthritis could mask otherwise flexible joints. As for MCAS, his reasoning was that it's just very hyped and so much overlap into other things that it's not worth testing for. And even if we did, it doesn't usually confirm anything, just leaves more questions. The thing is , although my RF is through the roof, my ANA's are always borderline so its believed by some doctors that my sjogrens is not bad enough to cause all these symptoms.
Maybe I'll get definitive answers eventually, who knows? In the meantime we struggle on.
Well, he could be right. The guy I went to also said it is being over-diagnosed now. He developed the tryptase test and has researched mast cells for thirty years. Feel free to message me. It is a hard diagnosis because the doctor has to be familiar with the presentation. You might want to see an immunologist for your peace of mind. Does Dr. Kaul think you have Scjogren’s? Maybe he thinks, as my doctors concluded, that my autonomic dysfunction is likely autoimmune related. I have Sjogren’s antibodies and those were re-tested.
At least, Georgie, our autonomic issues are being studied intensively. Lots of research is taking place.
Well apparantly I have POTS which causes a lot of autonomic symptoms so I guess its 6 of one and half dozen of another. Dr Kaul thinks I have mild sjogrens and PMR but not enough to cause all my symptoms. He isn't sure at this point what is causing them.
Still, as you say, we are being studied intensively.
Yes, POTS is a form of autonomic dysfunction. I think they will get to the bottom of this eventually. You should feel better when your POTS is treated, for sure.
Good luck with all of this. I know it is taking a long time.
Content on HealthUnlocked does not replace the relationship between you and doctors or other healthcare professionals nor the advice you receive from them.
Never delay seeking advice or dialling emergency services because of something that you have read on HealthUnlocked.